
Abstract
Objective:
Percutaneous cecostomy is a minimally invasive procedure that provides access to the colon for therapeutic interventions. This review aimed to update and summarize the existing information on the use and application of percutaneous endoscopic cecostomy in the field of therapeutic gastroenterology.
Data Sources:
A systematic review of the literature was performed without any restrictions on the year of publication from the date of inception in 1986 to January 2021.
Methods:
The review was performed using the medical subject heading keywords in the following search engines: MEDLINE, EMBASE, Cochrane, and Google Scholar.
Results:
A total of 29 articles were subjected to final data extraction. The review included a total of 174 patients who underwent percutaneous cecostomy. Most of the included studies were conducted in the United States (n = 14). The most common comorbidity was cancer (n = 10) and the major indication for performing percutaneous cecostomy was colonic pseudo-obstruction or Ogilvie’s syndrome (n = 15). The main technique for performing percutaneous cecostomy was endoscopy (17 studies), followed by fluoroscopy- (five studies), computed-tomography- (three studies), laparoscopy- (two studies), and ultrasound- (one study) guided procedures. The procedure was technically successful in 153 (88%) cases. The total cumulative rates of major and minor complications were 47.5%. These complications included tube malfunction, local wound site infections, and bleeding and rare complications of peritonitis and death.
Conclusion:
Percutaneous cecostomy is a safe and effective option for managing acute colonic pseudo-obstruction. It leads to durable symptom relief with low to minimal risk.
Introduction
A minimally invasive access to the gastrointestinal (GI) tract is required to manage several medical conditions if a surgical or radiological intervention is not feasible due to unexpected patient- or procedure-related factors. The availability of highly innovative endoscopic and interventional radiology techniques, however, has made such procedures more feasible with fewer complications. Creating access to the lower GI tract is a difficult task due to patient anatomy, including sigmoid colon mobility, dolichocolon, and presence of vital structures within the cecal pole, which includes the appendix, ileocecal valve, and appendiceal orifice. Furthermore, normal physiological motility may limit bowel localization and translumination because physiological antegrade bowel motility may hinder unexperienced endoscopists from widely using endoscopic-based technique. Traditional surgical cecostomy involves major invasive surgery that includes risks of developing stomal stenosis and leakage, appendiceal necrosis, inadvertent bowel perforation, and the potential risk of administering general anesthesia. Subsequently, this surgical approach is replaced by percutaneous cecostomy (PEC), which can be performed under the guidance of radiological methods, such as computed tomography (CT), ultrasound (US) imaging, fluoroscopy of the abdomen, and operative laparoscopy.1–3 Although its usage is infrequent in the adult patient population, PEC is an increasingly performed procedure due to its technical success and low morbidity rates in selected patients.4,5 It is utilized widely in the pediatric population for functional bowel disorders, including constipation, fecal incontinence,6,7 and congenital denervation bowel disorders. 8 It has several advantages, including a reduction in pain, enhanced recovery rates, and the possibility of performing the procedure in patients with higher morbidity in whom surgical cecostomy is not feasible. The aim of the current review is to perform a summary update for the current information about imaging-guided PEC in adult patients and its application in the field of therapeutic gastroenterology.
Methods
A comprehensive systematic review of the literature was conducted in major search engines, such as PUBMED/MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), and Google Scholar. In this review, we used a series of keywords (percutaneous cecostomy, interventional radiology, imaging-guided). The protocol of this systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 9 The keywords used were ((‘percutaneous’[All Fields] OR ‘percutaneous’[All Fields] OR ‘percutaneous’[All Fields]) AND (‘Cecostomy’[All Fields] OR ‘Cecostomy’[MeSH Terms] OR ‘Cecostomy’[All Fields] OR ‘Cecostomy’[All Fields]) AND (‘adult’[MeSH Terms] OR ‘adult’[All Fields] OR ‘adults’[All Fields] OR ‘adults’[All Fields])). The different methods used to perform cecostomy and their reported complications as outcomes of interest were the aims of this review.
Inclusion and exclusion criteria
Only evidence-based and peer-reviewed articles that studied PEC based on original data collected from adult human patients were included. We did not restrict articles based on sex, publication year, or language. Review articles, commentaries, clinical trials protocols, editorial, proceedings summary, instrument development summary, or those that studied cadavers only were excluded.
The process of inclusion and exclusion is shown in Figure 1. The reviewer assessed each reference against prespecified inclusion and exclusion criteria using a multistep process: first, ‘titles’ and ‘abstracts’, followed by ‘full text articles’.

Flowchart showing the overview of the inclusion and exclusion processes in the systematic review.
Data extraction
Data were obtained using an extraction form in which information was collected from all the eligible articles. All basic features of the articles, which comprised of the publication details (author and year), type of publication, number of participants, and their characteristics, were included.
Quality appraisal
Each article was assessed using a quality assessment tool. Considering that only case reports and case series were obtained in the results of our search, the tool for evaluating the methodological quality of case reports and case series proposed by Murad et al. 10 was used to assess the quality of the studies. This was a modification of the Newcastle–Ottawa Scale. This tool was used to examine four domains, which included selection, ascertainment, causality, and reporting. It had a total of eight questions to find the quality score. If all the domains were satisfactory, the study was classified as ‘good quality’; if three domains were satisfactory, the study was classified as ‘fair quality’; and if only two or one domains were satisfactory, the study was classified as ‘poor quality’. The author assessed each study independently and compared the scores later to reach a consensus. If an agreement was not reached, a second independent reviewer was consulted.
Results
Literature search results
In total, 447 articles were identified initially (Figure 2). Subsequently, 367 remained after removal of duplicates from those that were initially screened. After exclusion of 325 articles based on the exclusion criteria listed earlier and a manual search, 29 full-text articles were extracted and included for final analysis. The selected studies were enumerated based on their first author and year of publication (Table 1). The year of publication ranged from 1986 11 to 2019. 12

PRISMA for the search and selection of evidence-based articles on percutaneous cecostomy in intervention radiology and its application in the field of therapeutic gastroenterology.
Included studies in the systemic review.
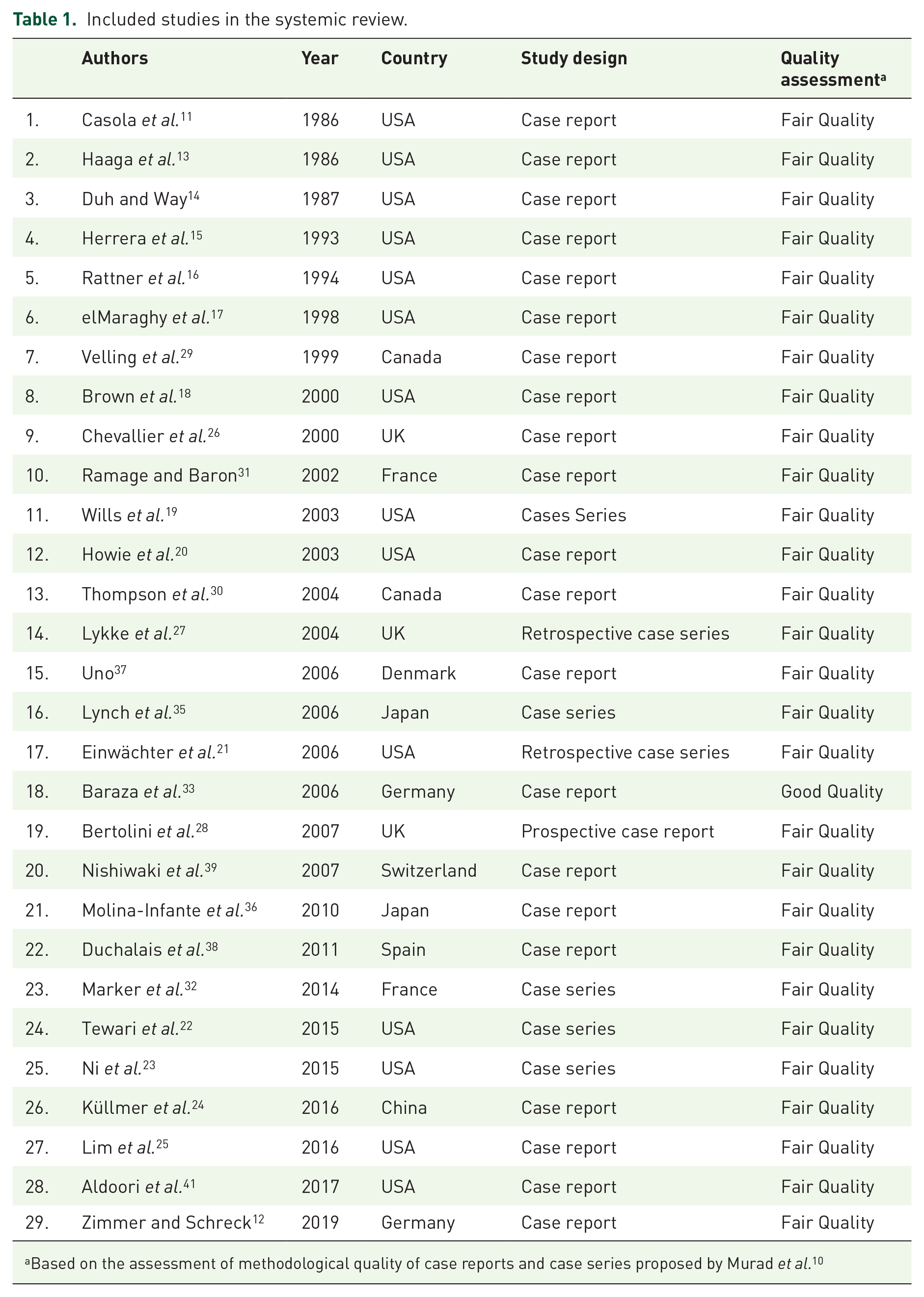
Based on the assessment of methodological quality of case reports and case series proposed by Murad et al. 10
Characteristics of the included studies
Most of the included studies were conducted in the United States (n = 14),11,13–25 followed by the United Kingdom (n = 3),26–28 Canada (n = 2),29,30 France (n = 2),31,32 Germany (n = 2),33,34 Japan(n = 2),35,36 China (n = 1), 24 Denmark (n = 1), 37 Spain (n = 1), 38 Switzerland (n = 1), 39 and Czech Republic (n = 1). 40 Most articles, which constituted 75.8% (n = 21) of the review, were case reports,11–18,20,24–26,29–31,33,36–39,41 followed by case series (n = 7)19,21–23,27,32,35 and a single prospective study. 28 All domains were satisfactory in a single study alone after application of the quality assessment tool (grade: good). In addition, 28 studies were classified as having a ‘fair quality’ (Table 1) and supplemental material.
Patient characteristics
The mean age of patients who were evaluated across all studies was 66.64 (range = 23–89) years. Not all case reports specified the patients’ sex. Among those who reported their sex, however, 44 were women and 62 were men. A total of 174 patients were evaluated across all the studies. The most common comorbidities of the participants were cancer (n = 10), dementia (n = 5), cerebrovascular accidents (n = 6), and diabetes (n = 4). The main indication for performing PEC was colonic pseudo-obstruction or Ogilvie’s syndrome (n = 16).
Characteristic of the PEC procedure
(a) Procedural technique: The main technique used for performing PEC was endoscopy (n = 17),12,15,16,18,19,21,23,24,27,28,30,31,33,35–38 followed by fluoroscopy- (n = 7),20,22,25,26,32,41 CT- (n = 3),11,13,25 laparoscopy- (n = 2),14,17 and US-guided22,39 procedures. The procedure was successful in a total 153 patients (93.86%) included in this review. This was described as a technical success in which intraluminal placement of the catheter tip was accomplished.
(b) Choice of the procedure: Among the studies, 17 included an explanation regarding the rationale of selecting the method of choice for the placement of PEC. The stated reasons are limited colonoscopy, 14 dolichocolon, 36 specific indication to deliver a therapeutic agent (fecal microbiota transplantation), 23 ineligibility for surgery,19,20,25–27,31,33,39 multiple prior colonic decompressions and the subsequent choice to proceed with colonoscopy and PEC,18,21,24,26,31 interposition between the stomach and transverse colon,20,37 inability to decompress the colon by colonoscopy and subsequent choice to proceed with fluoroscopy 29 or abdominal CT scan with fluoroscopic PEC insertion, 25 patient refusal to undergo surgical cecostomy, 27 and a new diagnosis of colon cancer. 39
(c) Preprocedure bowel preparation: Preprocedure bowel preparation was reported in 11 studies. Otherwise, most of the studies did not mention or specify a bowel preparation prior to the procedure, especially in patients with ACPO.11–14,18,23,25–28,37 Patients diagnosed with refractory constipation and neurogenic bowel were subjected to bowel preparation, which included an oral bowel preparation with polyethylene glycol solution typically 2 days prior to the procedure19,31–33,35,36,38 with a range of 2–6 liters and bisacodyl tablets. The other laxatives used were sodium phosphate for refractory constipation 35 and phosphate salt enema. 36
(d) Periprocedure antibiotics prophylaxis: Thirteen studies discussed their prophylactic antibiotic regimens and when the prophylactic antibiotics were administered (preprocedure, postprocedure, or pre- and postprocedure). The antibiotics used were oral, which included neomycin (1 g, 24 h before the procedure) 19 or kanamycin (3 g for 3 days before the procedure). 37 Intravenous regimens employed a wide spectrum of agents, which included the cephalosporin group. This included IV cefotetan (1000–2000 mg), 14 IV ceftriaxone (750 mg), 12 IV cefuroxime (750 mg),30,33 and IV cefoperazone 39 to cover gram-positive organisms, along with another agent used to cover anaerobic organisms with metronidazole (500 mg)18,30,33 or gentamicin 32 in conjunction with cephalosporin. Other agents such as IV piperacillin/tazobactam for broad coverage31,37 and amoxicillin/clavulanic acid31,38 used for outpatients were used as well.
(e) Procedural anesthesia: Twelve studies included procedures that were performed under conscious sedation.15,18,20,27–29,31–33,35,37 Six studies used general anesthesia.14,21,23,25,36,38 General anesthesia was used only in three studies without mentioning the agents used or its relation to the type of procedure. It was used in a CT fluoroscopic-guided, 25 laparoscopic, 14 and endoscopic-guided 38 PEC. Conscious sedation used with IV midazolam in doses ranged from 2 to 6 mg30,33 or in conjunction with fentanyl.31,32 IV propofol23,36 was used alone for conscious sedation. A few studies used only topical local anesthesia without conscious or general sedation.19,24
(f) Types of tube selected for the PEC procedure: The most commonly used tube was the percutaneous endoscopic gastrostomy (PEG) tube, followed by the PEC tube and T-fasteners (Table 2). A total of 16 studies utilized the endoscopic PEC technique using a variety of different catheter sizes. The 20 French (six studies) size, however, was the most commonly used. This was followed by size 16 (two studies) and 15 French (two studies). The other studies mentioned the usage of 14, 5, and 24 French. The operators in those studies did not elaborate on their catheter choice. Cecopexy was conducted to ensure proper fixation of the device and to minimize stool spillage and peritoneal contamination. This was achieved using an anchor system to fix the cecum to the anterior abdominal wall. This was reported in three studies using a variety of 3-4 nylon T-fasteners.26,35,36 Radiological modalities, such as abdominal US, CT of the abdomen, and fluoroscopy were employed based on techniques that used a variety of catheters with different sizes. The less commonly used catheters used in the review were urology catheters. These included a 12-French Foley catheter 14 and a 5-mi balloon suprapubic cystostomy catheter. 11
Cecostomy tubes and their method of insertion at the studies.

ACE, antegrade continence enema; CT, computed tomography; PEC, percutaneous endoscopic colostomy; PEG, percutaneous endoscopic gastrostomy; US, ultrasound.
Complications
The review shows that, despite an invasive intervention, there were a total of 83 reported complications (47.5% of the whole cohort) as shown in Table 3. There is a predominantly minor complication related to tube malfunction with a total of 41 incidents (23.6%). This type of complication is managed by replacing or removing the tube. Surgical intervention is no longer needed (Table 2). Other predominant complications include infection (n = 26, 14.8%), local pain (n = 10, 5.7%), and bleeding complications (n = 3, 1.67%).
Reported complications rates of percutaneous cecostomy.

PEC, percutaneous endoscopic colostomy.
Major complications were reported in only three articles, whereas minor complications were reported in seven articles. Among the complications reported by Lynch et al., 35 peristomal infections treated with antibiotics were observed in two patients, whereas peritonitis was reported in one patient. The occurrence of a large painful pneumoperitoneum around the PEC entry site (n = 10), chronic wound pain lasting for more than 3 months (n = 9), serous leakage (n = 7), minor wound infection (n = 2), and accidental removal of catheters (n = 2) were reported by Duchalais et al. 38
PEC removal was performed in patients with chronic local wound pain (n = 5, 26%). Marker et al. 32 reported one major complication, which was a pericecal abscess. Tewari et al. 22 reported the case of one patient who presented with sepsis and extensive subcutaneous emphysema, which extended cranially from the PEC tube site. Baraza et al. 33 reported a series of cases with complications such as peritonitis (n = 3), tube migration (n = 1), PEC-related death (n = 1), recurrence (n = 1), abdominal wall bleed (n = 2), PEC site infection (n = 6), buried bumper (n = 1), site pain (n = 1), and urgency (n = 1). Bertolini et al. 28 reported one patient who developed peritonitis and required surgery.
Discussion
The existing data are heterogeneous and consist mainly of case reports and case series with approximately 33 patients. This review focused on the procedure performed in adults aged 23–89 years. All of them had comorbidities that subsequently affected their clinical outcomes after PEC.
In addition, they shared a history of long duration of symptoms and multiple hospital admissions ranging from 3 months to 8 years. PEC was a clinically acceptable procedure that reportedly resulted in a better quality of life in adult patients with different neurological bowel conditions. The indication for this procedure in adults was colonic pseudo-obstruction or Ogilvie’s syndrome, which was characterized by colonic distension in the absence of mechanical obstruction. It was a common occurrence in hospitalized patients with serious conditions or in elderly patients who were bedridden.34,42 According to our findings, PEC was most frequently performed in patients affected by this syndrome. Other reported indications included the delivery of fecal microbial transplants 23 and relief of cecal volvulus. 43
The technique was most frequently used for PEC and was similar to the placement of PEG.12,18–21,23,26,28,30,33,36 This technique was originally described by Ponsky et al. 44 In this procedure, the cecum was fixed to the anterior abdominal wall, which reduced the potential for intraperitoneal spillage and allowed repeated instillation of large volumes of bowel cleansing agents safely and effectively. New techniques, which provided a better visualization of the cecostomy site, however, were described. Uno 37 described the introducer method, which helped avoid inadvertent placement of the cecostomy in the terminal ileum or any other undesirable spot. The CT technique was described as difficult as it did not allow good visualization of the wall of the bowel.13,15,25 This was a concern if the patient had a long-standing obstruction.
Several solutions were suggested to have a better fixation of the tube to the cecal wall. Lynch et al. 35 modified their procedure, so that three T-fasteners were placed in a triangular fashion around the tube. This prevented tube displacement. In contrast, the US technique facilitated puncture and the passage of a T-fastener needle into the cecum. This technique was useful in preventing peritonitis. 39 Unfortunately, the optimal cecostomy technique has not been established. The tract of the puncture improves with time, enables the replacement of the tube, and secures a less chance for peritoneal spillage.
This review showed success rate of 88% in performing the procedure. Most cited studies that were carried out in children showed a technical success rate of 78–100% and a clinical success rate of 84–100%.34,45–47 The complication rate in children was reported to be between 14% and 42% with most complications being minor. In our review after exclusion of the major complications, namely, severe pneumoperitoneum, peritonitis, and death, the total reported complication rate was 44%. The most common complications observed were pain, leakage, and buried bumper. Severe complications, which were rare, were consisted of migration, perforation, and sepsis. Peritonitis occurred due to fecal contamination secondary to tube migration. 33 In a different case, peritonitis was caused by inadvertent traction of the tube. 28 Thus, caregivers should be aware of the risk associated with handling these patients. Moreover, we agree with the findings of Rattner et al. They mentioned that the risk of peritonitis could be lessened by preparing the bowel, staging the dilation over two or more sessions, and letting the tract mature over a week to permit the formation of a pseudoepithelium. 16 One of the main advantages of PEC over surgical cecostomy was the presence of the cecostomy tube, which prevented stenosis of the stoma. Improvement in the quality of life was noted in several case series in which different instruments were used for assessment of patients with neurogenic and functional bowel disorders.32,48,49
The strength of our review is the inclusion of a survey of several online sources of data without limitation of the date of publication and language, which has allowed us to access a huge number of articles. This contrasted the previous review performed by Ben Ameur et al. in 2013, which involved a limited review of literature. 49 Nevertheless, this review also has several limitations. For instance, data resources were noncomparative and relied on a limited number of retrospective case series and reports with inherent variability in the technical success between the centers where the procedure was performed. Moreover, this review was limited only to adult patients with variable comorbidities.
Conclusion
Percutaneous endoscopic cecostomy is a feasible therapeutic intervention in patients with acute colonic pseudo-obstruction. It leads to durable symptom relief with low to negligible risk. To date, this is the largest review regarding PEC and this is the main strength of this analysis. The number and quality of available literature on this topic, however, are low, which, in contrast, is its main weakness. Thus, the findings from our review cannot be substantiated as the grade of evidence is considered very low in case series/reports. Nevertheless, inferences from such reports can be used for decision-making in individual cases. Prospective studies are needed in the future to further evaluate the benefits and disadvantages of performing this procedure.
Supplemental Material
sj-docx-1-cmg-10.1177_26317745211073411 – Supplemental material for Therapeutic utility of percutaneous cecostomy in adults: an updated systematic review
Supplemental material, sj-docx-1-cmg-10.1177_26317745211073411 for Therapeutic utility of percutaneous cecostomy in adults: an updated systematic review by Yasir Mohammed Khayyat in Therapeutic Advances in Gastrointestinal Endoscopy
Footnotes
Author contributions
YMK contributed to conceptualization, data curation, formal analysis, investigation, and writing-original draft.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author would like to thank the Deanship of Scientific Research at Umm Al-Qura University for supporting this work by Grant Code: (22UQU4290113DSR01).
Conflict of interest statement
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.