
Abstract
Pancreatic cancer with gastrointestinal tract metastasis is a fairly rare occurrence, and gastric metastasis in such cases has been seldom reported. We herein present a case of gastric involvement secondary to pancreatic cancer in a 74-year-old woman in whom the metastatic lesion only presented as mucosal erosion in the stomach. The patient had a 1-month history of progressive right upper quadrant pain before admission. Computed tomography and endoscopic examinations revealed a solid and hypo-enhancing mass in the head of the pancreas. The patient underwent conventional upper endoscopy before pancreatic biopsy, and mucosal erosion was observed in the gastric pylorus. We obtained gastric and pancreatic biopsies by gastroscopy and endoscopic ultrasound-guided fine needle aspiration, respectively. Pathologically, the biopsies taken from the area of gastric erosion showed poorly differentiated invasive adenocarcinoma that was morphologically consistent with the pancreatic specimens. Moreover, the gastric section showed tumor thrombi within the vessels. Hence, the suspected diagnosis was unresectable pancreatic cancer with gastric metastasis. The patient immediately underwent two courses of chemotherapy, but her condition rapidly deteriorated and she died 2 months later.
Introduction
Pancreatic cancer is a rapidly progressing malignancy that affects patients worldwide. Studies have shown that it tends to metastasize to the lymph nodes, liver, lung, and peritoneum, whereas stomach involvement has been seldom reported.1,2 In addition, according to autopsy and clinical series, the incidence of gastric metastasis is only 0.2% to 5.4%.3–5 Hence, gastric metastasis originating from the pancreas is fairly rare in clinical practice. We herein report a case of gastric metastasis from pancreatic cancer that was endoscopically characterized by mucosal erosion alone.
Case presentation
A 74-year-old woman with an unremarkable medical history was found to have a suspected pancreatic mass during a regular medical checkup in December 2018. However, she did not undergo further follow-up because of the absence of specific symptoms. In July 2019, the patient was admitted because of a 1-month history of progressive right upper quadrant pain. She denied any nausea, vomiting, fever, and jaundice during the course of her pain. Physical examination revealed that her abdomen was soft with right epigastric tenderness, and routine hematological tests showed no significant abnormalities. Computed tomography (CT) showed a 3.9- × 3.2-cm solid mass in the pancreatic head, with a mildly dilatated pancreatic duct and multiple nearby swollen lymph nodes (Figure 1(a)). Both the portal vein and splenic vein were encased by the mass. Moreover, abdominal ultrasound, enhanced CT of the chest and abdomen, and magnetic resonance cholangiopancreatography showed that apart from the enlarged lymph nodes, there was no evidence of liver, lung, or peritoneal metastasis. The patient continued to undergo further examination in our department to attain a definitive diagnosis.
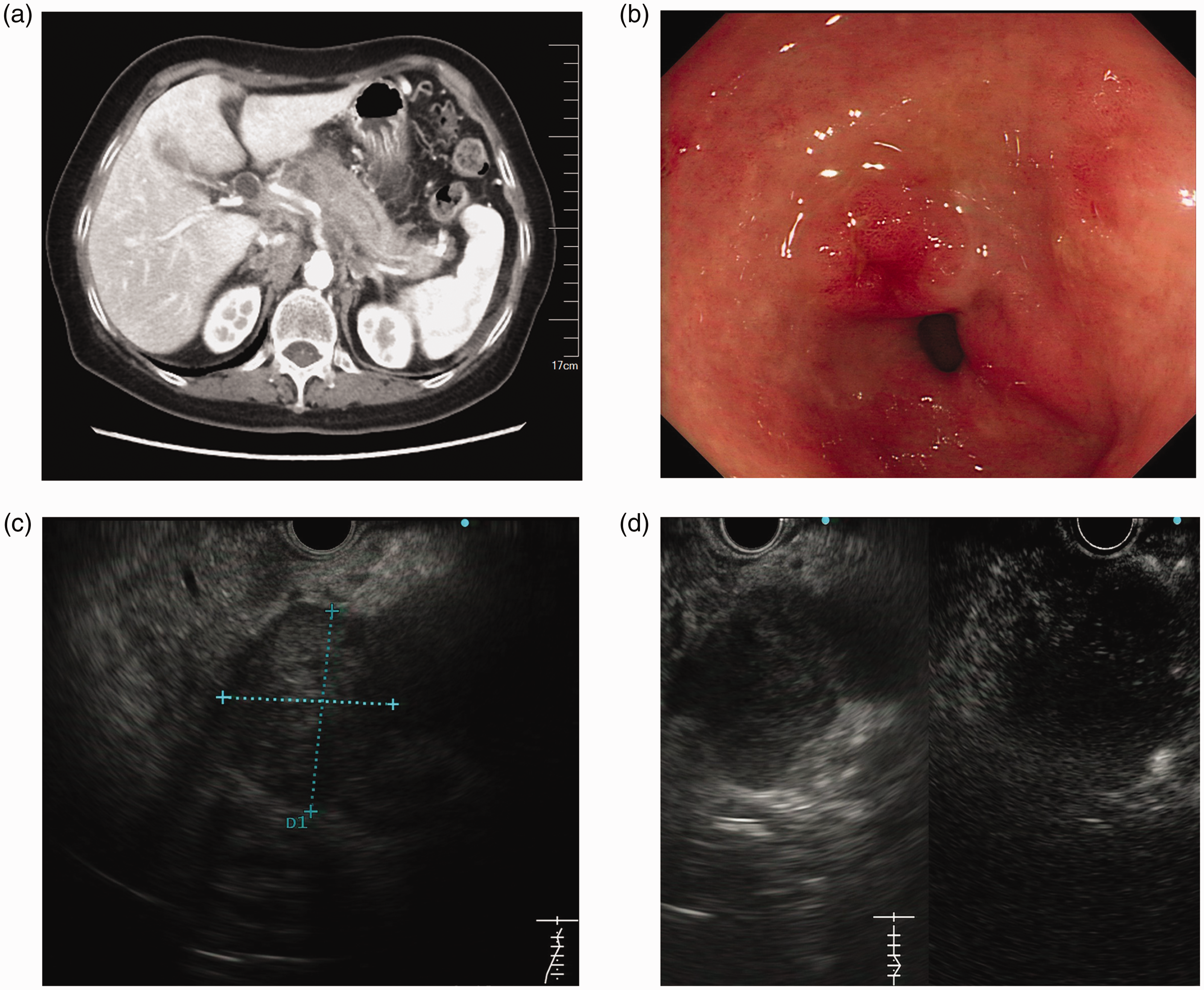
Clinical images and endoscopic manifestations. (a) Computed tomography showed a solid mass in the pancreatic head with a mildly dilatated pancreatic duct. (b) Endoscopic appearance of mucosal erosion in the gastric pylorus. (c) Endoscopic ultrasound showed a hypoechoic lesion in the pancreatic head. (d) Contrast harmonic echo–endoscopic ultrasound showed a hypo-enhancing and inhomogeneous mass.
After admission, the patient underwent conventional upper endoscopy before pancreatic biopsy, and mucosal erosion was observed in the gastric pylorus (Figure 1(b)). Narrow-band imaging showed that the capillary structure and glandular opening morphology of the lesion were generally normal. Forceps biopsies were carried out routinely. We then performed contrast harmonic echo–endoscopic ultrasound, which revealed a hypo-enhancing and inhomogeneous mass measuring 3.6 × 3.1 cm in the pancreatic head (Figure 1(c), (d)). Based on the CT images and endoscopic manifestations, we considered the pancreatic mass to be the primary lesion and performed endoscopic ultrasound-guided fine needle aspiration to obtain a definitive diagnosis. Pathologically, the pancreatic section showed poorly differentiated invasive adenocarcinoma. Moreover, the biopsies taken from the gastric erosion showed that the tumor had invaded the gastric mucosal vessels, and tumor cells were seen growing in sheets in the gastric mucosa; these findings were morphologically consistent with the pancreatic specimens (Figure 2(a), (b)). The surrounding gastric mucosa showed gastritis with no in situ lesions. Moreover, the gastric section revealed tumor thrombi within the vessels, and the tumor cells were eosinophilic (Figure 2(c)). Thus, we reached a final diagnosis of unresectable pancreatic cancer (stage IV according to the American Joint Committee on Cancer TNM staging system) with gastric metastasis. The patient immediately received two courses of chemotherapy with gemcitabine and nab-paclitaxel. However, her CA19-9 level increased and her clinical condition rapidly deteriorated. The patient died 2 months after her first presentation.

Pathological results of the gastric and pancreatic specimens. (a) The tumor had invaded the gastric mucosal vessels, and tumor cells were growing in sheets in the gastric mucosa. The surrounding gastric mucosa showed gastritis with no in situ lesions (hematoxylin–eosin staining, ×100). (b) Poorly differentiated invasive adenocarcinoma of the pancreas (hematoxylin–eosin staining, ×100). (c) Tumor thrombi were seen in the vessels (hematoxylin–eosin staining, ×100).
Discussion
Metastasis to the stomach is generally uncommon. In several large autopsy series, the incidence of this condition reportedly ranged from only 0.2% to 5.4%.3–5 The most prevalent metastatic tumors are derived from lung cancers, breast cancers, and malignant melanoma,5,6 whereas the most frequent sites of metastasis from pancreatic cancer are the lymph nodes, liver, lung, and peritoneum.1,2 Thus, pancreatic cancer with extrapancreatic metastasis to the stomach is rarely encountered in clinical practice. Oda et al. 5 reported that only two cases of gastric metastasis were identified in a series of autopsies performed on 209 patients with pancreatic cancer. In the current report, we presented a case of gastric metastasis from pancreatic cancer that was merely characterized by mucosal erosion endoscopically. This case has some guiding significance for clinical diagnosis.
Because of the low sensitivity of imaging examinations, most patients with pancreatic cancer (including those with metastatic gastric tumors) die of their primary lesions before clinical detection. As a result, the actual incidence of gastric metastasis from pancreatic cancer and the interval time from clinical detection to death are difficult to assess. Moreover, at the time of endoscopic examination and necropsy, metastatic tumors to the stomach may have variable manifestations, and most of them have been found to be polypoid or ulcerated with “volcano-like” lesions.4,7,8 Chelimilla et al. 9 described a patient with a large gastric fundic ulcer secondary to direct invasion from pancreatic adenocarcinoma. Sasajima et al. 10 subsequently described a patient with hematogenous gastric metastasis from pancreatic cancer in whom two solid masses were detected in the submucosal layer, with preserved integrity of the gastric mucosa. Other cases of gastric metastasis that occurred 1 to 4 years after surgery for pancreatic cancer have also been presented in several reports.11–13 In our patient, the metastatic lesion only presented as mucosal erosion in the stomach, which has not been previously reported. This endoscopic manifestation also indicates that the pancreatic cancer was advanced at the time of diagnosis.
Because endoscopic biopsy and brush cytology can provide valuable pathologic information, both gastric and pancreatic biopsies were obtained in this case. Gastric involvement may occur by different pathways, 11 including direct invasion, hematogenous spread, lymphatic metastases, intramural or intraluminal dissemination, and intraoperative seeding, and it is quite important to differentiate the primary site of tumor origin. In the present case, the primary pancreatic head carcinoma was not anatomically near the gastric erosion, and CT images and endoscopic ultrasound did not reveal that the pancreatic mass had directly infiltrated the gastric antrum. Additionally, the forceps biopsies were carried out before aspiration, which might have eliminated the possibility of metastasis by needle tract implantation. Moreover, the biopsies taken from the gastric erosion showed poorly differentiated invasive adenocarcinoma with tumor cells growing in sheets in the gastric mucosa, which was morphologically consistent with the pancreatic specimens. Therefore, we further ruled out the possibility of double cancer. Finally, by combining the clinical history with the pathological results, we determined that the metastasis had originated from the pancreas and spread to the stomach. It is also worth mentioning that because neither umbilication/central dimpling nor a macroscopic/microscopic opening was visualized on the surface by gastroscopy and narrow-band imaging, we considered a heterochronous primary pancreatic cancer originating from a gastric heterotopic pancreas to be unlikely. 14
Conclusion
This report describes a rare case of gastric metastasis from pancreatic cancer that was merely characterized by mucosal erosion. Although pancreatic cancer with gastric metastasis is fairly rare, the prognosis is almost invariably poor. Endoscopic examination with adequate biopsies plays an important role in the detection, evaluation, and accurate diagnosis of such cases.
Footnotes
Ethics
This manuscript was carefully prepared according to the CARE Checklist. 15 Ethics committee approval was not required because we presented only one case of a rare condition.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Medical Science and Technology Development Foundation, Nanjing Department of Health (Grant Numbers: ZKX18022, YKK17077), and Natural Science Foundation of Jiangsu Province (Grant Number: SBK2019022491).
Author contributions
Manuscript drafting: Jie Yang
Medical record data: Yue Yuan
Conception and design: Jie Yang and Ying Lv
Image analysis: Shu Zhang
Manuscript revision and funding acquisition: Ying Lv