
Abstract
Background:
Self-expandable metallic stents have not only largely replaced surgical gastrojejunostomy for unresectable gastric cancers, but their role as bridging therapy for resectable obstructing tumours is also evolving.
Objective:
To evaluate the efficacy and safety of pyloric stents in gastric outlet obstruction in patients with gastric cancer and assess survival in patients with resectable obstructing gastric tumours in whom stents were inserted as a bridge to surgery.
Methods:
We retrospectively reviewed the electronic medical records of patients who underwent self-expandable metallic stent insertion for gastric outlet obstruction due to gastric cancer from January 2014 to March 2019.
Results:
Out of 161 patients, clinical improvement was observed in 159 (99%) and 156 (97%) at 1 and 12 weeks of stent placement, respectively. None of these patients experienced serious complications, such as perforation or aspiration pneumonia. Of these 161 patients, enteral stents were placed as bridging therapy prior to surgery in 40 (24.8%). Among these, 35 (87.5%) of 40 underwent neo-adjuvant chemotherapy followed by curative surgery. Of the 35 patients, 3 failed to follow-up. One-year survival following curative surgery was 87.5%. Stent helped to reduce vomiting and improve nutrition, measured by the body mass index (p = 0.36) and serum albumin (p = 0.05), over a 4-week period following stent insertion.
Conclusion:
Pyloric stents are useful in relieving malignant gastric outlet obstruction, maintaining nutrition during neo-adjuvant treatment and improving survival without additional risk of postoperative complications. They have traditionally been used for palliation, but should also be considered as bridging therapy for obstructing resectable gastric tumours during neo-adjuvant treatment.
Introduction
Malignant gastric outlet obstruction (MGOO) occurs secondary to a tumour in the distal stomach or proximal duodenum, or by extrinsic compression caused by, for example, a pancreatic head tumour or by a malignant nodal mass. Symptoms may include nausea, intractable vomiting and abdominal pain. Pancreatic and gastric cancers are among the most common malignancies causing MGOO.1–3 Less frequent causes are duodenal, ampullary or hepatobiliary malignancies as well as lymphomas. 2 In developed countries, pancreatic cancer (15–20%) is the leading cause of MGOO, whereas in Asia gastric cancer (35%) is responsible for the majority.1,3,4 Gastric cancer remains the fourth most common malignancy and the second leading cause of cancer-related deaths, worldwide. 2 Surgical gastrojejunostomy (GJ) has been considered as the standard palliative treatment to relieve obstruction in advanced unresectable gastric cancer. 5 However, the use of stents is now increasingly being advocated, not only because they represent a less invasive alternative to GJ, with low associated morbidity and mortality, but also because they are associated with an earlier resumption of oral intake.5,6 Similarly, for resectable obstructing gastric tumours, it is important to alleviate symptoms and improve nutritional status.7,8 This in turn ensures uninterrupted neo-adjuvant treatment of the cancer, which is now becoming the standard of care for upper gastrointestinal (GI) tumours including gastric cancer. This is because neo-adjuvant therapy has been shown to result in improved long-term survival and in a lower rate of recurrence.7–10 While only a few studies have investigated the role of temporary fully covered self-expandable metallic stents (SEMS) in this subset of patients, the minimally invasive nature and good safety profile of SEMS suggest that they should be considered as a bridge to surgery in this cohort of patients. 11
The aim of this study was to retrospectively analyse the outcome of SEMS use in patients with GOO secondary to gastric cancer in the palliative setting and when used as a bridge to surgery in a curative setting. It also evaluates the efficacy and safety of pyloric stents in GOO in gastric cancer and 1-year survival in patients with resectable obstructing gastric tumours where stents were placed as a bridge to surgery.
Methods
IRB approval
After approval from the Institutional Review Board (IRB) of Shaukat Khanum Memorial Cancer Hospital and Research Centre, we retrospectively reviewed the electronic medical records of 161 patients who met the inclusion criteria and who underwent endoscopic placement of SEMS for GOO due to gastric cancer from January 2014 to March 2019.
Inclusion and exclusion criteria
Inclusion criteria comprise all gastric cancer patients with GOO at presentation and patients aged between 18 and 80 years. Patients with GOO secondary to cancers other than those of the stomach and gastric cancer with histopathology other than adenocarcinoma were all excluded. Patients with prior stent insertion were disqualified.
Procedural techniques
An upper GI endoscopy was performed, using a therapeutic gastroscope, to assess the nature and site of obstruction. A biliary catheter and a floppy guide-wire were used to negotiate the stricture, and contrast was injected under fluoroscopic control to assess the length and extent of the stricture and to ensure that the guide-wire had traversed the entire length of the stricture. The stent delivery system was then passed through the working channel of the gastroscope, over the guide-wire, and the stent was deployed under direct vision, with adjunct fluoroscopic control, in a standard manner. All stents used were standard fully covered SEMS (nitinol) with a size of 20 mm × 130 mm. Patients usually resumed oral intake of liquids within 6 h of stent placement. Diet was gradually advanced to a liquid/pureed diet over 24 h and to a soft diet thereafter, as tolerated. All these patients were assessed and given dietary advice by a clinical nutritionist prior to discharge from the endoscopy suite.
Data collection
Patient charts were reviewed to collect data on baseline characteristics, including demographic details, gender, age, body mass index (BMI), comorbidities, primary diagnoses and stage of disease at presentation. Stent efficacy was measured using the Gastric Outlet Obstruction Scoring System (GOOSS) at the time of stent insertion and at 1 and 12 weeks after stent insertion, while safety was documented by reviewing early and delayed stent-related complications. The rate of re-stenting, postoperative complications and 1-year survival following surgery was also assessed. Assessment of nutritional status was done by recording average BMI and serum albumin levels prior to stent insertion and at 4 weeks after stent insertion.
Statistical analysis
Statistical analysis was carried out using the Statistical Package for the Social Sciences (SPSS) software (version 20.0; SPSS, Chicago, IL, USA). Descriptive analysis was done using summary measures for categorical variables and continuous variables. Categorical variables were computed as frequencies and percentages, while continuous variables were stated as mean ± standard deviation. The paired t test was used to check the pre- and post-stenting mean difference in BMI and albumin. A p value of <0.05 was considered statistically significant. Overall survival was calculated using Kaplan–Meier curves.
Definitions
Malignant gastric outlet obstruction
MGOO is mechanical obstruction to the passage of food at the level of the distal stomach or proximal duodenum by loco-regional tumours, presenting with symptoms of outlet obstruction and confirmed endoscopically.
Technical success
The placement of an enteral stent across an obstructing tumour, confirmed on fluoroscopic imaging.
Efficacy/clinical improvement
Improvement in symptoms due to MGOO. This was assessed using the GOOSS at the time of stent insertion and at 1 and 12 weeks after insertion.
GOOSS
This scoring system is based on the following parameters.

GOOSS, gastric outlet obstruction scoring system.
Failure in improvement in GOOSS after stent placement implies stent failure. 12
Safety of stents
Safety was defined in the study as the absence of early or delayed complications after stent placement in all patients, as well as the absence of postoperative complications in those who underwent curative gastric resection at some point after stent placement.
Early and delayed complications
Adverse events that occurred within 7 days of stent placement were considered to be early; all others were defined as delayed complications.
Results
Patient characteristics
Out of 161 patients, 110 were men (68.3%) and 51 were women (31.67%), with an average age of 50.97 ± 12.5 years. Of these, 135 (83.8%) had no comorbidities, whereas 26 (16.1%) had concomitant underlying medical conditions, including diabetes mellitus, hypertension and ischaemic heart disease, as shown in Table 1.
Baseline characteristics.

Outcome variables
Technical success of pyloric stent placement was achieved in all (100%) our patients. Clinical improvement was calculated by the GOOSS at baseline, at 1 week and at 12 weeks after pyloric stent insertion. At the time of stent insertion, 118 patients (73.3%) had a GOOSS of 0 and 43 (26.7%) had a GOOSS of 1. This was reassessed on day 7 following stent placement, and the GOOSS had improved by >1 point in 99.3% and by >2–3 points in 69.3% of these patients. At 12 weeks, 35 patients (21.7%) were lost to follow-up, while in the remainder the GOOSS had improved by >1 and >2–3 points in 99.1% and 80.1%, respectively, which was statistically significant. This has been shown in Tables 2 and 3.
Improvement in gastric outlet obstruction score.

GOOSS, gastric outlet obstruction scoring system.
Gastric outlet obstruction scoring system (GOOSS) before (GOOSS 0) and after stent insertion (GOOSS 1 and GOOSS 12).
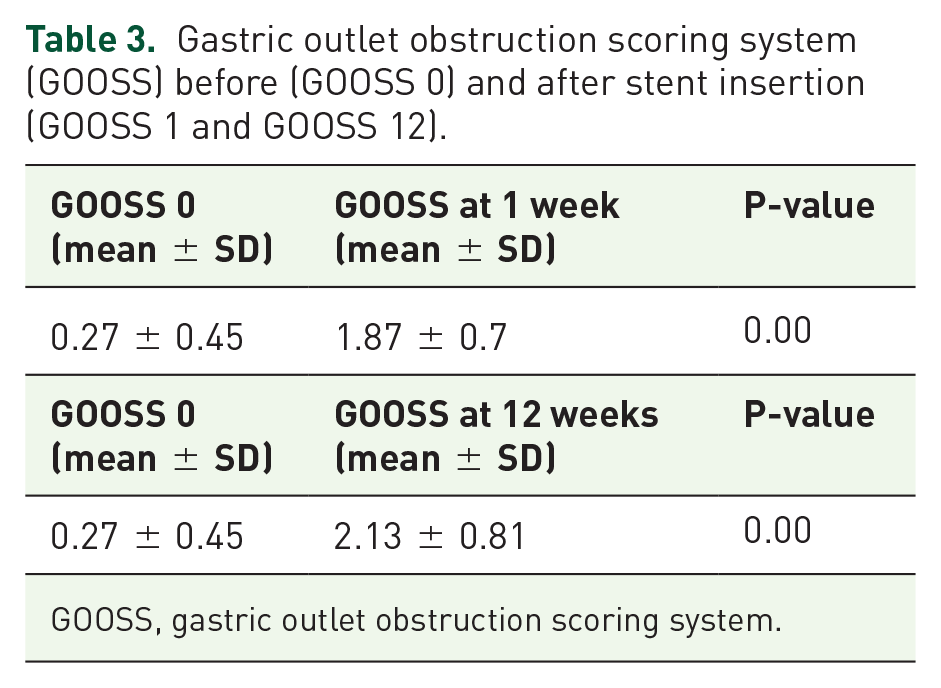
GOOSS, gastric outlet obstruction scoring system.
None of the 161 patients experienced serious complications, defined as perforation or aspiration pneumonia following stent insertion. Similarly, no early stent-related complications were observed. Late complications occurred as follows: 35 (21.7%) had stent migration, 21 (13%) had stent fracture and 11 (6.8%) patients had stent obstruction. Reviewing all 161 stented patients, 59 (36.6%) patients required repeat stent insertion. A total of nine patients (6.2%) underwent surgical GJ due to either recurrent stent-related complications, including fracture (3/9) and stent migration (2/9), or progressive disease causing multilevel small bowel obstruction (4/9).
Pyloric SEMS as a bridge to surgery
A subgroup analysis was performed for 40 (24.8%) patients in whom a stent was placed as a bridge to surgery for potentially resectable obstructing gastric tumours. Out of these, 2/40 were deemed inoperable owing to comorbid illnesses, while 3/40 were lost to follow-up. As a result, 35 patients underwent neo-adjuvant chemotherapy followed by curative surgery. One-year survival data following surgery were available for 32 of these 35 patients, after excluding a further 3 patients who were lost to follow-up after surgery. In the first 3 months following surgery, all the patients survived, while there were two deaths at 4 months and another two deaths between 8 and 9 months. As a result of these, an overall 28 patients survived at 12 months following curative surgery. Figure 1 shows the survival curve for this cohort.

One-year survival curve of the subgroup that underwent curative surgery following pyloric stent insertion as a bridge to surgery.
A 1-year survival following surgery was also seen according to the stage of cancer. In both stages I and III, the 1-year survival was 100%. All the four deaths were from stage II cancer, with two patients dying at 4 months and another two patients dying between 8 and 9 months. This is shown in Figure 2.

One-year survival curve of the subgroup that underwent curative surgery following pyloric stent as bridge to surgery according to the stage of cancer.
Serum albumin and BMI
Serum albumin and BMI were assessed before stent placement and at 4 weeks following stent insertion. The non-significant p values signify that the nutritional status was maintained during the period of neo-adjuvant chemotherapy, as shown in Table 4.
Nutritional assessment of patients who underwent surgery.

Discussion
MGOO can be caused by various locally advanced tumours, which have a detrimental effect on the overall health of patients.2,3 This study focused on MGOO caused by gastric cancer. Several studies have shown that many gastric cancers present late, as stage III or IV disease, with outlet obstruction requiring urgent intervention to alleviate symptoms. In our region, only 33% of gastric cancers are resectable at the time of presentation, with 66.7% being managed with palliative intent. 13 Patients with potentially curable disease usually receive neo-adjuvant chemotherapy followed by assessment for partial/complete gastrectomy as definitive treatment. On the contrary, patients in a palliative setting who have MGOO undergo GJ or SEMS insertion for symptom control. 14
Many trials and meta-analyses have compared SEMS insertion with GJ and have shown the obvious benefits of SEMS over GJ. 2 Open GJ was considered the choice of procedure for palliative treatment, but this has changed since the introduction of laparoscopic GJ (lap. GJ), which is safer in terms of less blood loss, lower morbidity and low opiate analgesia requirement following surgery. 15 SEMS insertion is an outpatient procedure, allows earlier resumption of oral diet, reduces hospital stay and lowers overall cost.2,5,11 In contrast, GJ requires hospital admission and is associated with a higher short-term morbidity and mortality, although it does require fewer re-interventions.2,5,14 Therefore, GJ is mostly offered to patients with a better ECOG (Eastern Cooperative Oncology Group) performance status (ECOG-PS) of 0 or 1 and a longer predicted survival compared with patients with a poorer ECOG-PS and a shorter duration of expected survival, who are better managed with SEMS insertion.2,5 These studies were limited to patients being treated with palliative intent. The long-term complications of SEMS are stent migration and tumour ingrowth/outgrowth, whereas in lap. GJ the most commonly encountered long-term complication is tumour recurrence at anastomotic site, causing obstructive symptoms. In either case, the patient will require re-intervention in the form of another stent placement. In a study by Min et al., 15 the rate of re-intervention is slightly higher in the SEMS group (29) compared with the lap. GJ group, which was 5%. This rate of re-intervention, for the SEMS group, in our study was 42.8%.
GOOSS has been extensively used in studies to compare the degree of clinical effectiveness after SEMS deployment. A GOOSS of 3 at day 7 of stent insertion is considered to be a good marker of stent patency. An earlier study from our institution by Mansoor et al. showed that, for 77 procedures performed on 69 patients, the technical success rate was 97%, with an improvement in GOOSS to 2–3 in 53.6%. 16 Similarly, Piesman et al. and Ye et al. reported attaining GOOSS of 2–3 in 56% and 80.3%, respectively, at day 7 after stent insertion.3,17 The results of our study were comparable, showing an improvement of GOOSS to 2–3 by day 7 in 69.5%, with a technical success rate of 100%.
Regarding the use of stents in GI tumours, Allievi et al. proposed their utility in possible resectable colorectal cancers, causing luminal obstruction. The rationale behind this strategy was to decompress the bowel prior to surgery to allow an uneventful primary anastomosis. Several randomized clinical trials have confirmed this utility of stents as bridge to surgery, thereby making it a standard of care.
16
Although for gastric cancers SEMS placement is recognized as a palliative procedure in relieving outlet obstruction, its role as a bridge to surgery in patients with resectable obstructing gastric tumours is yet to be defined. Only one study by Hala et al., which primarily defined the palliative role of stenting in MGOO, included a small cohort of patients where stenting was done as a bridge to curative surgery. However, postoperative complications and survival were not calculated for this subset, possibly due to the small number of patients:
11
Maintenance of adequate nutritional status by any means is of paramount importance in allowing uninterrupted neo-adjuvant chemotherapy.7,8 Miyabe et al showed that SEMS placement for MGOO in patients undergoing chemotherapy helped ensure an uneventful course, leading to improvement in overall survival in a group of patients with gastric cancer.
9
Ours is the largest study so far reported of patients with obstructing resectable gastric tumours, where SEMS insertion was employed as a bridge to surgery. Our results indicate that stent insertion helped to maintain the nutritional status of our patients during the neo-adjuvant period, as evidenced by stable albumin levels and BMI. Stent insertion in our cohort was not associated with increased risk of post-operative complications when compared with the literature on patients undergoing curative surgery without prior stent insertion (2.8% in our study vs. 9.5%).
18
The use of SEMS as a bridge to surgery was also associated with an increased survival at 1 year following surgery in our patient population, with rates approaching 87.5% as opposed to the best previously reported rate of 81.3%.
19
Conclusion
In our experience, enteral stent insertion leading to relief of MGOO helps maintain nutritional status during neo-adjuvant treatment and improves survival and is not associated with an increased risk of postoperative complications. Therefore, we conclude that SEMS should be used not only as a palliative measure but also as a bridging therapy for patients with obstructing resectable gastric tumours, prior to surgery.
Footnotes
Author contributions
SMS provided study idea; SMS and SB conceived and designed the analysis; MZS and MS were involved in data collection; SS and ANG performed the analysis and data interpretation; SMS and SB were involved in drafting the paper; MAY and SS were involved in critical revision of the article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval/patient consent
Exemption was approved by the Institutional Review Board of Shaukat Khanum Memorial Cancer Hospital and Research Centre Lahore, which is compliant with ICH-GCP guidelines.