
Abstract
Objective
The mean platelet volume (MPV) is a measure of platelet size, and it is considered a surrogate marker of platelet activation. Because the correlation between platelet count/size and lung cancer prognosis remains unclear, this meta-analysis comprehensively evaluated the prognostic significance of MPV among patients with lung cancer.
Methods
A systematic search of PubMed, Embase, Google Scholar, and additional sources of relevant studies were conducted with no language restrictions from inception to 7 May 2021. Overall survival (OS) and disease-free survival (DFS)/progression-free survival (PFS), as well as their hazard ratios (HR) and 95% confidence intervals (CIs), were pooled to evaluate the relationship between MPV and survival. The study protocol was registered on PROSPERO.
Results
Eleven studies involving 2421 patients with lung cancer were included in our analysis. Nine studies including only patients with non-small cell lung cancer were included in the meta-analysis. Our analysis revealed no significant associations of MPV with OS (HR = 1.09, 95% CI = 0.84–1.41) and DFS/PFS (HR = 1.13, 95% CI = 0.58–2.20).
Conclusion
Pretreatment MPV levels did not display prognostic significance in patients with NSCLC. Large-scale prospective studies and a validation study considering ethnicity and lung cancer staging are warranted.
Introduction
Lung cancer is the most prevalent cancer globally, being responsible for an extremely high number of cancer-related deaths in both men and women. 1 The prognosis of lung cancer is grim with a 5-year survival rate well below 15% despite advancements in radical surgery, radiotherapy, chemotherapy, and targeted therapy or immunotherapy. 2
Various novel biomarkers that predict the prognosis of lung cancer have been identified, including include carcinoembryonic antigen, cytokeratin-19 fragments, squamous cell carcinoma antigen, progastrin-releasing peptide, tumor M2-pyruvate kinase, and C-reactive protein. However, these prognostic biomarkers are not included in routine testing in the majority of patients with lung cancer owing to their high costs. 3 Mean platelet volume (MPV) is an inexpensive and potential prognostic marker that has been explored in a variety of cancers including lung cancer.
MPV is a measure of platelet size, and it is considered a surrogate marker of platelet activation. 4 Large platelets are more reactive and more likely to aggregate; thus, they are easily exhausted. Cancer-associated increases in platelet activation and subsequent exhaustion represent a plausible hypothesis that explains the decrease in platelet size in patients with cancer including lung cancer.4,5 Thus, a low MPV indicates exhausted platelets with potentially tumor growth-promoting cytokines causing worse outcomes in patients with cancer. 6
Various studies have explored the potential role of MPV largely as a prognostic and predictive biomarker among patients with cancer such as gastric cancer, bladder cancer, renal cancer, endometrial cancer, non-small cell lung cancer (NSCLC), and hepatocellular carcinoma.7–12 However, the correlation between platelet count/ size and lung cancer prognosis remains controversial because some studies determined that MPV is a poor prognostic factor in NSCLC whereas others suggested that MPV has no association with lung cancer.11,13–15 Thus, a robust analysis investigating the prognostic value of MPV among patients with lung cancer is needed. We conducted a meta-analysis to comprehensively evaluate the prognostic significance of MPV in this malignancy.
Materials and methods
Data sources and search strategies
Electronic databases such as PubMed, Embase, and Google Scholar were searched to identify relevant studies with no language restrictions from inception to 7 May 2021. The search used combinations of the terms “mean platelet volume,” “MPV,” “lung neoplasms,” “lung cancer,” “carcinoma, non-small cell lung,” and “carcinoma, small cell” as both medical subject headings and keywords with an appropriate Boolean operation. The detailed search strategy is available in Supplementary File 1. Furthermore, we checked the reference lists of all included studies and studies included in previous reviews to identify additional studies. A grey literature search was performed using Google Scholar and Open Grey. In addition, preprint servers and thesis repositories were also searched. Full texts were requested from the corresponding authors via mail and ResearchGate. This meta-analysis was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The study protocol, with well-defined methodology and inclusion criteria, was registered on PROSPERO reference number ID: CRD42021285941.
Selection criteria
The inclusion criteria in this meta-analysis were as follows: 1) provided data on the prognosis of patients diagnosed with lung cancer pathologically; 2) directly provided pretreatment MPV measured with hazard ratios (HRs) and 95% confidence intervals (CIs) or provided sufficient information to permit these values to be estimated; and 4) provided data on the relationship of survival outcomes including OS and/or DFS/progression-free survival (PFS) with MPV. Letters, reviews, experimental studies, case reports, conference abstracts, and non-human studies were excluded.
Data extraction and quality assessment
Two independent authors (SK and SS) reviewed original articles and selected the articles using the eligibility criteria. Any discrepancies during the selection process were resolved through discussion with a third reviewer (PS). A data extraction spreadsheet was created on Microsoft Excel version 2013 (Microsoft Corp., Redmond, WA, USA) to extract the data under different headings as follows: author, publication year, study region, study design, age (median age of the sample), sample size, follow-up duration in months (median/range), treatment status of the patient, clinical stage of the cancer, cutoff of MPV, cancer type, HRs with 95% CIs for OS and DFS/PFS, and Newcastle–Ottawa Scale (NOS) scores. Multivariate HRs were preferred over univariate HRs if both were given because of the advantage of multivariate analysis in excluding confounding factors. HRs from multivariable analyses were extracted when available. Otherwise, HRs from univariate analyses were extracted or estimated from Kaplan–Meier survival curves as described by Parmar and colleagues. 16 The value estimated from these curves was confirmed by requesting the HR from the corresponding author of the relevant study. DFS and PFS were considered the same in this analysis. We included only studies with the aforementioned data on patients with NSCLC in the meta-analysis to reduce bias and provide consistent findings. The NOS was used for the quality assessment of each study and described under three subscores: selection (maximum score, 5), comparability (maximum score, 2), and exposure (maximum score, 3). 17 Two authors independently assessed the study, and any disagreements were solved through discussion with the third author. Studies with scores of 6 or higher qualified for inclusion, and studies with scores exceeding 7 were considered high-quality studies.
Data synthesis and statistical analysis
All analyses were performed using STATA version 16.0 (StataCorp, College Station, TX, USA). HRs with 95% CIs were used to evaluate the relationship between MPV and lung cancer prognosis. Statistical heterogeneity was assessed using the Cochrane Q-test and the I2 statistic, with P < 0.1 or I2 > 50% indicating significant heterogeneity. 18 A random-effects model (DerSimonian–Laird method) was applied in cases of significant heterogeneity. Otherwise, a fixed-effects model was used to pool HR. 19 Subgroup analysis based on the country of origin, cutoff, tumor stage, sample size, and type of analysis was performed to identify the cause of significant heterogeneity.
Moreover, sensitivity analysis was performed by omitting each individual study sequentially to check the stability and robustness of the pooled outcomes. Publication bias was estimated using Begg’s correlation test and Egger’s linear regression test. P > 0.05 indicated the absence of significant publication bias along with the observation of symmetry in the funnel plot.20,21
Results
Study characteristics
A flowchart demonstrating the details of study selection according to the PRISMA guidelines is presented in Figure 1. In total, 85 studies were identified through database searches. First, we removed 26 duplicate articles, and the titles and abstracts of the remaining articles were screened. The 31 remaining articles with full text after screening were assessed per the eligibility criteria. Finally, 11 full-text articles including 2421 patients with lung cancer were included.11,15,22–30 Meanwhile, the meta-analysis only included studies of patients with NSCLC (n = 9).

A flowchart demonstrating the details of the study selection according to the PRISMA guidelines.
The characteristics of the included studies are presented in Table 1. All included studies were published from 2014 to 2020, and all studies were retrospective. Five studies were conducted in China,8,24–26,29 three studies were conducted in Turkey,15,22,23 two studies were conducted in Japan,11,30 and one study was conducted in Korea. 28 A study by Shi et al. had two datasets for HRs for patients with adenocarcinoma and squamous cell carcinoma. 24 Similarly, survival outcomes were described for patients with NSCLC in nine studies, patients with small cell lung cancer (SCLC) in one study, and patients with either NSCLC or SCLC in one study. In our analysis, five studies included patients with advanced lung cancer, whereas five studies included patients with both early-stage and advanced lung cancer. Most of the patients in the included studies were elderly, with a median age exceeding 60 years. Five studies used an MPV cutoff of <10 fL, five studies used a cutoff of >10 fL, and the cutoff was not mentioned in the final study. Last, the quality of the studies as by the NOS scale ranged from 6 to 8, as presented in Table 2.
Characteristics of the studies included in the analysis.
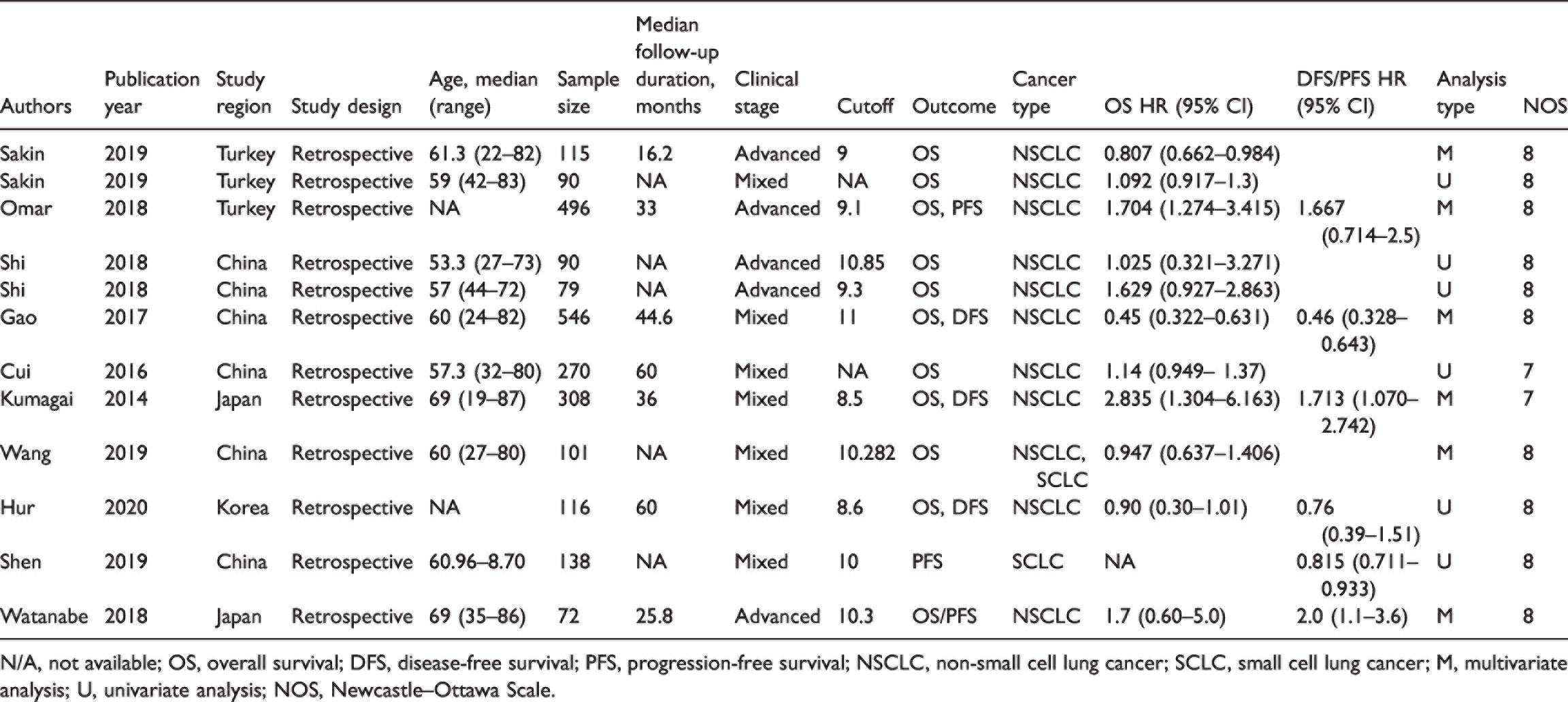
N/A, not available; OS, overall survival; DFS, disease-free survival; PFS, progression-free survival; NSCLC, non-small cell lung cancer; SCLC, small cell lung cancer; M, multivariate analysis; U, univariate analysis; NOS, Newcastle–Ottawa Scale.
Newcastle–Ottawa Scale for observational studies.
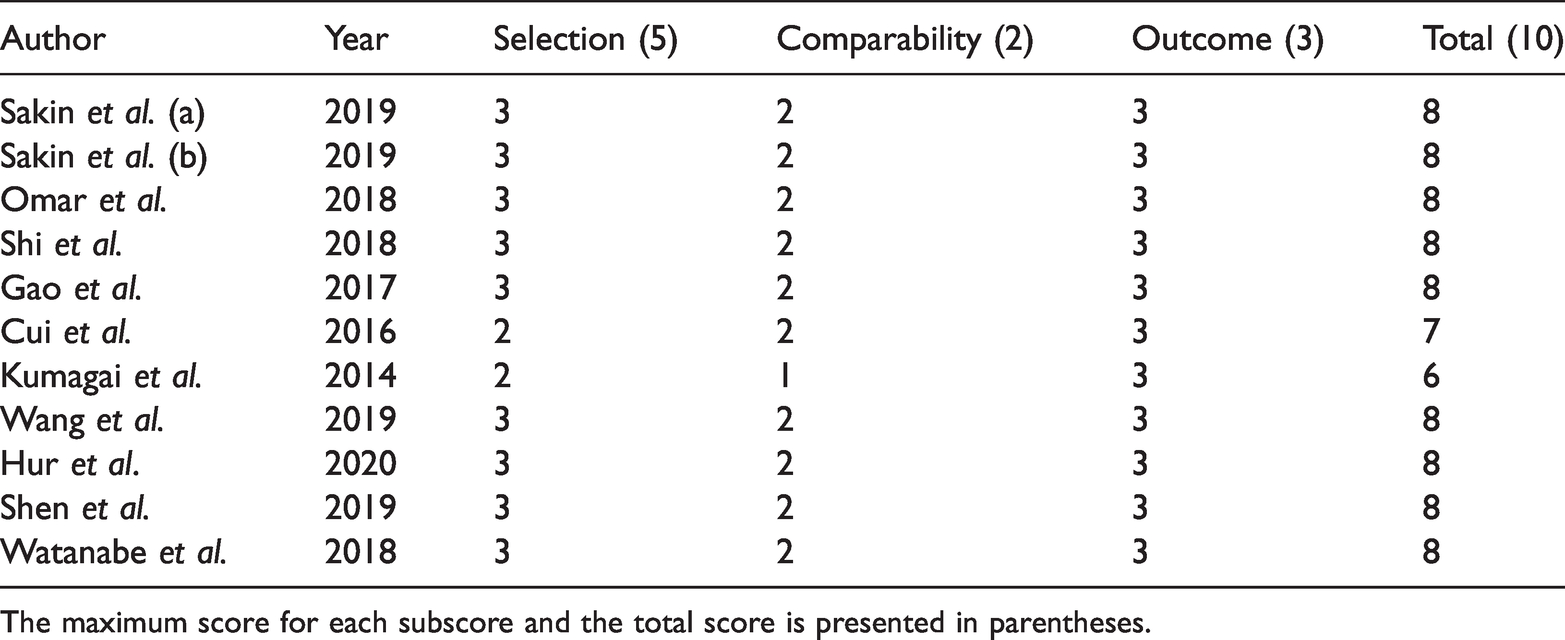
The maximum score for each subscore and the total score is presented in parentheses.
Meta-analysis (OS, DFS/PFS)
Nine studies11,15,22–28,30 including 2182 patients were included in the meta-analysis to assess the association between MPV and OS (Figures 2 and 3). The pooled HR for OS was 1.09 (95% CI = 0.84–1.41, P = 0.53). Because the analysis revealed significant heterogeneity (I2 = 79.75%, P < 0.001), a random-effects model was used. The model illustrated that MPV was not significantly associated with unfavorable OS among patients with NSCLC. Furthermore, subgroup analysis was performed (Table 3) for variables such as study region, sample size, clinical stage, and MPV cutoff, and no significant association between MPV and OS was observed in any subgroup.
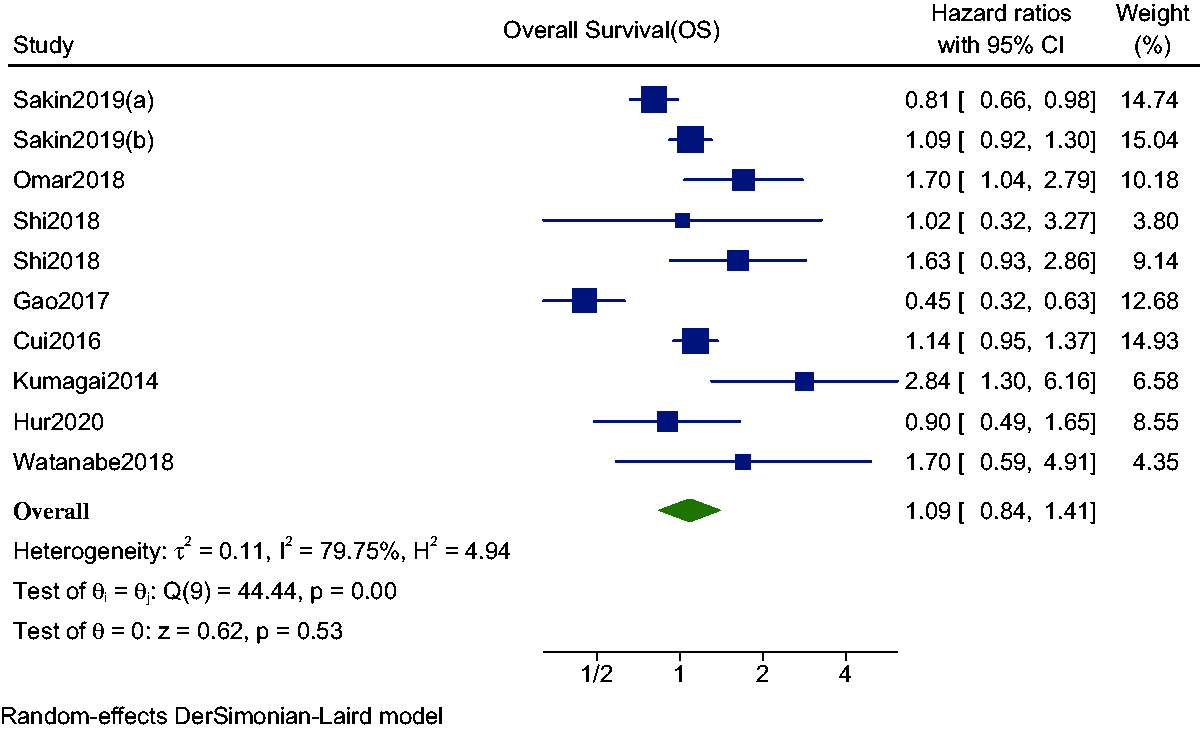
Forest plot with 95% CIs for the meta-analysis of association between OS and MPV.

Funnel plot for overall survival in the included studies.
Subgroup analysis of the associations of MPV with OS and DFS.

MPV, mean platelet volume; OS, overall survival; DFS, disease-free survival; PFS, progression-free survival; HR, hazard ratio; CI, confidence interval.
Similarly, five studies11,23,25,28–30 including 1538 patients were included in an analysis to assess the association of MPV with DFS/PFS. The pooled HR for MPV was 1.13 (95% CI = 0.58–2.20, P < 0.71), indicating no significant association between MPV and DFS/PFS in patients with lung cancer. The analysis identified significant heterogeneity (I2 = 88.01%, P = 0.71), and thus, a random-effects model was used (Figure 5). Subgroup analysis was performed, as presented in Table 3, and using variables such as study region, sample size, clinical stage, and MPV cutoff. Among the examined variables, a significant association between MPV and worse DFS/PFS was only observed in the study region subgroup.
Publication bias and sensitivity analysis
Figure 3 presents a symmetrical funnel plot and the results of Egger’s regression test, and no significant publication bias was observed in the analysis of OS (P = 0.13). Similarly, there was no evidence of publication bias among studies included in the analysis of DFS/PFS (Egger’s regression test, P = 0.31; Figure 6). Sensitivity analysis of studies included in the assessments of OS and DFS/PFS confirmed the reliability and robustness of our analyses (Figures 4 and 7).

Sensitivity analysis for studies of overall survival.

Forest plot with 95% CIs for the meta-analysis of the association between DFS/PFS and MPV.

Funnel plot for disease-free survival/progression-free survival.

Sensitivity analysis for studies of disease-free survival/progression-free survival.
Discussion
Investigations and research on prognostic markers are crucial particularly among patients with cancer because they can facilitate the improvement of existing treatments and development of newer treatment therapies and strategies of patient care. Previous meta-analyses only analyzed survival outcomes in different types of cancers including lung cancer. To our knowledge, this is the first meta-analysis to assess the prognostic significance of MPV regarding survival outcomes exclusively among patients with lung cancer.
A meta-analysis by Pyo et al. in 2016 illustrated that MPV was significantly higher in patients with malignant tumors than in healthy subjects. However, in lung cancer, MPV was lower in patients before treatment than in healthy subjects, albeit without significance (mean difference = −0.352, 95% CI = −0.763 to 0.060). 13 A recent meta-analysis found no significant association between MPV and survival outcomes among patients with cancer. In a subgroup analysis of seven studies, higher MPV was not associated with worse OS in NSCLC (HR = 0.85, 95% CI = 0.64–1.15). 14 Our study included 11 studies of patients with NSCLC and/or SCLC, whereas nine studies including only patients with NSCLC were included in the meta-analysis to reduce bias. Similarly as the aforementioned studies, no significant association between MPV and outcomes was observed.
Subgroup analysis was conducted by country of origin, MPV cutoff, clinical stage, sample size, and type of analysis. All subgroup analyses revealed insignificant associations between MPV and OS. Concerning DFS, a significant association between MPV and worse DFS was observed in the analysis of country of origin. However, the limited number of studies included in the subgroup analyses led to inconsistent findings.
We believe this result requires verification regarding prognostic significance in a validation cohort because univariate analysis carries a high risk of bias, leading to overestimation of sensitivity and specificity in predicting cancer prognosis. Interestingly, worse DFS was not significantly associated with MPV among patients with advanced cancer. These findings differ from those of a study indicating that MPV was similarly between patients with early-stage lung cancer and healthy subjects and that MPV increased with cancer progression. 31 However, the result cannot be generalized considering the small number of studies and sample size.
The platelet volume is determined during both megakaryopoiesis and thrombopoiesis. Various stages of platelet production and maturation are influenced by cytokines such as interleukin-6, granulocyte colony-stimulating factor, and macrophage colony-stimulating factor. 32 Moreover, platelets can be activated upon encountering circulating tumor cells, which results in the formation of microparticles that can potentially promote the invasiveness of tumor cells. 33 Therefore, this close interplay between high MPV and poor prognosis in cancer is a reasonable hypothesis. By contrast, our findings do not support the hypothesis that MPV is a prognostic factor for poor outcomes in patients with lung cancer.
The strength of our study lies in the fact that this is the first meta-analysis to examine the association between MPV and survival outcomes in patients with lung cancer. In contrast to previously published meta-analyses, our study results enable a deeper comprehensive understanding of the predictive role of MPV in lung cancer. However, this study had several limitations. The inclusion of retrospective studies with no randomized control trials and inclusion of only English-language studies might have added biases and excluded potentially suitable studies. Second, studies provided HRs and 95% CIs from univariate analyses, which could lead to bias concerning the overestimation of the prognostic role of MPV because multivariate HRs may not be statistically significant after the consideration of other elements. In addition, as with all meta-analyses, heterogeneity resulting from various factors, as depicted in the subgroup analysis, can potentially affect the results, thus mandating cautious interpretation. Moreover, because the incidence of lung cancer and patient survival differ significantly based on race and ethnicity, further prospective studies elucidating the role of MPV in consideration of these factors are necessary. 34 Last, the clinical application of MPV in predicting DFS mandates further verification because of the lack of a standardized cutoff.
Conclusion
Our meta-analysis revealed that pretreatment MPV does not have prognostic significance in NSCLC. Further high-quality, well-designed, large-scale studies with a uniform cutoff considering various factors such as patient ethnicity and lung cancer stage are necessary to establish the role of MPV as a prognostic tool for screening and/or monitoring lung cancer in clinical practice.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221084874 - Supplemental material for Prognostic significance of mean platelet volume in patients with lung cancer: a meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605221084874 for Prognostic significance of mean platelet volume in patients with lung cancer: a meta-analysis by Sanjeev Kharel, Suraj Shrestha, Prafulla Shakya, Rohit Rawat and Ramila Shilpakar in Journal of International Medical Research
Footnotes
Availability of data and materials
All necessary data and information are presented within the article. A supplementary file containing the search strategy has been provided.
Additional information
Appendix 1. Search strategy for PubMed.
Author contributions
SK and SS were involved in the conceptualization of the study along with designing the study search strategy, reviewing study abstracts, extracting data from full-text articles, and drafting the initial manuscript. PS, RR, and RS were involved in editing and revising the manuscript. All authors read and approved the final version of the manuscript.
Declaration of competing interests
None to declare.
Funding
No funding was required for the work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.