
Abstract
Achalasia is a primary esophageal motility disorder characterized by the loss of inhibitory neurons in the myenteric plexus, resulting in impaired relaxation of the esophagogastric junction. Achalasia is an incurable disease, and the treatment modalities are aimed at disruption of the esophagogastric junction and vary widely from pharmacological to endoscopic to surgical. Traditional endoscopic therapy includes pneumatic dilation, botulinum toxin injection, and peroral endoscopic myotomy. This review aims to provide an overview of the endoscopic management of achalasia, while focusing on the utilization of peroral endoscopic myotomy and other novel approaches.
Introduction
Achalasia is a primary esophageal motility disorder characterized by the loss of inhibitory neurons in the myenteric plexus, resulting in impaired relaxation of the esophagogastric junction (EGJ).1,2 Heartburn, dysphagia, and regurgitation are common presenting symptoms. Worldwide, the incidence ranges from 0.03 to 1.63 per 100,000 persons per year.1,2 Achalasia affects males and females equally with no racial predominance. Endoscopy, barium esophagram, and esophageal manometry are the three modalities utilized to diagnose achalasia with the gold standard being esophageal manometry.2,3 Achalasia is an incurable disease and treatment modalities are focused on reducing the lower esophageal sphincter (LES) pressure and improving symptoms. Treatments range from pharmacological to endoscopic to surgical.
Pharmacologic treatments include calcium channel blockers, nitrates, anticholinergics, beta-adrenergic agonists, and theophylline. 2 Pharmacologic therapy is often reserved for patients who are not candidates for surgical or endoscopic treatment. Traditional endoscopic therapy includes botulinum toxin injection, pneumatic dilation (PD) and peroral endoscopic myotomy (POEM).1,2 Novel treatment using a hydrostatic dilation balloon (EsoFLIP; Medtronic, Inc., Shoreview, MN, USA) has been recently described. The traditional surgical treatment is Heller myotomy. 2
The ideal treatment for achalasia continues to be a debated topic. The aim of this review is to provide an overview of the endoscopic management of achalasia, while focusing on the utilization of POEM and other novel approaches.
Endoscopic approaches
Pneumatic dilation (PD)
PD has been viewed as the standard of care for the treatment of achalasia. The conventional approach is graded dilation using 30-, 35-, and 40-mm polyethylene balloons. 2 Adverse outcomes include esophageal perforation [2.8%; 95% confidence interval (CI): 2.3–3.5%] and bleeding (2%; 95% CI: 1–4%).1,2 Gastroesophageal reflux disease (GERD) is a common postprocedure complaint (9% at 6 months follow-up). 1 There is no standardized treatment protocol for PD. A meta-analysis by van Hoeij and colleagues 4 included 10 studies with 643 patients comparing the efficacy between different balloon sizes and different dilation protocols. Dilation with 30- and 35-mm balloons showed comparable mean remission rates at 6 months (81% and 79%). When a 40-mm balloon was utilized, a higher remission rate of 90% was observed. However, these remission rates decreased significantly in all groups after 12 months (77% for 30 mm, 70% for 35 mm, and 87% for 40 mm). Furthermore, as needed dilations were more effective than predefined dilation timelines (86% versus 75% at 12 months).
A longitudinal cohort study by Müller and colleagues 5 focused on the long-term success of a single PD. Ninety-one patients were successfully treated with a single PD. Fifty-four percent of the patients experienced a clinical relapse during a mean follow-up time of 13.8 years. The success rates declined dramatically from 2 to 25 years (64–36%). Predictors of symptom recurrence included age <40 years, posttreatment LES >15 mm Hg, cardia width <5 mm and an esophageal barium column height >1 cm 4 to 12 weeks postdilation. In addition, achalasia type has been found to predict the therapeutic response to PD. Pratap and colleagues 6 in their study demonstrated that patients with type II achalasia had the best response to PD (90%) compared with types I (63.3%) and III (33.3%).
When compared with laparoscopic Heller myotomy (LHM), PD has proven to be equivalent. In their study, Boeckxstaens and colleagues 7 divided patients with newly diagnosed achalasia to treatment with PD or LHM with Dor’s fundoplication. After 1 year, the rate of therapeutic success was 90% in the PD group and 93% in the LHM group (p = 0.46). Therapeutic success remained similar at 2 years (86% in PD versus 90% in LHM). This landmark trial concluded that LHM did not have superior rates of therapeutic success compared with PD. More recently, a meta-analysis by Hao-Ran Wang and colleagues evaluated five studies with 498 patients and determined there was no significant difference in remission rate between LHM and PD at 2 and 5 years (1.05; 95% CI: 0.91–1.22% and 1.17; 95% CI: 0.84–1.64). PD appears to be a safe and effective treatment; however, success may wane with time requiring additional treatments.
PD is best suited for patients with type II achalasia.6,8 Older patients tend to have better rates of remission compared with patients younger than 40 years (58% versus 16% at 5 years). 9 Males experience a worse outcome after PD compared with females and as such may require a higher initial balloon diameter (35 mm versus 30 mm).10,11 Furthermore, PD is a cost-effective treatment modality for type II achalasia despite the waning efficacy over time.7,12 Over a 4- to 6-year period, one-third of the patients have recurrence of their symptoms and require retreatment.13,14 PD can be performed safely in patients who have relapsed postsurgical myotomy. However, the response to dilation is not as robust as seen in patients who are treatment naïve (50% versus 74% of previously untreated patients. 15
Botulinum toxin injection
Endoscopic injection of botulinum toxin (EBTI) is effective in treating achalasia by inhibiting the release of acetylcholine from the nerve endings and reducing the LES pressure.1,2,16 EBTI is performed by injecting 100 units of botulinum toxin above the gastroesophageal junction (GEJ). It is a generally safe procedure with scarce adverse events which include chest pain, allergic reactions, and mediastinitis.1,2 However, the efficacy of EBTI decreases rapidly with time. A large meta-analysis by Campos and colleagues 17 reviewed 105 studies which included 7855 patients and found symptom relief in 78.7% of patients at 1 month. However, this improvement was short lived with relief in only 70% of patients at 3 months, 53.3% at 6 months, and 40.6% at 12 months or longer. Approximately half of the patients required a second EBTI. A randomized controlled trial (RCT) showed that two planned injections 1 month apart were significantly better than a single injection for symptom relief (81% versus 52%). 18
When comparing EBTI with PD, a meta-analysis of seven studies and 178 patients showed no significant difference between the two therapies for the first 4 weeks following initial treatment. 19 At 6 and 12 months, more patients in the PD group were in remission compared with the EBTI group. As expected, LHM had a superior 1-year response rate compared with EBTI (83% versus 65%). 16 Overall, EBTI is a safe therapy with infrequent complications. The limitation of this treatment is the short symptomatic relief requiring additional treatments. Furthermore, with continued botulinum toxin injections, there is a concern for intramural fibrosis which can complicate other subsequent treatment modalities.2,17
EBTI is regarded as a short-term treatment option for achalasia patients who are at high risk for other definitive therapies because of comorbidities or advanced age.1,20 Predictors of response lasting more than 3 months include age >50 years (82% versus 43%) and patients with vigorous compared with classic achalasia (100% versus 52%)—a manometric feature that is no longer in use. 21
Peroral endoscopic myotomy (POEM)
POEM is a novel technique for the treatment of achalasia inspired by the concept of natural orifice transluminal endoscopic surgery (NOTES). 22 It requires the creation of a submucosal space to access the circular and longitudinal muscle fibers and perform selective or complete myotomy using a specialized knife (Figure 1). 2 The muscle must be cut at least 6 cm into the esophagus and 2 cm below the squamocolumnar junction onto the cardia. 2 One benefit of POEM is that the length of myotomy can be tailored for each patient. The index study evaluating the efficacy of POEM was published in 2010 by Inoue and colleagues. 22 POEM was performed on 17 consecutive patients with achalasia and resulted in a significantly reduced dysphagia symptom score from a mean of 10 to 1.3 (p = 0.0003) with no serious complications. The resting LES pressure also significantly reduced from a mean of 52.4 to 19.9 mm Hg (p = 0.0001). In the 5 months following treatment, only one patient required additional intervention due to the development of reflux esophagitis which responded to proton pump inhibitors.

Steps of the peroral endoscopic myotomy (POEM) technique: (a) submucosal bleb and incision, (b) creation of submucosal tunnel, (c) selective myotomy of inner circular muscle, (d) myotomy of the lower esophageal sphincter, (e) complete myotomy, and (f) endoclip closure.
In a meta-analysis reviewing 19 studies by Talukdar and colleagues, POEM was associated with a significant reduction in Eckardt’s score (ES) of −7.95 (p < 0.0001) and significant improvement in the resting LES pressure with an overall effect size of −7.28 (p < 0.0001). Notably, there was significant heterogeneity between the studies for both endpoints (I2 = 78.33%; p < 0.0001 and I2 = 75.68%; p < 0.0001, respectively). 23 Similar results were shown in a more recent meta-analysis by Evensen and colleagues 24 evaluating POEM outcomes in treatment naïve patients. They included seven studies with a total of 434 patients. Clinical success was defined as an ES ⩽3. Seven articles were included in the analysis revealing short-term clinical success rate >90%.
In numerous studies including meta-analyses, case–control studies, and an RCT, POEM has been shown to be equivalent to LHM and excelled when compared with the other available endoscopic treatment options for achalasia. An early meta-analysis in 2014 showed no significant difference between POEM and LHM in terms of reduction in ES, postoperative pain scores, length of hospital stay, adverse events, and symptomatic GERD. 23 In their large meta-analysis, Schlottman and colleagues 25 reviewed 53 studies (5834 patients) on LHM and 21 (1958 patients) on POEM to evaluate differences in outcomes between the two modalities. Mean follow-up time was significantly longer for LHM than POEM (41.5 versus 16.2 months, p < 0.0001). Dysphagia improved in 93.2% of patients undergoing POEM compared with 87.7% of patients undergoing LHM. A logistic model for improvement in dysphagia at 12 and 24 months showed a more significant improvement in dysphagia symptoms in the POEM cohort (93.5% for POEM versus 91.0% for LHM, p = 0.01 at 12 months; 92.7% versus 90.0%, p = 0.01 at 24 months). Nevertheless, POEM was associated with a higher risk of GERD symptoms compared with LHM [odds ratio (OR) 1.69, 95% CI: 1.33–2.14, p < 0.0001].
Werner and colleagues 26 performed a noninferiority, multicenter, randomized trial comparing POEM with LHM plus Dor fundoplication (LHD) for 221 patients with symptomatic achalasia who were followed for 2 years. The primary outcome, defined as an ES ⩽3 without the use of additional treatments, was seen in 83.0% of the POEM cohort and 81.7% of the LHM cohort (difference, 1.4 percentage points; 95% CI: −8.7 to 11.4; p = 0.007 for noninferiority). Improvement in esophageal function and Gastrointestinal Quality of Life Index did not differ significantly between the two groups. Reflux esophagitis troubled the POEM group more frequently than the LHD group throughout the duration of the study (57% versus 20% at 3 months, 44% versus 29% at 24 months). High-grade esophagitis (Los Angeles Classification grade C or D) was observed in 6% of the POEM group at 3 months and 3% of the LHM group. At 24 months, this difference shifted with 5% in the POEM group and 6% in the LHM group. Interestingly, esophageal pH monitoring showed a similar amount of patients in each group with abnormal reflux at both time points. At 3 months, 44% in the POEM group and 33% in the LHM group had abnormal reflux. At 24 months, both groups were at 30%. Similar results were observed in a case–control study from two high-volume centers evaluating POEM versus LHD over 4 years follow-up time with more than 90% enduring success for both treatment options. 27
When compared with PD, limited literature suggests that POEM may be more effective for the treatment of achalasia. The most robust evidence to suggest this comes from a randomized clinical trial by Ponds and colleagues 28 evaluating treatment outcomes of POEM versus PD in treatment naïve patients. Ninety-two percent of patients in the POEM group achieved treatment success defined as ES ⩽3 and the absence of severe complications or need for retreatment compared with 54% in the PD group. Surprisingly, there was no significant difference in the posttreatment median integrated relaxation pressure (9.9 mm Hg in POEM group versus 12.6 mm Hg in PD; difference 2.7 mm Hg, 95% CI: −2.1 to 7.5, p = 0.07). Reflux esophagitis was notably more frequent in the POEM group (41% versus 7%; difference 34%, 95% CI: 12–49%, p = 0.002). At the 2-year follow-up, 35% of the POEM cohort were assigned grade A–B esophagitis and 7% were assigned grade C. The PD group only had 7% of patients with reflux and all were assigned grade A.
Despite the benefits previously described, POEM presents with inherent risks, some of which are clinically inconsequential. Adverse events include mucosal injury (4.8%, 95% CI: 2.0–8.5%), esophageal perforation (0.2%, 95% CI: 0–1.1%), bleeding (0.2%, 95% CI: 0–1.4%), subcutaneous emphysema (7.5%, 95% CI: 3.5–12%), pneumothorax (1.2%, 95% CI: 0.1–4.3%), pneumomediastinum (1.1%, 95% CI: 0.1–4.7%), pneumoperitoneum (6.8%, 95% CI: 1.9–14%), and pleural effusions (1.2%, 95% CI: 0–8.3%).1,2,29 However, the most common complaint postprocedure is GERD which is estimated to occur in over half of the patients undergoing treatment. 2 A consensus statement regarding GERD after POEM was published in 2019. 30 Currently, there is no agreed upon incidence of GERD following POEM. Furthermore, there is limited literature evaluating if postprocedure GERD can lead to stenosis, Barrett’s or esophageal cancer. In 2019, a case report was published by Ichkhanian and colleagues 31 discussing a case of de novo Barrett’s esophagus with esophageal adenocarcinoma in a patient 4 years post POEM. This case highlights the long-term risk of GERD following POEM. Luckily, most patients with GERD do respond to PPI therapy. 30 It is hypothesized that GERD stems from excessive gastric myotomy and incision of the collar sling fibers. The double-scope method, which uses an ultrathin endoscope to observe the extent of submucosal tunneling at the gastric cardia, can be utilized to confirm the length and direction of myotomy. For cases of refractory GERD, endoscopic and surgical partial fundoplication are available options. Tyberg and colleagues 32 published their experience of performing transoral incisionless fundoplication (TIF) on patients who had previously underwent POEM. Five patients were included in their study with 100% technical success and discontinuation of PPI therapy in all patients.
Achalasia is a diagnosis without a cure and as such, treatment failure is a known problem. Two scoring systems have been proposed aiming to determine risk of clinical failure following POEM.
Liu and colleagues 33 proposed a risk-scoring system (Zhongshan POEM Score) based on prior history, clinical symptoms, and intraprocedural findings. A total of 1538 patients were included in this single-center retrospective analysis. These patients were divided into the training cohort (n = 769) or the internal validation cohort (n = 769). During the median follow-up time of 42 months, 109 patients had clinical failure (55 in the training cohort versus 54 in the validation cohort). Multivariate analysis revealed that previous treatment, intraprocedural mucosal injury, and clinical reflux were independent risk factors for clinical failure. These risk factors were assigned the following points: previous treatment (2 points), type I mucosal injury (2 points), type II mucosal injury (6 points), and clinical reflux (3 points). The risk score ranged from 0 to 11 points with higher scores corresponding to higher rates of clinical failure. The low-risk group was defined as risk score of 0 to 3 points and the high-risk group was defined as a risk score ⩾4. The rates of clinical failure were 5.56% in the low-risk group and 19.77% in the high-risk group. In the validation stage, Kaplan–Meier curves differed significantly between the two groups. Patients in the high-risk group had a higher risk of clinical failure compared with the ones in the low-risk group (hazard ratio: 3.99; 95% CI: 2.31–6.91; p < 0.001). Nevertheless, preoperative use of the Zhongshan POEM score is limited by the need to include postoperative factors.
Urakami and colleagues aimed to overcome this limitation by developing and validating a novel scoring system consisting of only preoperative factors. A total of 244 patients undergoing POEM for esophageal motility disorders at a single center were retrospectively included in their study. 34 Poor responders were defined as patients with any of the following at 1-year follow-up: ES ⩾3, endoscopic findings of food retention, and retreatments (endoscopic balloon dilation, re-POEM, and surgical myotomy). All others were deemed good responders. After step-wise multivariate analysis, four independent risk predictors of poor response were identified: pretreatment ES (OR: 1.45; 95% CI: 1.16–1.80, p = 0.001), previous treatments (OR: 3.75; 95% CI: 1.63–8.63, p = 0.002), sigmoid-type esophagus (OR: 3.68; 95% CI: 1.67–8.11, p = 0.001), and esophageal dilation grade ⩾II (OR: 3.75; 95% CI: 1.55–9.09, p = 0.003). These risk factors were assigned points as follows: pretreatment ES (1-point increment), previous treatments (4 points), sigmoid-type esophagus (4 points), and esophageal dilation grade ⩾II (4 points). The risk score ranged from 0 to 24 points with 0–9 points suggesting low risk, 10–15 points intermediate risk, and ⩾16 points high risk. During internal validation the scoring system showed a satisfactory discriminatory performance and a good calibration. These scoring systems can be helpful in identifying the patient who will have a good response to POEM and permit the endoscopist to follow the high-risk patients closely postprocedure allowing earlier intervention and better individualized treatment.
Novel strategies
Despite the proven success of POEM as a treatment option for achalasia, endoscopists continue to explore strategies to stretch its durability and minimize adverse events such as GERD. The ideal length of myotomy remains a matter of debate. Predefined esophageal myotomy length and length guided by two penetrating vessels (TPVs) as anatomic landmarks have been proposed.
Nabi and colleagues 35 in an RCT compared short (3 cm) versus long (⩾6 cm) esophageal myotomy in patients with type I and II achalasia. Clinical success based on ES and improvement in integrated relaxation pressure and barium column height at 5 min were similar between the two treatment groups. Incidence of GERD was also comparable in both myotomy groups (44.44% versus 56.67%, p = 0.431). One benefit of the short myotomy group is the significantly shorter operative time (44.03 ± 13.78 min versus 72.43 ± 27.28 min, p < 0.001). These results are similar to those reported by Gu and colleagues 36 for the management of type II achalasia. No statistically significant difference in treatment success defined by an ES ⩽3 was observed between the two groups (93.8% in the standard myotomy versus 95.7% in the short myotomy, p = 0.520). However, the standard myotomy group had more postoperative esophageal acid reflux (43.8% versus 23.9%, p = 0.042). Again, the short myotomy group had a significantly shorter operative time compared with the standard myotomy cohort (31.2 ± 15.3 min versus 45.6 ± 16.2 min, p < 0.05). Overall, short myotomy has similar efficacy and risk as standard POEM with the benefit of requiring less operative time and possibly causing less acid reflux.
In attempts to reduce post-POEM reflux, a novel method was adopted to preserve the oblique muscles at the gastric cardia. This is achieved using TPVs as anatomic landmarks to guide the appropriate length of myotomy. This was reported to be feasible and reliable in 2018 when Tanaka and colleagues 37 performed POEM on 37 patients using the TPV landmarks with a mean gastric myotomy length of 3.0 cm. A follow-up study by Tanaka and colleagues showed that the TPV group had a much lower rate of grade B or higher reflux esophagitis (31.3% versus 58.1%, p = 0.017). Although GERD symptoms at 3 months were lower in the TPV group, this did not reach statistical significance (10.8% versus 19.4%, p = 0.23) when compared with the conventional line group. 38 The TPV method is an alternative way for the endoscopist to use a reliable landmark to the extent of the myotomy in hopes of minimizing subsequent GERD.
In a different strategy aiming at trying to reduce post-POEM GERD, endoscopists have been exploring the feasibility of performing acid-reducing procedures concurrently with POEM. Proposed therapies include POEM with fundoplication (POEM-F) or transoral incisionless fundoplication (POEM-TIF). There are limited data on these novel therapeutic approaches with small patient cohorts and short follow-up intervals. In a recent study by Patil and colleagues, 39 20 patients underwent POEM-F at a single center with an 85% technical success rate. These patients were followed for 3 months. At 1 month, follow-up endoscopy showed 29.4% of patients had loosening of the fundal wrap and 17.6% had ulcerations in the fundus and GEJ. At 3 months, 41.2% of patients had loosening of the wrap. The patients whose wrap was maintained had normal esophageal acid exposure. Thus, POEM-F is technically feasible, and the short-term outcomes are promising. Bapaye and colleagues 40 followed 25 patients for 1 year post POEM-F. POEM-F was technically successful in 92% of patients. At 12 months, GerdQ scores were <8 in 95.6% of patients signifying a low probability of GERD. A case report published in 2020 by Brewer Gutierrez and colleagues 41 described the first patient treated with single-session POEM-TIF. The procedure took a total of 139 min and an esophagram on postoperative day 1 showed no leak. At 6 months follow-up, the patient was asymptomatic without acid suppression therapy and underwent a 48-h pH study off PPI with 0.6% acid exposure and a DeMeester score of 2. High resolution esophageal manometry (HREM) showed partially treated achalasia type II. More research must be performed on technical feasibility, long-term outcomes prior to the widespread adoption of these techniques.
EndoFLIP/EsoFLIP balloon dilation
A subset of achalasia patients experience clinical failure posttreatment. EndoFLIP (Functional Luminal Imaging probe; Medtronic GI Solutions, Sunnyvale, California, USA) impedance planimetry system with its ability to evaluate bolus flow can be a complementary tool that helps in understanding the mechanical function of the esophagus and thus aids in diagnostic and management decisions especially in challenging cases (e.g. post failed treatment) (Figure 2).
EndoFLIP balloon placed across the lower esophageal sphincter.
While HREM measures the contractile topography of the esophagus, EndoFLIP focuses on the luminal geometry and the esophageal wall compliance as well as EGJ opening dynamics. 42 During volume-controlled balloon distention at a synchronized pressure and using high-resolution impedance, the diameter and cross-sectional area (CSA) of the esophagus and its stiffness can be evaluated in real time along the axial plane. The information obtained can help in calculating the distensibility index (DI) by dividing the median narrowest CSA by the median intra-bag pressure over a set time frame. 43 For accurate assessment of distensibility, the intra-bag pressure should be greater than 15 mm Hg to ensure adequate distension of the lumen. The aforementioned process is facilitated by a propriety software that filters out fluctuations caused by respiratory or vascular artifacts, peristalsis, and catheter movement.
In treatment-naïve patients with achalasia, the EGJ is narrow and stiff which is reflected by an abnormally reduced DI.44,45 This correlates with symptom severity calculated by the ES. 46 On the other hand, immediate increase in EGJ-DI is demonstrated following POEM, or Heller myotomy prior to creation of fundoplication, at which point DI tends to decrease.47,48 As such intraoperative real-time EndoFLIP can be utilized to plan the myotomy and to fashion the fundoplasty post myotomy balancing the extent of GEJ distensibility, while trying to limit GERD.
EndoFLIP may also predict clinical outcome after POEM. In a multicenter cohort study of 291 patients with achalasia undergoing POEM, Moran and colleagues 49 sought to evaluate if impedance planimetry measurements could predict clinical response and reflux following POEM. A total of 91.7% of patients had a clinical response (defined as ES ⩽3) after POEM and 39.4% developed reflux. Percent change in CSA (defined as postprocedural CSA divided by preprocedural CSA) and percent change in DI (defined as postprocedural DI divided by preprocedural DI) were the most predictive parameters at cutoff values of 360% and 272%, respectively. The impedance planimetry values were weak predictors of post-POEM reflux.
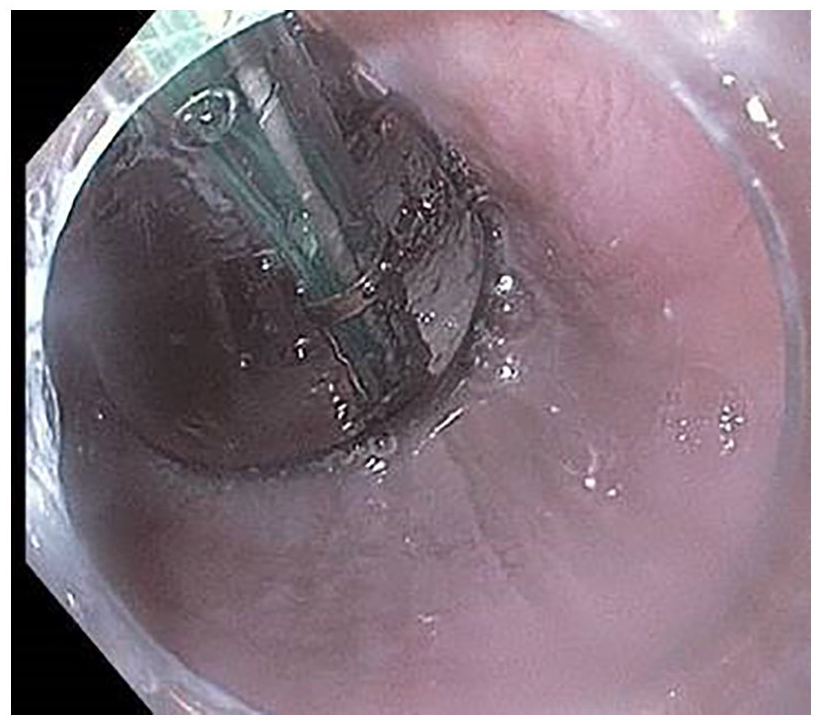
The EsoFLIP dilation balloons are derivatives of EndoFLIP but with rigid hydraulic balloons that lack the intra-bag pressure sensor. These ‘therapeutic’ balloons are used to perform EGJ dilation in patients with achalasia similar to that achieved with pneumo-dilation (Figure 3). Real-time display offers dynamic measurement of the aforementioned parameters while ensuring appropriate positioning of the balloon waist across the EGJ. This advantage allows for controlled dilation of the EGJ to a fixed diameter (up to 30 mm), obviating the need for fluoroscopy. In two recent studies, the EsoFLIP was shown to be successful (ES < 3) in 64–85% of patients at 6 months follow-up without major adverse effects.50,51 EsoFLIP eliminates the need for fluoroscopy and degree of dilation can be individualized (e.g. dilation stopped when the waist of the balloon is effaced).

EsoFLIP balloon placed across the lower esophageal sphincter for hydrostatic sphincter dilation in a patient with achalasia.
The use of the FLIP system provides an objective and convenient tool that aids in the diagnosis, treatment, and postoperative management as well as prediction of outcomes in patients with achalasia and achalasia variants. Furthermore, the EsoFLIP system is a safe treatment option for achalasia patients with the advantage of real-time individualized intervention similar to pneumo-dilation sans fluoroscopy. As such, the importance of the FLIP systems continues to evolve as we work on standardizing measurement protocols and establishing threshold values to corroborate their correlation with pre- and posttreatment dysphagia and reflux scores.
Guidelines
The American Society of Gastrointestinal Endoscopy (ASGE) published a new guideline in 2020 on the management of achalasia. 1 LHM, PD, and POEM are all appropriate and effective therapeutic modalities that should be considered for the treatment of achalasia. POEM is the recommended treatment for patients with type III achalasia. Botulinum toxin should not be used as a definitive therapy for achalasia, although it is appropriate for patients who are not candidates for other interventions. Patients who pursue POEM should be counseled about the increased risk of postprocedure reflux. In patients with failed initial myotomy of either method (LHM or POEM), the guidelines recommend PD or redo myotomy with the same or different technique.
The American College of Gastroenterology (ACG) also published updated guidelines in 2020 on diagnosis and management of achalasia. 2 These guidelines break down initial therapy based on achalasia subtype. For type I and type II achalasia, PD, LHM, and POEM have comparable efficacy. For type III achalasia, POEM is a more efficacious treatment option. Botulinum toxin should be utilized in patients who cannot undergo any of the other definitive therapies. Injection of botulinum toxin does not significantly alter the ability to perform a myotomy. In patients with failed initial therapies, ACG recommends that PD can be used for recurrent achalasia symptoms post LHM or POEM. In addition, POEM is a safe option for patients who have been treated with LHM or PD. If a patient fails endoscopic therapy (POEM or PD), LHM should be considered before definitive esophagectomy.
The European Society of Neurogastroenterology and Motility (ESNM) and United European Gastroenterology (UEG) published the European Guideline on Achalasia in 2020.52,53 These guidelines mirror those published by the ASGE and ACG in regard to safety and efficacy. Achalasia subtype, patient-specific characteristics, possible side effects, and the center’s expertise should factor in decision-making. Botulinum toxin should be reserved for patients who are unfit for more invasive treatment. One unique recommendation is to perform follow-up endoscopy to screen for GERD in patients treated with myotomy without an antireflux procedure. If there are reflux symptoms, PPI therapy is recommended.
The Japan Gastroenterological Endoscopy Society (JGES) published clinical practice guidelines for POEM in 2018. 54 The main recommendation is that POEM is indicated for the treatment of esophageal achalasia with good short-term outcomes. POEM treatment outcomes are similar to PD and LHM for type I and type II achalasia. POEM is better than the other treatment modalities for type III achalasia. POEM can be used for straight-type or sigmoid-type achalasia. It is appropriate to perform POEM after failed LHM. Outcomes of POEM are similar to LHM or balloon dilation. Finally, GERD should be assessed with an upper endoscopy and treated with acid secretion inhibitors as needed.
Finally, in 2019, the Korean Society of Neurogastroenterology and Motility (KSNM) and the Asian Neurogastroenterology and Motility Association (ANMA) created the Seoul Consensus on Esophageal Achalasia Guidelines which discussed the diagnosis and management of achalasia. 55 In contrast to the other guidelines, only pneumatic balloon dilation is recommended as the initial treatment for patients with achalasia. For type III achalasia, POEM is recommended over LHM despite comparable outcomes in treatment-naïve patients because it allows for extended myotomy. Acid suppressive therapy is recommended for patient with reflux symptoms or esophageal erosions undergoing POEM. Botulinum toxin is recommended for patients who are unfit for endoscopic or surgical treatment. For patients who fail initial therapy, POEM is recommended for patients who were initially treated with other endoscopic therapies or LHM.
Guidelines from different societies are summarized in Table 1.
Summary of relevant recommendations on achalasia from the different worldwide societies.

ACG, American College of Gastroenterology; ASGE, American Society of Gastrointestinal Endoscopy; ESNM, European Society of Neurogastroenterology and Motility; UEG, United European Gastroenterology; GERD, Gastroesophageal reflux disease; JGES, Japan Gastroenterological Endoscopy Society; LHM, laparoscopic Heller myotomy; PD, pneumatic dilation; POEM, peroral endoscopic myotomy; EGD, esophagogastroduodenoscopy. PPI, proton pump inhibitors.
Conclusion
Achalasia is a heterogeneous disease with no definite cure. Treatment options vary in efficacy and durability. The choice of intervention needs to be tailored to each individual patient based on several predefined variables (age, comorbid conditions, HREM, EndoFLIP, center’s expertise, etc.). To date, POEM has emerged as a successful alternative to PD or LHM. Despite research advancements, postmyotomy acid reflux remains an ongoing limitation. Proposed strategies to address reflux include short myotomy, TPV technique, the use of EndoFLIP during POEM, or with concomitant or subsequent anti-reflux procedures such as POEM-F or TIF. At this point, the utility of these techniques and long-term success remains to be well established. Nevertheless, the future of endoscopic therapy is bright.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.