
Abstract
Data on prognostic factors associated with outcome following resection of perihilar cholangiocarcinoma vary. We sought to define and characterize current available evidence on prognostic factors associated with perihilar cholangiocarcinoma after resection. The PubMed, Embase, and Cochrane library were systematically searched for relevant studies published before December 2019. Prognostic factors were identified from multivariate regression analyses in studies. Only high-quality studies were included (Newcastle–Ottawa Scale > 6 stars). A total of 45 studies involving 7338 patients were analyzed. The meta-analysis demonstrated that serum bilirubin levels (hazard ratio: 1.76, 95% confidence interval: 1.27–2.44), serum CA19-9 levels (hazard ratio: 1.32, 95% confidence interval: 1.05–1.65), tumor size (hazard ratio: 1.27, 95% confidence interval: 1.04–1.55), major vascular involvement (hazard ratio: 1.61, 95% confidence interval: 1.09–2.38), distance metastasis (hazard ratio: 17.60, 95% confidence interval: 2.01–154.09), perioperative blood transfusion (hazard ratio: 1.36, 95% confidence interval: 1.15–1.62), T-stage (hazard ratio: 1.96, 95% confidence interval: 1.47–2.61), lymph node metastasis (hazard ratio: 2.06, 1.83–2.31), resection margin status (hazard ratio: 2.34, 95% confidence interval: 1.89–2.89), not-well histology differentiation (hazard ratio: 2.03, 95% confidence interval: 1.69–2.44), perineural invasion (hazard ratio: 2.37, 95% confidence interval: 1.59–3.55), and lymphovascular invasion (hazard ratio: 1.41, 95% confidence interval: 1.15–1.73) were prognostic factors for poorer overall survival. Adjuvant chemotherapy (hazard ratio: 0.37, 95% confidence interval: 0.25–0.55) had a positive effect on prolonged overall survival. In addition, positive resection margin status (hazard ratio: 1.96, 95% confidence interval: 1.47–2.61) and lymph node metastasis (hazard ratio: 2.06, 95% confidence interval: 1.83–2.31) were associated with poorer disease-free survival. The prognostic factors identified in the present meta-analysis can be used to characterize patients in clinical practice and enrich prognostic tools, which could be included in future trial designs and generate hypotheses to be tested in future research to promote personalized treatment.
Keywords
Introduction
Perihilar cholangiocarcinoma (PHC), which accounts for 60–70% of all cholangiocarcinoma,1,2 is defined as adenocarcinoma of the biliary tract originating from the second-degree bile ducts to the insertion of the cystic duct into the common bile duct.2,3 PHC has an annual incidence of 1 to 2 per 100,000 individuals in the United States. 4 At diagnosis, however, most patients are ineligible for resection because of locally advanced or metastatic disease.3,5 Resection is the only potentially curative option for patients with resectable PHC and most often results in a median overall survival (OS) of only about 35–40 months.6–8
Identifying which patients have a dismal prognosis and which treatments are most likely to benefit patients would enable personalized treatment strategies and improve survival. A variety of prognostic factors are associated with outcome following curative resection of PHC, including resection margin, lymph node status, tumor-node-metastasis (TNM) stage, tumor size, tumor differentiation, perineural invasion, and adjuvant chemotherapy.9,10 However, available prognostic indexes have used different sets of factors based on a limited number of patients and consistent evidence for prognostic factors is still lacking.
This study sought to review systematically the available evidence on the survival of patients with PHC following curative-intent resection as well as analyze clinically relevant prognostic factors.
Methods
A systematic review and meta-analysis on the existing published medical literature were conducted according to the Cochrane Collaboration guidelines. 11
Literature search strategy
The PubMed, Embase, and Cochrane Library were searched for studies published before December 2019 using the following terms and strategy to find the relevant studies: (“cholangiocarcinoma” or “bile duct tumor” or “perihilar cholangiocarcinoma” or “hilar cholangiocarcinoma”) AND (“resection” or “surgery” or “surgical”). The references of the included studies, relevant reviews and meta-analyses were manually screened to look for other eligible studies. Only studies written in English, regardless of which patient population was included.
Eligibility criteria
The inclusion criteria for the eligible studies were (1) studies that reported resected PHC patients; (2) information about PHC populations was provided; (3) studies reported on prognostic factors in multivariate regression analyses; (4) survival data were provided; (5) only high-quality studies were included (NOS score > 6 stars). Studies that met any of the following criteria were excluded: (1) studies on patients with intrahepatic cholangiocarcinoma or distal bile duct carcinoma; (2) studies on patients with gallbladder carcinoma; (3) recurrent PHC; (4) replicated data report from the same author, department, and institution; (5) abstracts, reviews, case reports, letters to the editor, and articles available in non-English language were excluded from analysis.
Data extraction
Two reviewers (L.L. and C.L.) independently screened the titles, abstract, and full texts of the studies and performed data extraction, and a third author (T.Y.) cross-checked the data. Any disagreement was resolved through discussion. The data extracted included the surname of the first author, country, year of publication, period of patient inclusion, number of patients, characteristic of the including patients, independent risk factors of OS, independent risk factors of disease-free survival (DFS). In addition, the number of relevant studies and patients were also calculated, which stratified by sex, age, Bismuth–Corlette classification, 12 major vascular involvement, portal vein involvement, hepatic artery involvement, preoperative jaundice, preoperative biliary drainage, preoperative percutaneous transhepatic biliary drainage (PTBD), preoperative endoscopic retrograde biliary drainage (ERBD), preoperative portal vein embolism, surgical procedures, perioperative blood transfusion, TNM stage (pT1-2, pT3-4, N0, N1-2, M1 and M0), surgical margin (R0 and R1), histology differentiation, lymphovascular invasion, perineural invasion, perioperative complication, perioperative mortality, adjuvant chemotherapy, and radiation. Furthermore, prognostic factors for OS and DFS were identified using multivariate Cox regression analyses from the various studies. We extracted the available multivariate hazard ratios (HRs) with 95% confidence intervals (CIs) for further meta-analysis.
Quality assessment
The modified Newcastle–Ottawa Scale (NOS) was used to assess the quality of the non-randomized studies which were included in the meta-analysis. 13 The maximum possible score was 9 stars and the minimum score was 0. The sum score >6 means a high quality. The Cochrane methodology was used to assess the “risk of bias.” The Grading of Recommendations Assessment, Development and Evaluation (GRADE) System was used to assess the quality of the evidence and the strength of the recommendations. 14
Data analysis
The Review Manager (RevMan, the Cochrane Collaboration, Oxford, UK) version 5.3 was used for data pooling. The primary end-points of this meta-analysis were OS and DFS. The effect measures for the OS and DFS were expressed as HR. The pooled HR and the 95% CI of the outcomes were calculated. Statistical method of Exp(O-E)/Var was adopted to calculate pooled HR. According to the updating Cochrane handbook, random-effects model was chosen as a priority for all analyses, and then the alternative test was performed as a sensitivity test. The results of the data pooling in the meta-analysis were presented as “forest plots.” Generally, heterogeneity between the studies was assessed using the I 2 statistic and chi-square (χ 2 ) based Q-test. An I 2 > 50 or p < 0.1 indicated significant heterogeneity. 15 A p < 0.05 in the Z-test on pooled data was considered as a statistically significant difference. The 95% CI of the pooled ratio was provided for analysis of statistically significant, as well as the effect range estimate.
Results
Through searches of PubMed (n = 1324), Embase (n = 217), and Cochrane library (n = 15) databases, 918 articles were identified while 638 duplicate references were excluded. After title and abstract reviewing, 792 of the 918 original articles were eliminated for failure to meet the inclusion criteria. In addition, of the remaining 126 studies, 55 were excluded after reviewing the full-text due to incomplete data; 26 studies were excluded after reviewing the full-text due to the overlapped data from a same institution or low quality (NOS score ⩽ 6 stars). Eventually, 45 retrospective studies2,7,10,12,16–56 with high quality were included in the systematic review and meta-analysis. The search and screening processes of the medical literature review are summarized in Figure 1.
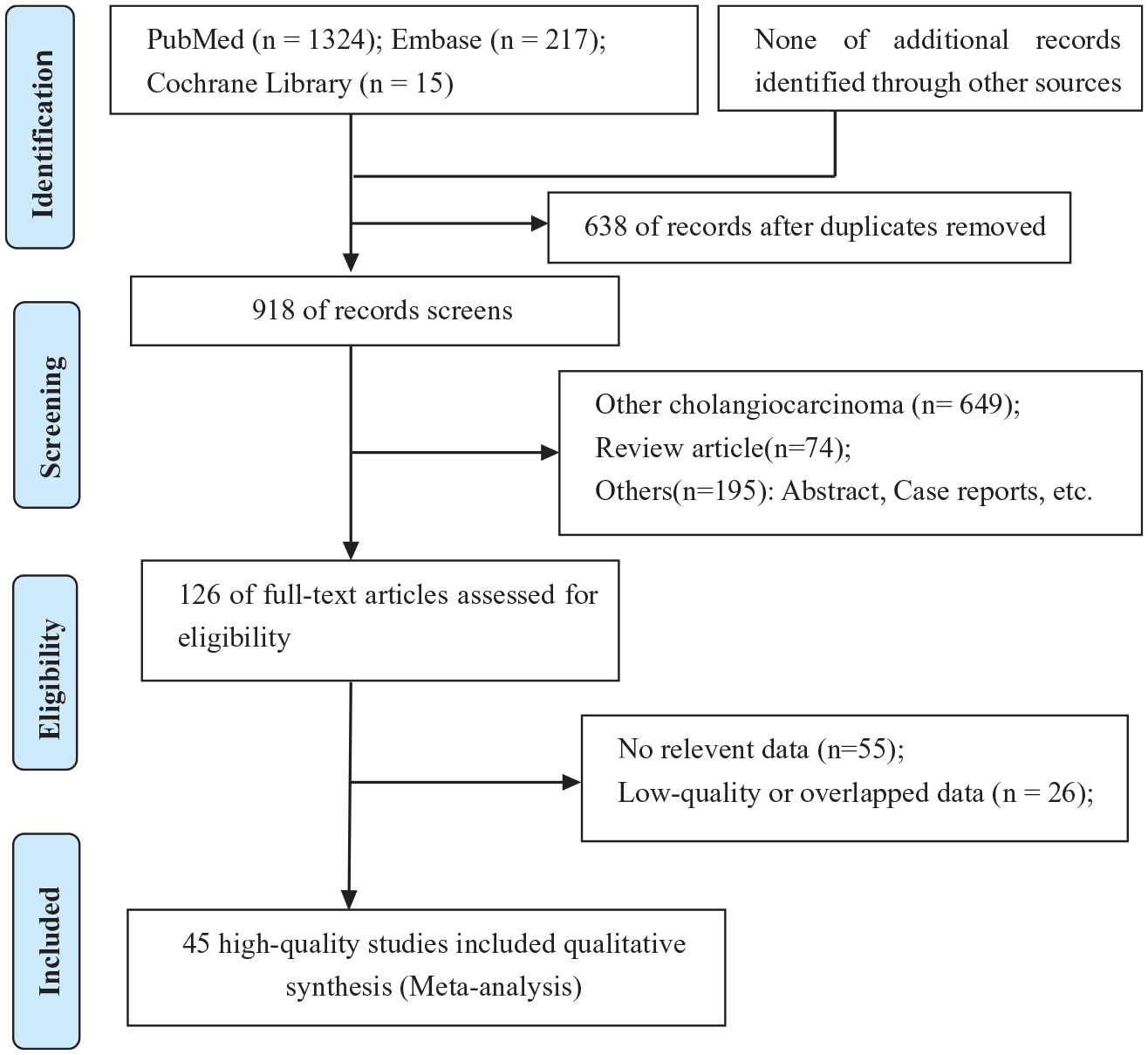
PRISMA flow diagram showing selection of articles for review.
Quality assessment of the included studies
Quality assessment of the included non-randomized controlled trials was evaluated based on the NOS. All of the 45 non-randomized controlled trials studies were relatively high quality with overall NOS scores ranging from 7 to 8 (Supplement Table 1).
Baseline characteristics of the included patients
Forty-five studies2,7,10,12,16–56 that reported 7338 patients undergoing resection of PHC were published between 1996 and 2018. Fifteen studies2,12,16,18,19,21,26,31,32,39,40,43,49,50,53 were from Western countries and 28 studies7,10,17,20,22–24,27–31,33–38,41,42,44–48,51,52,54,56 were from Asia. One studies 55 from Australia, and one study 25 from the cooperation of Japan and United Kingdom. Four studies12,21,31,33 only included patients with Bismuth–Corlette type III or IV PHC and three studies29,38,50 only reported patients with PHC and major hepatectomy. The detailed information of the characteristics of included patients, prognosis of OS and DFS were presented in Table 1. The number of included studies and patients stratified by different characteristics were summarized in Figure 2. Furthermore, more detailed baseline characteristics of the patients in each study were shown in Table 2.
Characteristics of the included studies and independent risk factors.

Age (old vs young); B-C type, Bismuth–Corlette classification (type I/II/III(A/B)/IV); biliary drainage (with vs without); bilirubin (high vs low), serum bilirubin levels; blood loss (more vs less); CA19-9 (high vs low), serum CA19-9 levels; chemotherapy/radiation (with vs without); chemotherapy (without vs with), adjuvant chemotherapy; C-index (high vs low); CLI (with vs without), caudate lobe invasion; CLR (with vs without), caudate lobe resection; complication (with vs without); DFS, disease-free survival; extension to gallbladder (with vs without); HAI (with vs without), hepatic artery invasion; HAR (with vs without), hepatic artery resection; HD (moderate/ poor vs well), histological differentiation; M (+ vs −), with distance or liver metastasis; Muscle mass (low vs high); MVI (+ vs –), microvascular invasion; N (+ vs −), lymphatic nodes metastasis; N-L ratio (high vs low), neutrophil-to-lymphocyte ratio; low skeletal (low vs high); LVI (+ vs −), lymphovascular invasion; OS, overall survival; PBT (with vs without), perioperative blood transfusion; PN (+ vs −), perineural invasion; PTBD (percutaneous transhepatic biliary drainage vs endoscopic retrograde biliary drainage); PVI (with vs without), portal vein invasion; PVR (with vs without), portal vein resection; R, resection margin status (R1 or 2 vs R0); sex (male vs female); T (T3/T4 vs T1/T2), T-stage; tumor size (large vs small); UICC stage (high/low), UICC tumor stage; vascular invasion (with vs without).

Number of included studies and patients stratified by different characteristics.
Baseline characteristics of the patients, their tumors, and long-term survival.

OS, overall survival; PN, perineural invasion.
Prognostic factors for OS
According to the systematic review, a total of 33 risk factors were investigated in multivariate regression analyses (Table 1). From these risk factors, 20 risk factors of OS were available for meta-analysis (Figure 3). Factors with clinically relevant prognostic value of OS included: preoperative serum bilirubin levels, preoperative serum CA19-9 levels, tumor size, major vascular involvement, distance metastasis, perioperative blood transfusion, T-stage, lymph node metastasis, resection margin status, not-well histology differentiation, perineural invasion and lymphovascular invasion. Adjuvant chemotherapy was a protective factor for OS. Of note, factors of sex, age, carcinoembryonic antigen (CEA), preoperative biliary drainage, with liver resection, with caudate lobe resection and with major vascular resection were not statistically associated with postoperative prognosis. Meanwhile, the heterogeneity test demonstrated some factors with high heterogeneity (I2 > 50% or p < 0.05). No significant publication bias was found in the funnel plot.

Forest plots pooled the overall survival stratified by different risk factors.
Prognostic factors for DFS
According to the systematic review, a total of 12 risk factors of DFS were investigated in multivariate regression analyses (Table 1). Among these risk factors, only two risk factors were available for meta-analysis. The clinically relevant prognostic factors associated with DFS included: positive resection margin status (HR: 1.96, 1.47–2.61) and lymph node metastasis (HR: 2.06, 1.83–2.31; Figure 4). Meanwhile, the heterogeneity test demonstrated lymph node metastasis with high heterogeneity (I2 = 84%, p = 0.01). No significant publication bias was found in the funnel plot.

Forest plots pooled the disease-free survival stratified by different risk factors.
Sensitivity analysis
A sensitivity analysis was performed, in which one study at a time was removed, and the other reports analyzed to estimate whether the results changed significantly by the removal of a single study. The sensitivity analysis demonstrated that the present meta-sensitivity analysis did not suggest an undue influence of any single study.
Discussion
This meta-analysis aimed to assess the available evidence on the prognostic factors for patients with PHC following resection. To this end, 45 high-quality retrospective studies comprising 7338 patients were included in the meta-analysis. Of note, the prognostic factors with a significant effect on OS included serum bilirubin levels, serum CA19-9 levels, tumor size, major vascular involvement, distance metastasis, perioperative blood transfusion, T-stage, lymph node metastasis, resection margin status, not-well histology differentiation, perineural invasion, and lymphovascular invasion. In addition, positive resection margin status and lymph node metastasis had a negative effect on DFS.
PHC is a relatively uncommon malignancy with high mortality which is reported to occur more frequently in recent years. As the progress of preoperative management and surgical resection techniques, an enhancement of resectability rate of PHC ranging from 80% to 87% has been achieved. R0 resection has becoming a gold standard of surgical treatment of PHC. Nevertheless, the prognosis is still very poor. As described previously, the prognosis of PHC is associated with multifactors.23,47,52 To improve the survival rate of PHC postoperatively, each clinicopathological factors that can be controlled, associated with prognosis, should be miniaturized.
To our knowledge, there are only two meta-analyses that have reported the prognosis of patients with resectable PHC. In 2018, Bird and colleagues 57 (included 24 studies) and Tang and colleagues 58 (included 38 studies) performed a meta-analysis to only assess the clinicopathological factors associated with prognosis of patients with resectable PHC, respectively. In addition, both of these studies pooled univariable HRs and included some studies with overlapped data. Compared with the two previous meta-analyses, the current review was much more extensive as it included 45 studies comprising 7338 patients. Of note, the method of data extraction and calculation was more robust as it was an adopted HR from multivariable Cox regression analysis. In addition, in this meta-analysis, demographic characteristics, clinicopathological characteristics, surgical procedures, and perioperative treatments were systematic analyzed. Another strength of this study only included high-quality studies (NOS scores ⩾ 6 stars), and some studies with overlapped data were also excluded.
In this meta-analysis, the results demonstrated that serum bilirubin levels, perioperative blood transfusion, T-stage (T3/T4), lymphovascular invasion were independent risk factors for OS and without heterogeneity. Serum CA19-9 levels, tumor size, major vascular involvement, distance metastasis, lymph node metastasis, resection margin status, not-well histology differentiation and perineural invasion were also independent risk factors but with high heterogeneity. Meanwhile, adjuvant chemotherapy had a positive effect on OS without heterogeneity. In addition, serum CEA levels and with major vascular resection were not independent risk factors for OS and without heterogeneity. Sex, age, preoperative biliary drainage, with caudate lobe resection and with liver resection were also not independent risk factors for OS but with high heterogeneity. Furthermore, lymph node metastasis and resection margin status had a negative effect on DFS, but the former had with a significant heterogeneity. Factors with significant heterogeneity indicated that the prognostic value of this variable is yet to be defined.
Lymph node metastasis and margin status were significant prognostic factor in our meta-analysis. Previous studies have similarly reported lymph node metastasis and margin status to be significant prognostic factors for survival, along with perineural invasion and not-well tumor differentiation. PHC recurrence after surgical resection results in poor prognosis and short OS times. Positive margin status and lymph node metastasis were also found to be independent prognostic factors for the DFS. Adjuvant chemo- and/or radiation therapy has not yet been standardized. Surgical resection associated with adjuvant therapy may provide the most favorable outcome. The present meta-analysis also showed that postoperative adjuvant chemotherapy was a positive prognostic factor for PHC after curative resection. However, the difference of chemotherapy protocols and/or radiotherapy were not analyzed in-depth, because the available data were limited.
Several limitations should be considered when interpreting data from this study. Although we only selected high-quality studies, all of the included studies were predominantly retrospective in nature. As such, there may be inherent selection bias from some of the studies. The consistency and representativeness of patients included was suboptimal. This heterogeneity in the selection of patients may have led to selection bias. In addition, not all relevant factors were reported in each study and analyzed in multivariable Cox regression analysis. Finally, some prognostic factors were with significant heterogeneity. Subsequently, the results of these factors should be interpreted with caution.
In conclusion, this systematic and meta-analysis provides updated and more robust evidence on prognostic factors in resection of PHC. Prognostic factors identified in this review can be used to better characterize patients in clinical practice, guide the development of better prognostic models, and be used in future trial design as stratification factors or to be included in regression review analyses. Due to some factors with high heterogeneity, future randomized controlled trials are needed to better define the role of these factors.
Supplemental Material
sj-pdf-1-cmg-10.1177_2631774521993065 – Supplemental material for Prognostic factors of resectable perihilar cholangiocarcinoma: a systematic review and meta-analysis of high-quality studies
Supplemental material, sj-pdf-1-cmg-10.1177_2631774521993065 for Prognostic factors of resectable perihilar cholangiocarcinoma: a systematic review and meta-analysis of high-quality studies by Lei Liang, Chao Li, Hang-Dong Jia, Yong-Kang Diao, Hao Xing, Timothy M. Pawlik, Wan Yee Lau, Feng Shen, Dong-Sheng Huang, Cheng-Wu Zhang and Tian Yang in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
Author contributions
L.L., H.X., F.S., D.-S.H, C.-W.Z., and T.Y. conceived and designed the study. L.L. and C.L. searched the literature and extracted the data. L.L., H.-D.J., and Y.-K.D. wrote the manuscript. T.M.P. and W.Y.L. proofread the manuscript. T.Y. obtained funding. All authors approved the final version of the manuscript. The authors declare no competing financial interests.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant nos. 81672699 and 81972726). Approval for this study was obtained from the Ethics Committee of our hospital.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Congress publication
The abstract of this study has been presented as a poster presentation in the congress: “3rd International Advanced Liver & Pancreas Surgery Symposium—ISLS 2019” (10–12 October 2019, Istanbul, Turkey).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.