
Abstract
Radical resection with or without adjuvant chemotherapy is a common option for stage II and III colorectal cancer. Few reports exist regarding gastric tumorigenesis, including gastric cancer, gastric intraepithelial neoplasia, and gastric stromal tumor, in patients who received this protocol as the standard treatment for colorectal cancer. We present two cases of gastric tumorigenesis in patients with colorectal cancer following radical resection combined with adjuvant chemotherapy. Both patients underwent gastrectomy and D2 lymphadenectomy for their gastric tumors; neither patient developed recurrence up to 2 years after treatment. These cases indicate that patients should be monitored closely for gastric tumorigenesis after treatment for colorectal cancer. Early detection and active surgical treatment can provide satisfactory results for colorectal cancer followed by gastric tumorigenesis. Long-term follow-up and regular examinations, especially gastroscopy, are necessary to detect gastric tumorigenesis after colorectal cancer. The focus on monitoring colorectal cancer alone in colorectal cancer patients should be changed to include a broader range of cancers in addition to precancers and other tumors, such as gastric stromal tumor.
Keywords
Introduction
Currently, colorectal cancer is the third most common cancer worldwide, with approximately 1.80 million new cases and 0.86 million deaths each year.1–4 Traditional and emerging treatments for colorectal cancer described in the National Comprehensive Cancer Network (NCCN) clinical practice guidelines include surgery, chemotherapy, radiotherapy, and immunotherapy. The standard treatment regime includes radical resection and adjuvant chemotherapy, which are commonly used to treat patients with stage II and III colorectal cancer.3,5,6 Patients usually benefit from this therapeutic strategy, with a low incidence of recurrence. Gastric tumorigenesis, including gastric cancer, gastric intraepithelial neoplasia, and gastric stromal tumors, after radical resection combined with adjuvant chemotherapy, is uncommon. Here, we present two such cases and discuss the pathogenesis, clinical manifestation, examination, and treatment of these patients.
Case presentation
Case 1
A 58-year-old man presented to the Second Hospital of Jilin University (Changchun, Jilin, China) after suffering lower abdominal pain for 2 months. No obvious abnormalities were identified on physical examination. Concentrations of the serum tumor markers, carcinoembryonic antigen (CEA), alpha-fetoprotein (AFP), and carbohydrate antigen19-9 (CA19-9) were within their respective normal ranges. Colonoscopy performed at the patient’s local hospital revealed a circumferential tumor located 50 cm from the anal verge, and biopsy revealed a moderately differentiated adenocarcinoma. During hospitalization, abdominal and pelvic computed tomography (CT) indicated thickening of the left transverse colonic wall with associated stenosis (Figure 1). The patient then underwent laparoscopic-assisted radical left hemicolectomy. Postoperative pathology revealed moderately differentiated adenocarcinoma with a minor component of mucinous adenocarcinoma (Figure 2a). Although the tumor had invaded all layers of the colonic wall, none of the lymph nodes were positive; therefore, the tumor/node/metastasis (TNM) staging was T3N0M0. Immunohistochemical analysis demonstrated that the tumor was BRAF V600E mutation-negative, but CDX2-, MLH1-, MSH2-, MSH6-, and PMS2-positive (Figure 2b–f). The patient subsequently received six cycles of XELOX (capecitabine [XELODA; Roche, Shanghai, China] and oxaliplatin (Oxaliplatin; Hengrui, Jiangsu, China) chemotherapy and was discharged from the hospital. He attended regular follow-up examinations every 2 to 4 months, thereafter.
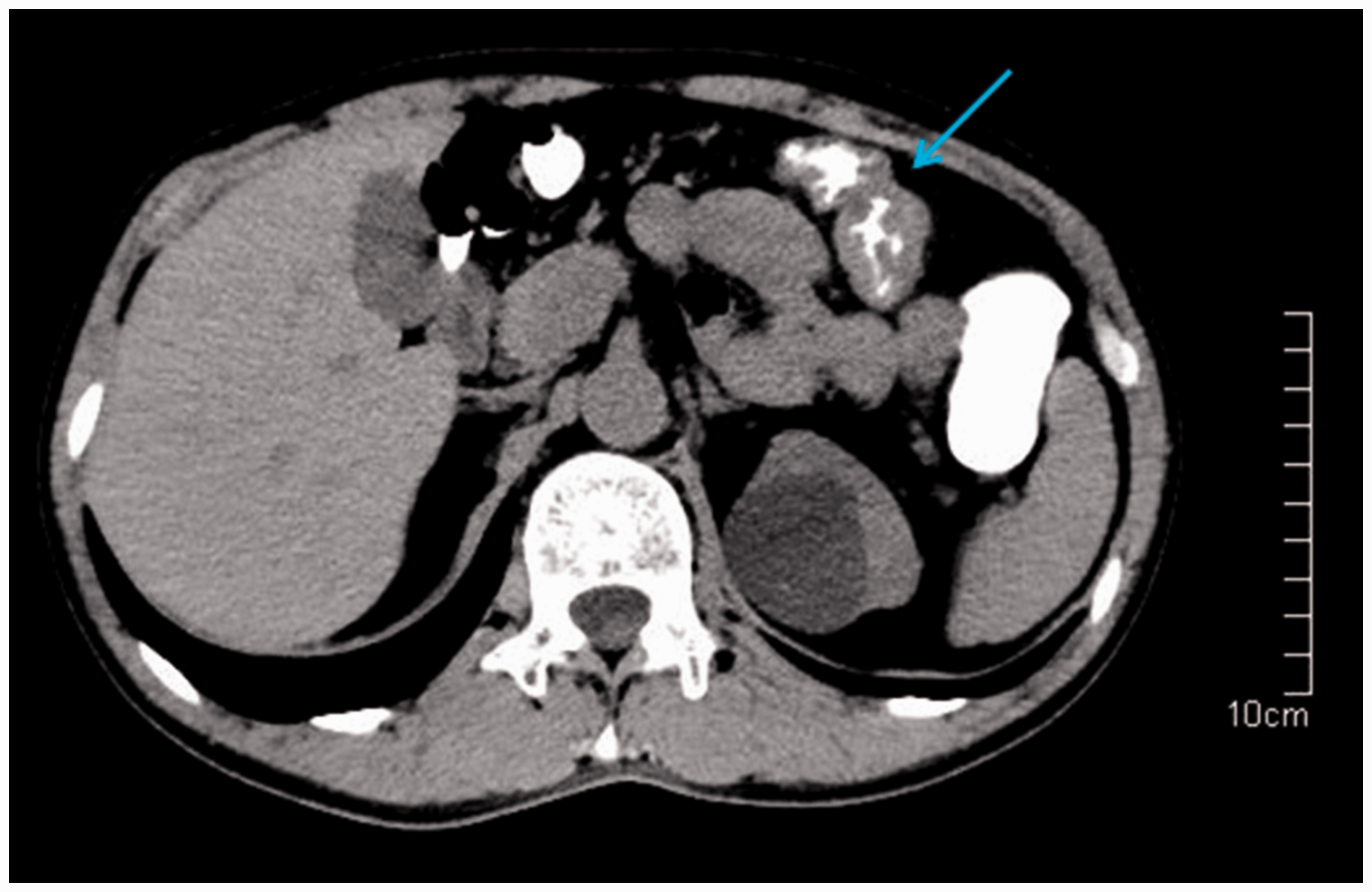
Imaging findings. Abdominal computed tomography (CT) image showing thickening in the left transverse colon.

Histopathological and immunohistochemical findings. (a) Postoperative pathology revealing a moderately differentiated adenocarcinoma with a minor component of mucinous adenocarcinoma. (b) CDX2-positive. (c) MLH1-positive. (d) MSH2-positive. (e) MSH6-positive. (f) PMS2-positive. (g) Postoperative pathology demonstrating a signet-ring cell carcinoma of the diffuse type in Lauren’s classification. (h) ABPAS-positive. (i) MUC5ac-positive. Hematoxylin and eosin staining, magnification ×100; immunohistochemical staining, ×100.
No obvious abnormalities were identified during 2 years of regular follow-up examinations, until gastroscopy indicated an area of rough mucosa (diameter: 2.0 cm) with a central concavity and erosion, on the lesser curvature. Endoscopic ultrasonography showed thickened mucosa. Concentrations of the serum tumor markers, CEA, AFP, and CA19-9 were within their respective normal ranges. According to the pathological and immunohistochemical findings, CDX2-negative signet-ring cell carcinoma was diagnosed. The patient then underwent gastrectomy and D2 lymphadenectomy (D2 radical gastrectomy). Postoperative pathology demonstrated a signet-ring cell carcinoma of the diffuse-type in Lauren’s classification (Figure 2g). The tumor was confined to the mucosa, and none of the lymph nodes were positive; therefore, the TNM staging was T1aN0M0. Immunohistochemical analysis demonstrated that the tumor was CDX2-negative, but alcian blue/periodic acid-Schiff (AB/PAS)-, MUC5ac- (Figure 2h–i), MLH1-, MSH2-, MSH6-, and PMS2-positive. The patient received no other treatment but attended regular follow-up examinations every few months. After 2 years, the patient remained well.
Case 2
A 65-year-old man presented to our hospital complaining of loose stool for 5 days and hematochezia for 1 day. No obvious abnormalities were identified on physical examination. The concentrations of the serum tumor markers, CEA, AFP, and CA19-9, were within their respective normal ranges. Colonoscopy performed at his local hospital revealed a hyperplastic tumor located 10 cm from the anal verge in addition to scattered polyps across the entire colorectum. Pathologic examination indicated that the hyperplastic tumor was a moderately differentiated adenocarcinoma. One of the polyps was a high-grade dysplasia located 80 cm from the anal verge, and the other polyps were adenomas. CT imaging showed thickening of the rectal wall (Figure 3). The patient underwent endoscopic mucosal resection (EMR) to treat the adenomas. After recovery, he underwent laparoscopic-assisted radical rectal resection (Dixon procedure) and radical right hemicolectomy. Postoperative pathology revealed a moderately differentiated rectal adenocarcinoma with a component of mucinous adenocarcinoma and a moderately differentiated colonic adenocarcinoma (Figure 4a–b). The rectal tumor invaded all layers of the wall, and perirectal lymph nodes were positive (2/14); therefore, the TNM staging was T3N1M0. The colon cancer invaded the submucosa, and none of the lymph nodes was positive; therefore, the TNM staging was T1N0M0. Immunohistochemical analysis demonstrated that the tumor was BRAF V600E mutation-negative, but CDX2-, MLH1-, MSH2-, MSH6-, and PMS2-positive (Figure 4c–g). The patient subsequently received six cycles of XELOX chemotherapy and was discharged from the hospital. He attended regular follow-up examinations every 3 to 6 months. One year later, he underwent repeat EMR for the colorectal polyps, which were identified as adenomas by pathologic examination.

Imaging findings. Abdominal computed tomography (CT) showing thickening of the rectal wall.

Histopathological and immunohistochemical findings. (a) Postoperative pathology demonstrating a moderately differentiated rectal adenocarcinoma with a component of mucinous adenocarcinoma. (b) Moderately differentiated colonic adenocarcinoma. (c) CDX2-positive. (d) MLH1-positive. (e) MSH2-positive. (f) MSH6-positive. (g) PMS2-positive. (h) Postoperative pathology showing low- and high-grade intraepithelial neoplasms with intestinal metaplasia. (i) Gastric stromal tumor. (j) CD117-positive. (k) CD34-positive. (l) DOG1-positive. Hematoxylin and eosin staining, magnification ×100; immunohistochemical staining, ×100.
No further abnormalities were detected during follow-up until gastroscopy conducted 2 years after the colorectal surgery indicated an ulcer (1.4 cm × 0.7 cm) on the anterior wall of the gastric antrum and a protuberant lesion (0.6 cm × 0.6 cm) on the gastric fundus. The CA 50 concentration was 146.73 U/mL (normal range: 0–20 U/mL). Furthermore, colonoscopy indicated multiple colorectal polyps, and high-frequency electrocoagulation combined with argon plasma coagulation was performed during the colonoscopy procedure to remove the polyps. Pathological analysis suggested a malignancy of the gastric antrum, and the patient then underwent D2 radical gastrectomy and local resection of the gastric fundus neoplasm. Postoperative pathology demonstrated low- and high-grade intraepithelial neoplasms with intestinal metaplasia on the gastric antrum and a low-risk gastrointestinal stromal tumor (GIST) with a karyokinesis count of <5/50 in high-power field evaluation of the gastric fundus (Figure 4h–i). Immunohistochemical analysis revealed that that the tumor was cluster of differentiation (CD)117-, CD34-, and DOG1-positive (Figure 4j–l), but desmin-, smooth muscle actin (SMA)-, neuron-specific enolase (NSE)-, and S-100-negative, with Ki67 <1%. Six months later, colonoscopy indicated two rectal polyps, which were treated by high-frequency electrocoagulation combined with argon plasma coagulation. Seventeen months after the gastric surgery, the patient had recovered well.
The details and immunohistochemical analysis results for both cases are shown in Tables 1 to 4.
The patients’ demographic and tumor data.

Immunohistochemical analysis of the colon cancers.

Immunohistochemical analysis of the gastric cancer.

Immunohistochemical analysis of the gastric stromal tumor.

Discussion
The cases presented here highlight the importance of monitoring a broader range of tumors after treatment for colorectal cancer. Patients with stage II and III colorectal cancer usually receive radical resection with or without adjuvant chemotherapy, depending on the presence of risk factors in stage II cancer. According to the European and Japanese guidelines, these risk factors are poor differentiation; <12 resected lymph nodes; vascular, lymphatic or perineural tumor invasion; obstructive or perforated tumors; and T4 stage.3,5,6
Standard treatments maximize the benefits to patients; however, drug resistance is an unresolved issue with therapeutic advancements. Several mechanisms of drug resistance in colorectal cancer have been reported, such as limited drug transport in the tumor. 7 Drug metabolism, apoptosis, and microRNA levels are also involved.7,8 Drug resistance decreases the therapeutic effects and increases the possibility of recurrence and metastasis. Although the possibility of recurrence and metastasis is inevitable, gastric tumorigenesis is a rare phenomenon. It is worth mentioning that the incidence of gastric cancer is disproportionately high in East Asian countries,9,10 and this is the most common secondary cancer in East Asian colorectal cancer patients.11–13 According to Yoon et al., 11 the incidence of gastric cancer is 0.61% in patients with previous colorectal cancer, and mutations in p53 and microsatellite instability (MSI) in colorectal cancer may be key factors related to secondary gastric cancer.11,14
p53 mutations, which are common in gastric and colorectal cancer, correlate with the depth of tumor invasion in gastric cancer.15,16 Translocations in chromosome 17 and at the p53 locus may contribute to secondary cancer in colorectal cancer. 17 Yun et al. 14 reported that secondary cancers occur with relatively high frequency in colorectal cancer patients and proposed that MSI might be a useful predictive marker. Interestingly, Kim et al. 18 proposed that p53 and MSI are not useful markers for predicting colorectal cancer in gastric cancer patients. In the cases presented here, p53 was either absent or weakly expressed, and microsatellite stability (MSS) was confirmed, suggesting that strong positive expression of p53 might be more meaningful. In addition, a variety of p53 mutations have been identified, which are difficult to detect individually, especially in rare mutations. Some patients are also reluctant to incur the additional cost associated with identifying mutations. In addition, gastric cancer is more likely to occur in MSI colorectal cancer patients, although it can also occur in MSS patients.
Some studies have indicated that chemotherapy may increase the risk of cancer.19–21 Although these studies did not involve colorectal cancer followed by gastric cancer, a parallel phenomenon cannot be excluded. The patients described in this report received XELOX chemotherapy after surgery.
As a heterogeneous disease, there is an urgent need to develop biomarkers for colorectal cancer, and the biomarkers should have potential predictive or prognostic value. Based on the molecular biomarkers, personalized treatment for colorectal cancer patients can also be explored.7,22 Usually, patients with advanced cancer have a poor prognosis, whereas those with early-stage cancer experience longer survival. Early stage, well- or moderately differentiated tumors and no lymphovascular invasion imply a positive prognosis with longer survival. However, secondary cancers are more likely to occur in these patients. The colorectal cancer stages in our patients were stage II (Case 1: T3N0M0) and III combined with I (Case 2: T3N1M0 combined with T1N0M0); both patients showed moderate differentiation and no lymphovascular invasion.
The onset of gastric cancer is usually insidious, making regular examination indispensable for colorectal patients after treatment. These patients tend to be older, with a lower body mass index and a higher incidence of peritoneal metastasis than patients with colorectal cancer alone. In addition, the pathologic type is more likely to be undifferentiated and signet-ring cell carcinoma. 23 Active surgery is the most common intervention in this situation. Effective management and surveillance of postoperative colorectal cancer patients improves early lesion detection and allows prompt treatment and an improved prognosis. Such precancerous lesions include gastric intraepithelial neoplasia, also known as dysplasia, which is classified as low- and high-grade.
The reported prevalence of gastric intraepithelial neoplasia is between 9% and 20% in high incidence regions,24,25 and these tumors are usually found in the antrum.25,26 Both low- and high-grade intraepithelial neoplasms have an increased risk of malignancy. According to guidelines published by groups such as the British Society of Gastroenterology, the American Society for Gastrointestinal Endoscopy, and a number of European societies,25–28 both low- and high-grade intraepithelial neoplasms require complete removal. However, there is some controversy regarding this requirement for low-grade intraepithelial neoplasia because of the lower risk of malignant transformation.25,29,30
The surveillance of postoperative colorectal cancer patients is also beneficial for early detection of GIST, which is the most frequent mesenchymal tumor in the gastrointestinal tract and which can also exist synchronously or metachronously in colorectal cancer patients.31,32 The standard treatment for GIST without metastasis is radical resection, and the risk stratification for GIST is according to tumor size, mitotic index, and Ki67 level.33–35 Approximately 44% of patients have high-risk GIST, whereas low- and very-low-risk GIST, as in our case, account for 32% of cases. 35 The 5-year recurrence-free survival rate after surgery is estimated at 59.9%, and the prognosis of GIST is associated with early diagnosis and R0 resection. 33 A series of colorectal cancer cases that developed gastric tumorigenesis are summarized in Table 5.36–40
Series of colorectal cancer cases developing gastric tumorigenesis.

GIST, gastrointestinal stromal tumor.
The cases reported here are also partly consistent with multiple primary malignant neoplasms (MPMN), first standardized by Warren and Gates, and defined as two or more malignant tumors from different sites in an individual over a period of time.41,42 Warren and Gates defined MPMN according to the following criteria: (1) each tumor must be malignant according to histology; (2) each tumor must be distinct from the other tumors; and (3) tumors must not be metastases from other tumors. If the time between the diagnoses of the two primary malignant neoplasms is less than 6 months, the MPMN are considered synchronous, but if the time is longer than 6 months, the MPMN are considered metachronous.41,43
Conclusion
Following treatment for colorectal cancer, patients should be monitored for gastric tumorigenesis, including gastric cancer, gastric intraepithelial neoplasia, and gastric stromal tumors. Gastroscopy plays a crucial role in regular long-term follow-up examinations, and early detection and prompt treatment can improve the patients’ prognosis.
Footnotes
Ethics statement
This case report was approved by the Ethics Committees of the Second Hospital of Jilin University (Changchun, China; approval number: 2020091). Written informed consent was obtained from the patients for publication of this case report.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Science and Technology Department of Jilin Province, China (No. 20180101130JC).