
Abstract
Background
Colonic abnormalities, ranging from benign haemorrhoids to malignancies, pose a significant global health burden. Despite extensive research in Western populations, regional data from Saudi Arabia remain limited.
Objective
To evaluate the prevalence, demographic trends and clinical relevance of colonic abnormalities in a Saudi Arabian population.
Methods
This retrospective cross-sectional study analysed 2523 colonoscopy reports from Al Noor Specialist Hospital, Makkah, Saudi Arabia, between 1 March 2010 and 30 December 2020. Reports were examined for key findings, including polyps, tumours, bleeding, diverticulosis, haemorrhoids and inflammation. Statistical analyses were used to assess age- and sex-specific trends.
Results
Haemorrhoids (38.1%) and polyps (12.2%) were the most frequent abnormalities. Polyps were most common in patients aged 50–59 years. Sex differences were significant; men showed a higher prevalence of haemorrhoids (p < 0.001) and active bleeding (p = 0.04), while women exhibited a higher prevalence of ulcers and erosions (p < 0.001). Older patients exhibited a higher prevalence of diverticular disease and bleeding; younger individuals (20–39 years) had higher rates of inflammatory changes.
Conclusion
Colonic abnormalities were prevalent in this Saudi population, with distinct age- and sex-specific patterns. These findings support the need for tailored screening strategies. Future multicentre studies should explore the effect of genetic, dietary and environmental factors on colonic health in the study region.
Keywords
Introduction
Colorectal conditions, ranging from benign abnormalities such as haemorrhoids and diverticulosis to potentially life-threatening malignancies, represent a significant global health burden.1–3 Colorectal cancer (CRC) is the third most diagnosed cancer and the second leading cause of cancer-related deaths worldwide.1,4 CRC accounted for approximately 1.9 million new cases and 935,000 deaths annually in 2020.4,5 Polyps, a precursor lesion for CRC, are detected in 15%–40% of colonoscopies depending on population characteristics, emphasising the importance of early intervention.6,7 Additionally, non-neoplastic conditions such as diverticular disease and gastrointestinal bleeding significantly impact morbidity, particularly in older populations.8,9 In Saudi Arabia and the broader Middle East, CRC has emerged as a growing health challenge, with recent data showing an increase in incidence rates, particularly in younger populations.10,11
Colonoscopy is the gold standard for diagnosing and managing a broad spectrum of colorectal conditions. 12 Its dual role as a diagnostic and therapeutic tool enables the detection of early-stage CRC and the removal of pre-cancerous polyps, thus preventing progression to malignancy.7,13 Furthermore, colonoscopy is critical in diagnosing rare conditions, including vascular lesions, inflammatory disorders and advanced tumours, providing invaluable insights into gastrointestinal pathology. 7 Despite its proven efficacy, access to colonoscopy and utilisation rates remain variable across regions, with significant disparities in screening and diagnostic services observed between high-income and low- and middle-income countries.14,15
The prevalence and patterns of colonic abnormalities are significantly influenced by demographic factors such as age, sex and geographic region.5,16 Globally, CRC incidence rates are higher in males than in females, with age-standardised rates of 86.1 per 100,000 males and 56.9 per 100,000 females in the UK in 2014. 17 Age is a critical factor, with most CRC cases diagnosed in individuals aged >50 years.7,8,18 Additionally, recent studies have reported an increasing incidence of early-onset CRC in individuals aged <50 years, mainly in high-income countries.19,20
In Saudi Arabia, CRC has become the most commonly diagnosed cancer among males and the third most common among females. A comprehensive analysis of data from the Saudi Cancer Registry between 2001 and 2018 revealed a 335.6% increase in CRC cases, with the age-standardised incidence rate rising by 152%. The median age at diagnosis was 60 years for males and 58 years for females. 11 Despite these trends, further region-specific data must be collected on the prevalence and patterns of other colonic abnormalities, such as polyps, diverticular disease and haemorrhoids, in Saudi Arabia and the broader Middle East.
Age- and sex-specific trends in colonic abnormalities have been well-documented in Western populations. For instance, a study analysing colonoscopy data from a community-based sample in the United States found that the prevalence of right-sided colonic polyps increased with ageing and was higher in females. 21 However, similar comprehensive studies need to be performed in Saudi Arabia and the Middle East. 1 This gap in knowledge limits the ability to develop targeted screening and prevention strategies tailored to the demographic characteristics of these populations. In Saudi Arabia, studies have highlighted an increasing demand for colonoscopy as the incidence of CRC rises, particularly in individuals aged <50 years, a trend mirrored globally.1,22 However, regional data on the prevalence and demographic patterns of other colonic conditions, such as diverticula, haemorrhoids and inflammation, remain limited.1,16 This is concerning, given the role of lifestyle factors, dietary habits and healthcare accessibility in shaping gastrointestinal health.23,24 While global studies have emphasised age- and sex-specific variations in colorectal abnormalities,25,26 such data are sparse in the Middle East, highlighting the need for tailored screening and management strategies for populations in this region.4,18
This study can enhance clinical decision-making and improve gastrointestinal health outcomes in Saudi Arabia and beyond by addressing the regional knowledge gap and providing novel insights into the epidemiology of colonic conditions. Addressing this gap is crucial because understanding the demographic variability in colonic abnormalities can inform healthcare policies and resource allocation. Therefore, conducting region-specific research is essential to provide a clearer picture of the epidemiology of colonic abnormalities in Saudi Arabia. This study aimed to assess the prevalence and demographic distribution (by age and sex) of colonic abnormalities reported in colonoscopy procedures over a 10-year period. It also aimed to inform region-specific screening practices and enhance the understanding of common and rare endoscopic findings in the Saudi population. The study was conducted using archival materials obtained from patients who underwent colonoscopy at Al Noor Specialist Hospital in Makkah, Saudi Arabia, over 10 years. This research is particularly important given the recent global emphasis on early detection and prevention of colorectal disease. Additionally, it seeks to identify age- and sex-related trends and risk factors for significant conditions, thereby informing strategies to optimise screening and preventive care in the region.
Methodology
Study design and population
This was a 10-year, cross-sectional, retrospective analysis conducted at Al Noor Specialist Hospital, Makkah, Saudi Arabia. The analysis included all patients who underwent colonoscopies between 1 March 2010 and 30 December 2020. Data were acquired from the archival database between September and December 2020 from Al Noor Specialist Hospital, Makkah, Saudi Arabia. The study size (n = 2523) corresponded to all eligible cases over the 10-year period. It was not calculated prospectively due to the retrospective nature of the study. This study followed the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines for reporting observational studies. 27
Data collection
Data were retrieved from the Al Noor Specialist Hospital medical record archive. Eligibility criteria included all patients who underwent colonoscopy at Al Noor Specialist Hospital between 1 March 2010 and 30 December 2020 and had complete procedural documentation. Patients whose reports lacked findings due to early termination were excluded. The dataset included demographic information such as patient age, sex and nationality as well as detailed colonoscopy reports. These reports were systematically reviewed to extract specific findings and conditions relevant to the study. The primary outcomes were the presence and type of colonic abnormalities. Predictors included patient age and sex. Quantitative variables such as age were grouped into 10-year brackets (e.g. 20–29 and 30–39 years) based on clinical relevance and distribution. No independent assessment of exposure was included because data were drawn from pre-existing colonoscopy reports. To minimise selection bias, all eligible reports were included. Although reporting bias may exist, only documented findings were analysed to ensure consistency. Colonoscopy reports were examined for key findings using a predefined list of keywords corresponding to clinical terms (e.g. ‘polyps’, ‘diverticulosis’ and ‘ulcers’). The reports were manually reviewed for consistency.
The findings were included as documented in the endoscopic reports, without reinterpretation or classification beyond what was explicitly reported. For example, terms such as ‘cobblestone appearance’ were recorded without attributing them to Crohn’s disease (CD) unless explicitly stated. Future studies integrating clinical and pathological data could enhance standardised classifications. The conditions analysed from the colonoscopy reports are summarised in Table 1, and each condition was categorised and statistically analysed to identify demographic and age-related patterns.
Conditions analysed in the study.

Data analysis
Statistical analysis was performed using SPSS version 28 (IBM Corp., Armonk, NY, USA) and Microsoft Excel (Microsoft Corp., Redmond, WA, USA). Descriptive statistics (mean ± SD, frequencies) were used. Chi-square tests were used to assess group differences. Nominal regression was used to identify predictors of abnormalities based on age and sex. Clustering analysis was used to explore pattern similarities among subgroups. Quantitative variables such as age were grouped into 10-year brackets (e.g. 20–29 and 30–39 years) based on clinical relevance and distribution. Reports with missing relevant findings due to procedural incompleteness were excluded. For complete reports, the absence of a documented condition was presumed to indicate its absence. Missing data were not imputed; cases lacking documentation were excluded. No sensitivity analysis was conducted due to dataset limitations.
Ethical approval
This study was conducted following ethical guidelines and was approved by the Committee for Research Ethics for the Health of Makkah Region, Ministry of Health (H-02-K-076-0103-268). It was conducted in accordance with the ethical principles of the Helsinki Declaration of 1975, as revised in 2024. The ethics committee waived the requirement for individual patient consent because this was a retrospective study involving archival data. All patient data were anonymised to ensure confidentiality and compliance with ethical standards.
Results
All included records (n = 2523) represented completed colonoscopy procedures. Records with incomplete documentation were excluded, and no follow-up was conducted. Participants’ demographic data included age, sex and nationality. Additional confounders were not available in the dataset. No adjustment for confounding was performed due to the descriptive nature of the dataset. No sensitivity analyses were performed because we used a retrospective, fixed dataset.
Age and nationality were also assessed as predictors. Although age showed a borderline association with sex (p = 0.060), the effect did not reach statistical significance, indicating that age distribution across sexes was relatively balanced. In contrast, nationality demonstrated a significant association with sex (p < 0.001), although this may reflect sampling biases or demographic characteristics rather than clinically meaningful differences.
These findings highlight key sex-specific differences in colonic abnormalities and suggest potential areas for tailored clinical interventions. The significant association of vascular and inflammatory conditions, such as angiodysplasia and ulcers, with specific sex underscores the importance of individualised screening and management strategies to address the distinct needs of male and female patients.
Predictors of sex differences in colonic abnormalities
Nominal regression analysis was conducted to identify predictors of sex differences in colonic abnormalities among 2523 patients. The final model showed significant improvement over the intercept-only model (−2 log likelihood = 1012.009, chi-square = 206.724, p < 0.001) and explained 6.0%–10.6% of the variance in sex classification (Nagelkerke = 0.106, McFadden = 0.060). Males were significantly more likely to present with internal haemorrhoids (41.2% vs. 20.7%, p = 0.005) and angiodysplasia (p = 0.046). Females had significantly higher rates of ulcers and erosions (p = 0.001), consistent with the descriptive prevalence observed in the dataset, where ulcers and erosions occurred in 1.6% of females compared with 0.6% of males. Adhesions causing obstruction were observed exclusively in females (three cases, p = 0.023). Common findings such as polyps (p = 0.409), external haemorrhoids (p = 0.639) and active bleeding (p = 0.300) were not significantly associated with sex. Rare abnormalities, including fungating tumours and anal masses, showed no sex-specific trends, likely due to their low prevalence. These findings underscore distinct patterns of colonic abnormalities between males and females (Tables 2 and 3).
Frequency distribution of colonic conditions identified in colonoscopy reports.
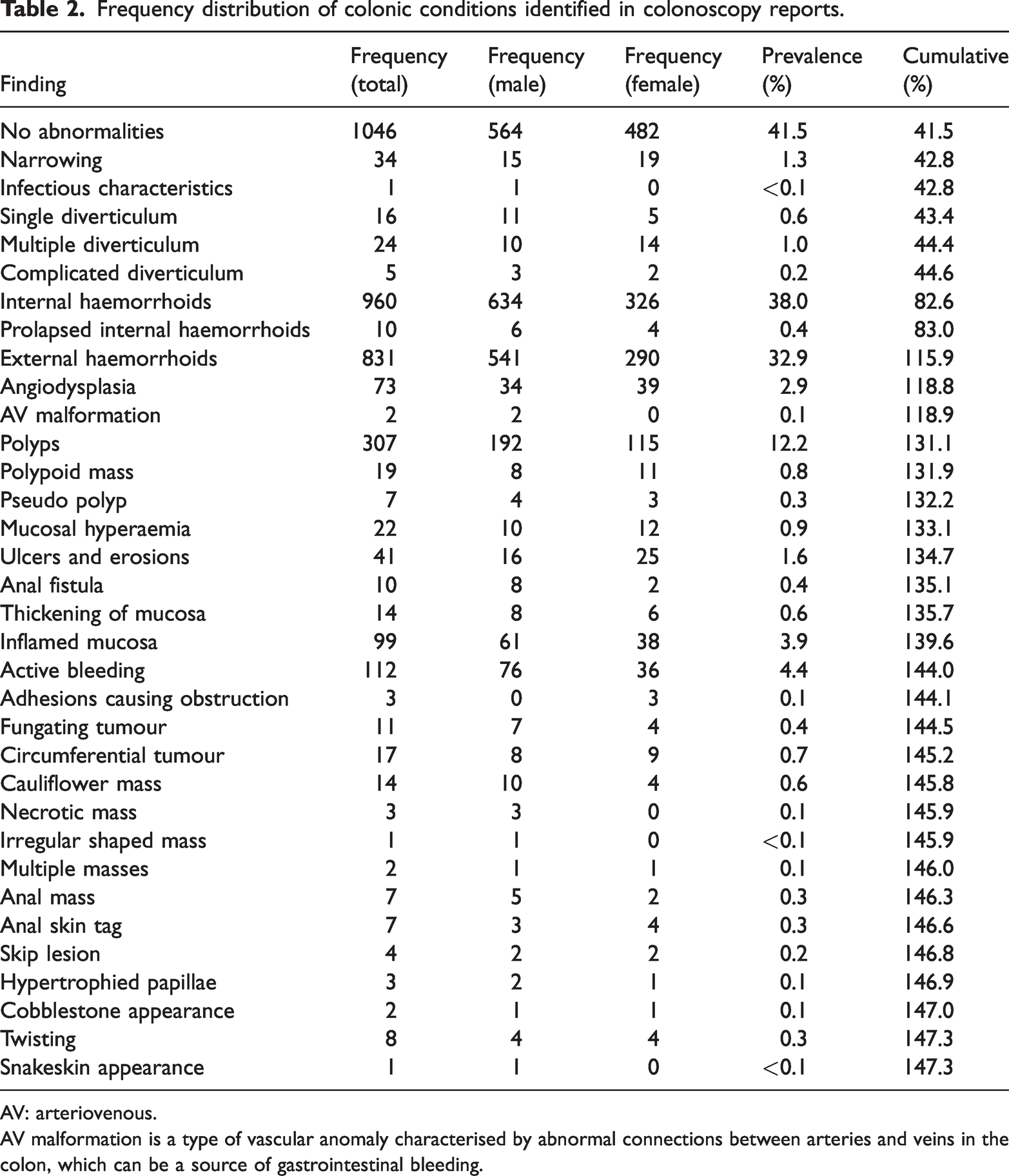
AV: arteriovenous.
AV malformation is a type of vascular anomaly characterised by abnormal connections between arteries and veins in the colon, which can be a source of gastrointestinal bleeding.
Nominal regression analysis of sex-based differences in colonic findings.

OR: odds ratio; CI: confidence interval.
In total, 2523 colonoscopy procedures were analysed to assess the distribution of findings across sexes, revealing both common and rare abnormalities and statistically significant sex differences (Table 2). Among the findings, the most frequently reported result was ‘no abnormalities’, observed in 1046 patients (41.5%). This outcome was slightly more common in males (564 cases) than in females (482 cases), with the difference being statistically significant (p < 0.001).
Haemorrhoids were among the most prevalent abnormalities. Internal haemorrhoids were identified in 960 patients (38.1%), with males demonstrating significantly higher rates than females (634 vs 326 cases, p < 0.001). Similarly, external haemorrhoids were observed in 831 patients (32.9%), with a higher prevalence in males (541 vs 290 cases, p < 0.001). Other common findings included polyps, which were detected in 307 patients (12.2%), although their distribution did not differ significantly between sexes (p = 0.16). Additionally, inflamed mucosa was noted in 99 patients (3.9%), showing no significant sex differences (p = 0.56).
Some findings exhibited notable sex-based disparities. Ulcers and erosions were significantly more frequent in females (n = 25) than in males (n = 16), with a p-value <0.001. In contrast, active bleeding was substantially more common in males (n = 76) than in females (n = 36), with a p-value of 0.04. Another condition with significant sex differences was angiodysplasia, which was slightly more frequent in males (n = 39) than in females (n = 34), yielding a p-value of 0.03.
Rare findings, although less prevalent, included several critical abnormalities. Tumours, including fungating tumours (11 cases), circumferential tumours (17 cases) and cauliflower masses (14 cases), were identified. These findings are particularly significant due to their potential implications for colorectal malignancy. Adhesions causing obstruction were exclusively observed in females, with three cases reported (p = 0.03). Other uncommon abnormalities such as snakeskin appearance, irregularly shaped masses and twisting were reported in only one or two patients each, highlighting the diversity of conditions detectable through colonoscopy.
The results underscore the clinical and demographic variability of gastrointestinal conditions. The high prevalence of common conditions such as haemorrhoids, particularly in males, may reflect more significant access to screening in this population. Conversely, sex-based differences in conditions such as active bleeding and ulcers suggest the need for targeted preventive strategies. Additionally, rare findings such as advanced tumours and adhesions indicate delayed diagnosis due to limited healthcare access, particularly among vulnerable populations. These findings emphasise the importance of sex-specific screening, tailored interventions and improved accessibility to preventive care to optimise outcomes in colorectal health.
In total, 2523 colonoscopy procedures were analysed and categorised into 10 age groups to investigate the distribution of colonic abnormalities and age-related patterns. The most common finding was ‘no abnormalities’; this finding varied significantly across age groups (p = 0.049), with the highest prevalence observed in patients aged 50–59 years (213 cases, 20.4%), as shown in Table 4.
Age distribution of colonic abnormalities among 2523 patients.

Findings are presented as the number of cases in each age group. * indicates statistically significant associations with age.
Haemorrhoids were among the most frequent conditions. Internal haemorrhoids were detected in 960 patients (38.1%), peaking in the 50–59 years age group (211 cases), although no significant association with age was identified (p = 0.13). Similarly, external haemorrhoids were identified in 831 patients (32.9%), peaking in the 50–59 years age group (186 cases), with no significant relationship with age (p = 0.16). Polyps, found in 307 patients (12.2%), were most prevalent in the 50–59 years age group (75 cases); however, this trend did not reach statistical significance (p = 0.26).
Several findings showed significant age-related patterns. Diverticular disease demonstrated a clear association with advancing age, with single diverticula (p < 0.001) and multiple diverticula (p < 0.001) becoming increasingly common in older patients. Single diverticula were rare in individuals aged <50 years but peaked in the 70–79 years age group (n = 6). Similarly, multiple diverticula were most frequent in patients aged 70–79 years (n = 8). Complicated diverticula, although less common, were also significantly associated with age (p = 0.01) and observed in small numbers across patients aged 50–99 years.
Mucosal abnormalities showed distinct age distributions. Mucosal hyperaemia was most frequently detected in younger patients aged 20–29 years (p = 0.01). At the same time, ulcers and erosions were evenly distributed across age groups, showing no clear age-related trend but remaining significant (p = 0.01). Thickening of the mucosa was strongly associated with younger age, particularly in patients aged 20–39 years (p < 0.001), with no cases reported in older patients. Inflamed mucosa, observed in 99 patients (3.9%), was most prevalent in the 50–59 years age group (23 cases) and demonstrated a significant association with age (p < 0.001).
The prevalence of active bleeding showed a progressive increase with advancing age (p < 0.001), peaking in the 60–69 years (25 cases) and 80–89 years (15 cases) age groups. This trend highlights the increasing risk of gastrointestinal bleeding with ageing.
Rare findings included fungating tumours (p = 0.04), predominantly observed in patients aged 60–79 years, with 7 of the 11 cases occurring in this age group. Skip lesions, although infrequent, were more commonly observed in younger patients aged 20–29 years (p = 0.01). Cobblestone appearance was exclusive to patients aged 20–39 years (p = 0.048). Advanced conditions, such as necrotic masses and circumferential tumours, were primarily observed in patients aged over 50 years, although these associations did not reach statistical significance.
Discussion
This study provides a comprehensive analysis of 2523 colonoscopy procedures conducted over 10 years, offering valuable insights into the prevalence and demographic patterns of colonic abnormalities in a Saudi Arabian population. Haemorrhoids were highly prevalent, with internal haemorrhoids observed in 38.1% of patients and external haemorrhoids in 32.9%. Polyps were identified in 12.2% of the patients, with the highest prevalence in individuals aged 50–59 years. Interestingly, ‘no abnormalities’ were reported in 41.5% of the patients, with this finding being more common in males.
The analysis of age- and sex-specific trends in colonic abnormalities revealed distinct patterns with significant clinical and public health implications. Age was found to significantly influence the prevalence of several conditions. Diverticular disease, for example, showed a strong association with advancing age, with both single and multiple diverticula becoming increasingly common in patients aged ≥60 years. This finding aligns with global data, which have consistently reported diverticular disease as predominantly affecting older individuals due to age-related changes in colonic structure and function. 28 Studies from Europe and North America have similarly highlighted a marked increase in diverticular disease incidence in individuals aged >60 years, 3 most prevalent in the 50–59 years age group, underscoring the critical importance of initiating CRC screening at this stage of life. International findings echo this trend, reporting increased polyp detection rates beginning at the age of 50 years, coinciding with the recommended age to begin routine CRC screening. Early detection of polyps is a key strategy to prevent malignant transformation, making this age group a priority for targeted interventions.
Age-specific trends revealed distinct patterns in the presentation of colonic abnormalities. Diverticular disease demonstrated a strong association with advancing age, with single and multiple diverticula becoming increasingly common in patients aged ≥60 years. Conditions such as active bleeding and inflamed mucosa also showed significant age-related increases, particularly in older individuals. Conversely, younger patients (20–39 years) were more likely to present with conditions such as mucosal hyperaemia and skip lesions, suggesting a different clinical profile for this age group.
The high prevalence of haemorrhoids and polyps observed in this study aligns with global trends. Haemorrhoids were identified in 38.1% of the study patients, consistent with the findings from Austria, where a prevalence of 39% was reported among adults undergoing CRC screening. 29 Similarly, polyps were detected in 12.2% of the patients, with the highest prevalence in individuals aged 50–59 years. This is comparable to global data, indicating that the prevalence of colorectal polyps increases with ageing, particularly after the age of 50 years. 30 The slightly lower prevalence of polyps observed in this study compared with those in some global reports may reflect differences in screening coverage, dietary habits or genetic factors influencing colorectal health. For instance, a study from China reported a polyp detection rate of 20.1% among individuals undergoing colonoscopy, which is higher than the rate observed in this study. 30 These variations underscore the importance of considering regional differences when interpreting prevalence data. Overall, although the prevalence rates reported in this study are comparable to global data, the observed sex differences and slightly lower polyp prevalence highlight the need for region-specific studies to enable a better understanding of the epidemiology of colorectal conditions in Saudi Arabia and the broader Middle East.
In this study, sex also played an essential role in the distribution of colonic abnormalities. The observed sex-based disparity, with males showing significantly higher rates of both internal and external haemorrhoids, is noteworthy. Although some studies have reported higher prevalence rates of haemorrhoids in males, 31 others have found no significant sex differences.29,32 This observation is consistent with that reported in regional studies in the Middle East, which have reported a similar male predominance in hemorrhoidal disease. 33 This inconsistency may be due to variations in study design, population characteristics and diagnostic criteria. Potential explanations for this sex-based difference include occupational, physical activity, dietary habit and anatomical variations. 34
These findings underscore the importance of targeted screening strategies, particularly in middle-aged individuals (50–59 years) who exhibit the highest prevalence of abnormalities. Identifying trends in younger patients, such as the occurrence of mucosal hyperaemia, also suggests the need for early diagnostic interventions to prevent disease progression. These results provide critical insights into the epidemiology of colonic abnormalities in Saudi Arabia, supporting the development of age- and sex-specific screening and management strategies to improve colorectal health outcomes.
Inflammatory conditions such as mucosal hyperaemia and skip lesions were more common in younger patients aged 20–39 years. This pattern is consistent with global reports that have identified inflammatory bowel diseases, which often manifest with these findings, as predominantly affecting younger populations.35,36 This trend highlights the importance of raising awareness about inflammatory conditions in younger individuals to enable timely diagnosis and management. 37
Sex-based differences were notable in several conditions. Active bleeding was significantly more common in males. International research has linked higher rates of gastrointestinal bleeding in males to risk factors such as increased use of nonsteroidal anti-inflammatory drugs 38 and alcohol consumption. 39 Ulcers and erosions were observed more frequently in females than in males in this study, similar to previous findings. 40 This finding differs from those of some studies reporting a higher prevalence in males, 41 suggesting the potential influence of regional or cultural factors, which warrants further investigation. These findings may be generalisable to urban tertiary hospitals in Saudi Arabia but not to rural or primary care settings.
Although Saudi Arabia lacks a nationwide CRC screening programme, findings from this study offer critical insights into common abnormalities and age-related patterns, which may support future policy development in CRC screening. These findings underscore the need to implement age- and sex-specific screening and management strategies for colonic abnormalities. The increased prevalence of polyps in middle-aged individuals reinforces the existing guidelines that recommend the initiation of CRC screening at the age of 50 years. The higher rates of haemorrhoids and active bleeding in men suggest the need for targeted education and preventive measures for this demographic population. Additionally, the high prevalence of inflammatory conditions in younger patients highlights the necessity of early diagnostic evaluations in this age group.
Identifying necrotic masses during colonoscopy underscores the importance of prompt histopathological evaluation and intervention to improve patient prognosis. Necrotic masses in the colon are often indicative of advanced malignancies, such as CRC. Necrosis within a tumour typically suggests a high-grade lesion with a propensity for rapid growth and potential metastasis. 42 In addition, tumour necrosis is associated with poorer prognostic outcomes in CRC patients. 43
The cobblestone appearance of the colonic mucosa is a hallmark endoscopic feature of CD. 44 This pattern results from deep, longitudinal ulcerations interspersed with oedematous mucosa, giving the mucosal surface a cobblestone-like appearance. 45 Such findings are crucial for differentiating CD from other inflammatory bowel diseases, as they reflect the transmural inflammation characteristic of CD. 46 The terminologies used in lesion classification (e.g. ‘fungating’ and ‘cauliflower mass’) reflect the language found in the original reports. This inconsistency highlights the need for standardised colonoscopy reporting protocols in the institution.
Recognising this pattern during colonoscopy facilitates early diagnosis and initiation of appropriate therapeutic strategies. Clinically significant findings such as fungating tumours, necrotic masses and cobblestone appearance, although rare, were identified in this study, emphasising the diagnostic utility of colonoscopy in detecting potentially life-threatening conditions. Interestingly, adhesions causing obstruction were exclusively observed in females, highlighting unique sex-specific presentations.
A study by Khor et al. highlighted the diagnostic challenges posed by necrotic tumours in the colon, emphasising the need for comprehensive histological assessment to distinguish malignant from benign lesions. 47
Novelty and limitations of the research
This study significantly contributes to the understanding of colonic abnormalities in Saudi Arabian population, offering one of the most comprehensive analyses conducted in the Western region to date. With a duration of 10 years and analysis of over 2500 colonoscopy reports, this study extended beyond the typical focus on CRC by encompassing a wide range of conditions, including both common (e.g. haemorrhoids and polyps) and rare findings (e.g. necrotic masses and cobblestone appearance). This broad scope allows for a more holistic understanding of colonic health in the region, making the study uniquely positioned to address gaps in the existing literature.
A significant strength of this research is its regional focus. Although extensive data exist on colonic abnormalities in Western populations, 48 studies in Saudi Arabia and the broader Middle East still need to be more comprehensive. 49 By systematically evaluating age- and sex-specific trends, this study provides new insights into the epidemiology of colonic abnormalities, highlighting demographic and age-related increases in the prevalence of conditions. Additionally, the documentation of rare abnormalities such as necrotic masses and cobblestone appearance underscores the diagnostic value of colonoscopy and highlights findings that may have significant clinical implications. These contributions provide a strong foundation for future research into the region’s genetic, environmental and lifestyle factors influencing colorectal health.
Despite its strengths, the study has several limitations. As the findings originate from a single-centre analysis, they may not be fully generalisable to the broader Saudi population. This is because patient demographics and healthcare access can vary significantly across regions. The study’s retrospective nature further limits its ability to ensure complete and consistent data collection, potentially affecting the analysis of rare or less thoroughly documented conditions. Additionally, although the study identified essential trends in colonic abnormalities, it did not correlate these findings with patient symptoms, disease severity or outcomes, restricting its clinical applicability.
The study data did not include laboratory results or histopathological confirmations (e.g. polyp pathology) due to the scope of ethical approval, which limited our access to only colonoscopy reports. Therefore, findings were analysed strictly as reported in endoscopic documentation. Moreover, this study did not assess clinical symptoms or referral reasons for colonoscopy due to data limitations. Future studies should incorporate symptom-based analysis to refine correlations between presentation and findings. The experience level of performing gastroenterologists was not recorded, which may have influenced the detection rates or reporting accuracy. This represents a limitation of the retrospective study design.
Another limitation is the absence of data on genetic, dietary and lifestyle factors that could provide deeper insights into the aetiology of these conditions. Moreover, the underrepresentation of specific demographic groups, such as younger patients or those without access to healthcare, may have skewed the findings. Finally, although the study compares its results with global and regional trends, the limited availability of similar data from the Middle East restricts the contextual analysis of its findings.
Conclusion
This 10-year cross-sectional analysis provides valuable insights into the prevalence and demographic distribution of colonic abnormalities in a Saudi Arabian population. Haemorrhoids and polyps were the most common findings, with significant age- and sex-specific trends. Notably, the prevalence of polyps peaked in individuals aged 50–59 years, supporting the importance of initiating CRC screening in this age group. The higher prevalence of haemorrhoids and active bleeding in males further highlights the need for sex-specific preventive strategies.
Although rare, the identification of abnormalities such as necrotic masses and cobblestone patterns underscores colonoscopy’s diagnostic role in detecting potentially serious conditions. These findings emphasise the importance of comprehensive evaluation during endoscopic procedures.
By addressing gaps in regional data, this study enhances the understanding of colorectal health in the Middle East. However, limitations such as its single-centre design and lack of genetic or lifestyle data should be addressed in future multicentre prospective studies.
These results provide a foundation for improving screening protocols and guiding future research into demographic and environmental influences on colonic health in Saudi Arabian and similar populations.
Footnotes
Acknowledgement
The authors thank all the institutions and individuals who provided valuable support during this study. The authors would like to extend special thanks to the research teams, healthcare professionals and statisticians whose expertise contributed to the successful completion of this work.
Authors’ contributions
All authors contributed equally.
Consent for publication
Not applicable.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no potential conflicts of interest concerning this article’s research, authorship and/or publication.
Ethical approval
This study was approved by the Committee for Research Ethics for the Health of Makkah Region, Ministry of Health (H-02-K-076-0103-268). This study was conducted in accordance with the ethical principles of the Helsinki Declaration of 1975, as revised in 2024.
Funding
This research has not received financial support from any funding agency, commercial or not-for-profit sectors.