
Abstract
A few cases have shown that bee stings can be linked to coronary stent thrombosis. However, instances of recurrent myocardial infarction resulting from bee stings among patients who have successfully undergone revascularization treatment are rare. This case report describes a man in his early 60s who experienced an acute myocardial infarction. The left anterior descending coronary artery was revascularized by a drug-eluting stent. Just 1 week later, the patient experienced a second acute myocardial infarction and it occurred immediately after a bee sting. Angiography revealed stent thrombosis so thrombus aspiration was performed. Subsequently, the blood flow in the stent was unobstructed. Follow-up coronary angiography 1 year later revealed no signs of restenosis within the stent. Hymenoptera venoms contains thrombogenic substances that might lead to acute stent thrombosis.
Introduction
Bee stings can cause local reactions, including erythema, swelling and pain; systemic toxic reactions such as vomiting, hypotension, and seizures; and rare reactions like cardiac ischaemia and deep vein thrombosis. 1 These clinical responses are associated with Hymenoptera venom. Hymenoptera venom is a poisonous substance that contains a complex mixture of phospholipase A1, phospholipase A2, hyaluronidase, melittin and antigen 5. 2 Relying on mast cell activation and inflammatory mediator release, Hymenoptera venom might lead to stent thrombosis. To the best of our knowledge, very early stent thrombosis in a patient with acute myocardial infarction following a bee sting has not yet been reported. Therefore, this case report describes a man with acute myocardial infarction who developed stent thrombosis following a bee sting.
Case report
A man in his early 60s with chest pain was admitted to the emergency room of the Affiliated Jinhua Hospital, Zhejiang University School of Medicine, Jinhua, Zhejiang Province, China. The patient had a history of hypertension and type 2 diabetes mellitus with high adherence to his antidiabetic and antihypertensive medications. In addition, the patient did not lead a sedentary lifestyle. The patient’s family had no genetic diseases or history of cardiovascular disease. Electrocardiography was administered and revealed ST segment elevation in the I and AVL leads. Immediately after admission, he was taken into a catheterization laboratory for a coronary angiogram. One drug-eluting stent (BuMA® drug-eluting stent; Sino Medical Sciences Technology Inc, Tianjin, China) was implanted in the left anterior descending region of the coronary artery because of severe coronary stenosis. His medications were as follows: 100 mg aspirin, oral, once a day, for 1 week; 75 mg clopidogrel, oral, once a day, for 1 week; 20 mg atorvastatin, oral, once a day, for 1 week. The prognosis was excellent and the patient was discharged after several days.
The patient was readmitted to the emergency room 1 day after discharge. He stated that he was stung by a bee 7 h before admission to the hospital. Within a few minutes of being stung, he experienced a headache, chest tightness and nausea. On admission, erythema could be found throughout the body. His blood pressure was 150/94 mmHg and his heart rate was 83 beats/min. The rest of the physical examination results were normal. Because the patient had a history of myocardial infarction, electrocardiography was performed immediately with ST segment elevation in the I and AVL leads. Based on the medical history, main symptoms, physical examination and auxiliary examination, the patient was diagnosed with acute myocardial infarction, hypertension and type 2 diabetes mellitus. After obtaining informed consent, the patient was taken into a catheterization laboratory for another coronary angiogram. The left anterior descending region of the coronary artery was totally occluded by stent thrombosis (Figure 1(a)). Thrombus aspiration was successfully performed and the primary result was excellent (Figure 1(b)).
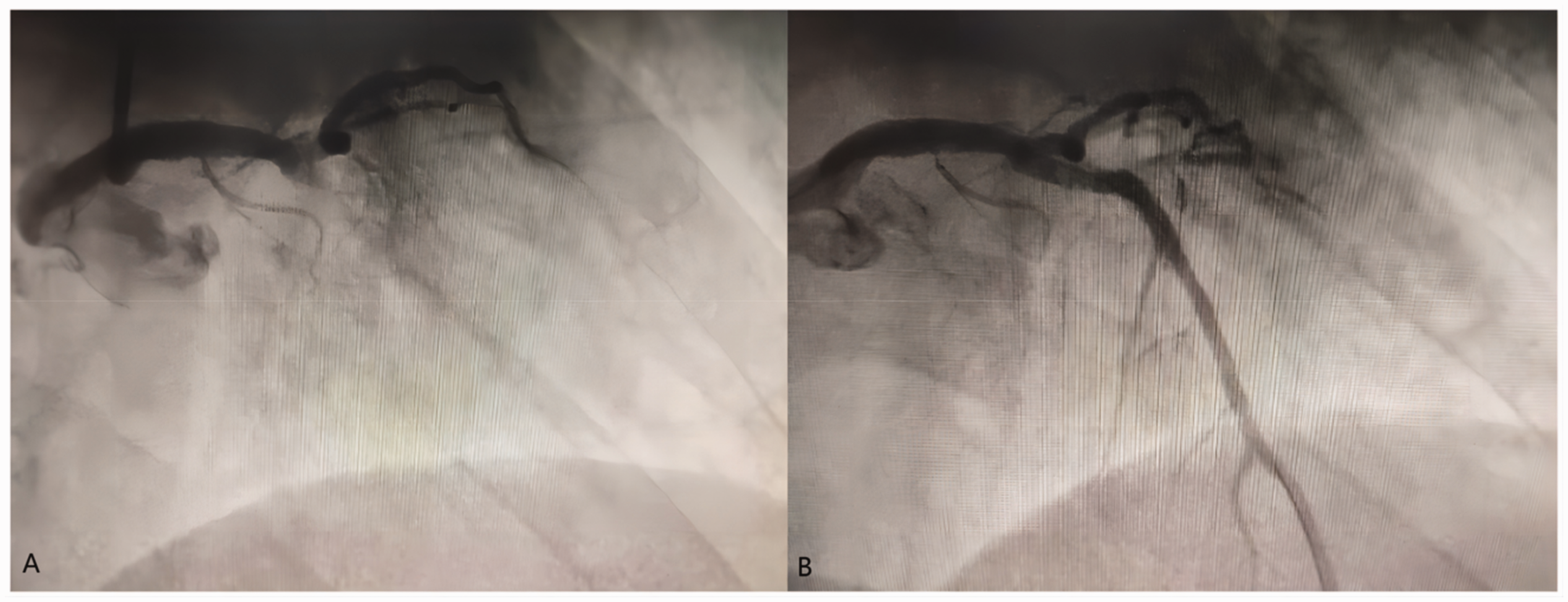
Coronary angiography images of man in his early 60s who initially presented with chest pain and subsequently underwent successful percutaneous coronary intervention for myocardial infarction but after discharge was stung by a bee that resulted in a second myocardial infarction: (a) coronary angiography at the second admission showed that the left anterior descending region of the coronary artery was totally occluded by stent thrombosis and (b) coronary angiography showing that thrombus aspiration was deployed with a good angiographic result.
The postoperative course was uneventful and the patient was discharged after 6 days. His medications were as follows: 100 mg aspirin, oral, once a day, for 1 year; 75 mg clopidogrel, oral, once a day, for 1 year; 20 mg atorvastatin, oral, once a day, for 1 year. Follow-up coronary angiography 1 year later revealed no evidence of restenosis within the stent.
All patient details were de-identified, so signed patient consent was not required. Given the nature of this study, no formal ethics committee approval was necessary. The reporting of this study conforms to CARE guidelines. 3
Discussion
To the best of our knowledge, this is the first description of a patient with acute myocardial infarction who had undergone a successful revascularization and then suffered acute in-stent thrombosis caused by a bee sting.
The clinical outcome of myocardial infarction has been significantly improved by percutaneous coronary intervention. 4 However, the unfavourable effects caused by percutaneous coronary intervention cannot be ignored. Early coronary stent thrombosis is one possible negative result. Five percent of patients with ST-elevation myocardial infarction suffer from early coronary stent thrombosis and these patients always have highly unfavourable mortality rates. 5
Recently, researchers found that Hymenoptera venom was closely linked to coronary stent thrombosis. For example, stent thrombosis caused by bee stings is classified as Type III Kounis syndrome. 6 Kounis syndrome is an acute coronary syndrome that is associated with mast cell degranulation and the release of inflammatory mediators during an allergic reaction. Some cases of coronary stent thrombosis following Hymenoptera stings have reported.7,8 Hymenoptera venom can create vasospasm, nonvasospastic angina and even coronary thrombosis. 9 Mast cells play an important role in this process and they are usually found in the margins of coronary plaques. During the process of thrombus formation, mast cells infiltrate the intima, media and adventitia of the coronary artery adjacent to the stent. There are many immunoglobulin (Ig)E molecules on the surface of mast cells. Degranulation of mast cells occurs when antigens of different specificities encounter the IgE molecules on their cell surface. 10 Substances released in this process, such as histamine, platelet activating factors and cytokines, have been implicated in potentiating platelet agglutination and in transforming stable atherosclerotic plaques to unstable ones that are prone to rupture and the initiation of the cascade of reactions in thrombosis. 7
In this current case, the patient with acute myocardial infarction underwent successful percutaneous coronary intervention. Furthermore, as recommended by guidelines, he continuously accepted dual antiplatelet therapy. Given the occurrence of chest pain after the bite and the follow-up imaging results, we believe that the bee sting caused acute stent thrombosis, rather than stent narrowing or clopidogrel resistance. While several cases have been reported, further studies are still needed to substantiate this correlation and elucidate the exact underlying mechanism.
Footnotes
Author contributions
F.W: conceptualization, data curation, writing – original draft preparation; Z.Y.L: supervision, writing – reviewing and editing.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by grants from the ‘2020 Jinhua Science and technology research plan project’ (no. 2020-3-027). The funding body had no role in the study design, data collection and analysis, and in writing the manuscript.