
Abstract
Self-expandable metallic stents (SEMS) have been widely used in adults to relieve obstruction secondary to colorectal tumours. However, there is a paucity of literature about their use in children, with only a few case reports describing stent insertion in children with benign colonic conditions. There is one case report on a malignant colonic condition in a child by Hussain et al. in the literature. However, due to the rarity of the condition, there are currently no guidelines from learned societies on colorectal SEMS placement in paediatric patients. We share our experience of using a fully covered SEMS to relieve malignant colonic obstruction in a 6 year-old-child, who was on treatment for T cell lymphoma. This was done as a bridge to surgery, thereby allowing planned surgery, and avoiding colostomy in this child, who went on to have colonic resection with primary anastomosis.
Case report
We report a case of a 6-year-old boy, who was on maintenance chemotherapy for an underlying diagnosis of stage IV T cell lymphoma with loss of MLH1 and PMS2 expression on lymph node biopsy (high probability of lynch syndrome). He presented with a 1 day history of persistent vomiting, abdominal distention and diarrhoea. Investigations showed a haemoglobin of 11.2 g/dl. Renal function, serum electrolytes and liver function tests were normal. An erect abdominal X-ray showed dilated large and small bowel, with air-fluid levels. A contrast-enhanced computed tomography scan of the abdomen and pelvis confirmed proximal descending colon obstruction secondary to an annular stenosing mass. The child was kept nil by mouth, intravenous fluids and analgesia were started and a nasogastric tube was inserted to decompress the bowel. An urgent paediatric surgical opinion was sought. A diagnosis of possible malignant large bowel obstruction was made and gastroenterology review was advised. The gastroenterologist advised unprepared sigmoidoscopy, with biopsy and possible stent insertion. The rationale for this was that this would relieve bowel obstruction, allow time for a definitive histologic diagnosis of the cause of bowel obstruction to be made and potentially allow resection of the obstructed segment of the bowel with primary anastomosis, thus avoiding a colostomy in this very young child. It was decided that, since specific paediatric stents were not available and adult-sized colonic stents would be inappropriate for a child, a fully covered biliary self-expandable metallic stent (SEMS), which has a smaller diameter and length of 10 mm and 6 cm, respectively, as opposed to 20 mm and 13 cm for adult colonic stents, would be used. After informed written consent was taken from the patient’s parents, sigmoidoscopy was performed under general anaesthesia the same day and showed a polypoid stenosing tumour at 20 cm from the anal verge, which was biopsied (Figure 1). A 6 cm × 10 mm fully covered (adult) self-expanding biliary metallic stent was inserted under fluoroscopic assistance , as showed in Figures 2–4. This allowed virtually immediate relief of obstruction, with drainage of close to 1500 ml of liquid stool. No immediate complications were observed. The patient made a good recovery and was allowed home 3 days later. The histology subsequently revealed the tumour to be a poorly differentiated carcinoma with neuroendocrine differentiation. The patient then returned to the hospital 3 weeks later, for an elective left hemicolectomy. The surgical specimen showed a poorly differentiated adenocarcinoma with neuroendocrine and signet ring cell differentiation, pT4 pN3 disease, with the abdominal wall and left peritoneal wall deposits, positive for metastatic disease. The patient was restarted on chemotherapy for his underlying lymphoma, with a plan for possible further treatment for his metastatic colorectal cancer (CRC).

Endoscopic view of the tumour.

After colonic stent insertion

Guidewire passed through tumour.
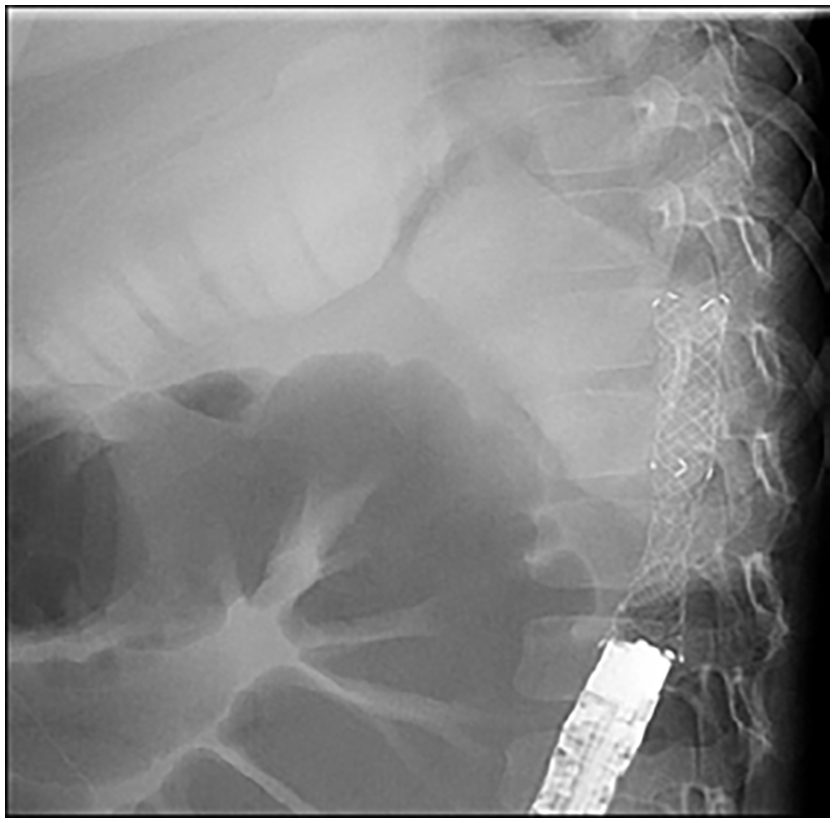
After colonic stent placement.
Discussion
CRC is the third most common cancer in adults, worldwide. 1 However, it is rare in children, with an incidence of one per million.2–4 Similarly, in the adult population 8–13% of the patients present with large bowel obstruction, 5 although malignant strictures are exceedingly rare in paediatric patients.4,6,7 There is, therefore, a scarcity of literature on the management of malignant bowel obstruction in children, with no definite management guidelines available, to date.2,3,6 A case report exists of an infant in whom a removable silicone stent was successfully placed for a benign anastomotic stricture following surgery for Hirschsprung’s disease. 8 In a case series of five patients, Lange et al. 9 describe the use of metallic stents for benign colorectal strictures with variable results. There is just a single case report published in 2004 by Hussain et al. 10 who used SEMS for relieving complete large bowel malignant obstruction in a child. Similarly, due to its rarity, no definitive treatment has been proposed for children with malignant colorectal tumours and the few case reports which do exist suggest using adult chemotherapy protocols in children presenting with CRC. 11 Hence, one might infer that similar management may be applied to address malignant strictures in paediatric patients.
Historically, emergency surgery was considered to be the treatment of choice in adults presenting with malignant bowel obstruction.3,4,12 However, this is associated with high morbidity and mortality due to the hazards of operating on patients with an unprepared bowel which usually results in stoma formation.7,12 Metallic stents, which have traditionally been used for palliation, now are recommended as a bridge to surgery for resectable obstructing colorectal tumours.4,13 A meta-analysis by Allievi et al. 7 compared the use of stents with emergency surgery and found that use of the former was associated with a shorter hospital stay, helped to convert emergency to elective surgery, increased the likelihood of primary anastomosis, avoided surgery prior to diagnosis or staging, and was associated with better quality of life.
Our institution is the largest tertiary care cancer centre in the country and we have extensive experience in using metallic stents in adults, including as a bridge to surgery for obstructing colorectal tumours. Extrapolating the evidence from the literature and based upon our experience of using stents in adults, we decided to treat malignant bowel obstruction in this paediatric patient with SEMS, with good effect. It is important to note here that there are no commercially available colonic stents for this age group 6 and our adult-sized colorectal stents appeared to be inappropriate for a 6-year-old child, weighing only 15 kg. We solved this issue using a fully covered self-expandable biliary metallic stent, which had a smaller diameter and length.
In conclusion, stents can be used to relieve malignant bowel obstruction even in children, thereby saving them from risks of emergency surgery, as well as from stoma formation. Although this is a rare condition, we feel that the use of stents is likely to be of benefit in specialised centres such as ours, and that this represents a useful addition to the currently available forms of treatment for such conditions.
This case has been reported according to case report (CARE) guidelines 2013. 14
Footnotes
Ethics approval and consent to participate
Case report has been approved by the Institutional Review Board of Shaukat Khanum Memorial Cancer Hospital and Research Centre, Lahore. IRB no. EX-21-10-21-01.
Consent for publication
Informed consent has been taken from the parents of the patient for publication of case report and has been documented in patient’s record, hospital information system (HIS).
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Availability of data and materials
Not applicable.