
Abstract
Achalasia is a chronic incurable esophageal motility disorder characterized by impaired lower esophageal sphincter (LES) relaxation and loss of esophageal peristalsis. Although rare, it is currently the most common primary esophageal motility disorder, with an annual incidence of around 1.6 per 100,000 persons and prevalence of around 10.8/100,000 persons. Symptoms of achalasia include dysphagia to both solids and liquids, regurgitation, aspiration, chest pain and weight loss. As the underlying etiology of achalasia remains unclear, there is currently no curative treatment for achalasia. Management of achalasia mainly involves improving the esophageal outflow in order to provide symptomatic relief to patients. The most effective treatment options for achalasia include pneumatic dilation, Heller myotomy and peroral endoscopic myotomy (POEM), with the latter increasingly emerging as the treatment of choice for many patients. This review focusses on evidence for current and emerging treatment options for achalasia with a particular emphasis on POEM.
Introduction
Achalasia, first described by Sir Thomas Willis in 1674, is a chronic disorder of esophageal motility characterized by impaired lower esophageal sphincter (LES) relaxation and loss of esophageal peristalsis.1,2 Although rare, it is currently the most common primary esophageal motility disorder, with an annual incidence of around 1.6 per 100,000 people and prevalence of around 10.8 per 100,000 people. 3 Symptoms of achalasia include dysphagia to both solids and liquids, regurgitation, aspiration, chest pain and weight loss. 4
Achalasia is an idiopathic condition that affects both men and women of all ages. The pathophysiological changes of achalasia involve a selective loss of inhibitory neurons of the myenteric plexus that coordinate esophageal peristalsis and facilitate LES relaxation in response to a food bolus.1,2 The underlying etiological cause for these changes is unknown, although autoimmune, viral and neurodegenerative triggers have been proposed. 5
A number of diagnostic tests are routinely utilized for the diagnosis of achalasia. An upper endoscopy generally shows a dilated esophagus with a spastic LES. It usually shows retained food and saliva and also helps exclude other anatomical esophageal abnormalities or tumors which can mimic symptoms of achalasia. Barium esophagram classically shows the presence of a dilated esophagus, impaired esophageal motility and clearing, and a narrowed gastroesophageal junction (GEJ) resulting in a ‘bird’s beak’ sign. High-resolution esophageal manometry (HREM) confirms the diagnosis of achalasia by demonstrating lack of esophageal motility and impaired relaxation of LES. Based on the HREM findings, achalasia is classified into three types, as outlined in the Chicago classification: type I, type II, and type III. 6 Along with impaired relaxation of LES, type I achalasia is characterized by a complete absence of esophageal peristalsis on HREM, type II is characterized by pan-esophageal pressurization, and type III is characterized by spastic contractions in the esophagus. In addition to the differences in HREM findings, these subtypes portend somewhat different prognosis and treatment outcomes.7–9
As the underlying etiology of achalasia remains unclear, there is currently no curative treatment for achalasia. 5 All available treatments are hence palliative. Management of achalasia involves improving the esophageal outflow in order to provide symptomatic relief to patients. Traditionally, the treatment modalities employed for this purpose included pharmacological therapy (e.g. calcium channel blockers, long-acting nitrates), endoscopic interventions (e.g. endoscopic botulinum toxin injection to LES, pneumatic dilation), and possibly surgical interventions (surgical myotomy, esophagectomy). 10 In recent years, peroral endoscopic myotomy (POEM) has emerged as an alternative approach for treatment of achalasia and is increasingly being utilized, especially in patients with multiple comorbidities who are poor candidates for traditional laparoscopic or open surgical interventions.
Because treatment of achalasia is not curative, therapeutic success is determined by the improvement in symptoms as reported by patients. To this effect, a simple scoring system has been developed to quantify severity of symptoms before and after treatment. Frequently referred to as the Eckardt score, the scoring system takes into account the frequency of each of the four major symptoms of achalasia including dysphagia, regurgitation, retrosternal pain and weight loss. Each symptom is scored on a 0–3 scale, resulting in total possible scores between 0 and 12, with higher scores indicating more symptomatic disease (Table 1). 11 Although the exact definition of treatment success differs in each study, a decrease in Eckardt score to 3 or less is generally considered a success.
Clinical scoring system for achalasia (Eckardt score).

This review focusses on evidence for current and emerging treatment options for achalasia with a particular emphasis on POEM (Table 2).
Therapeutic options for treatment of achalasia.
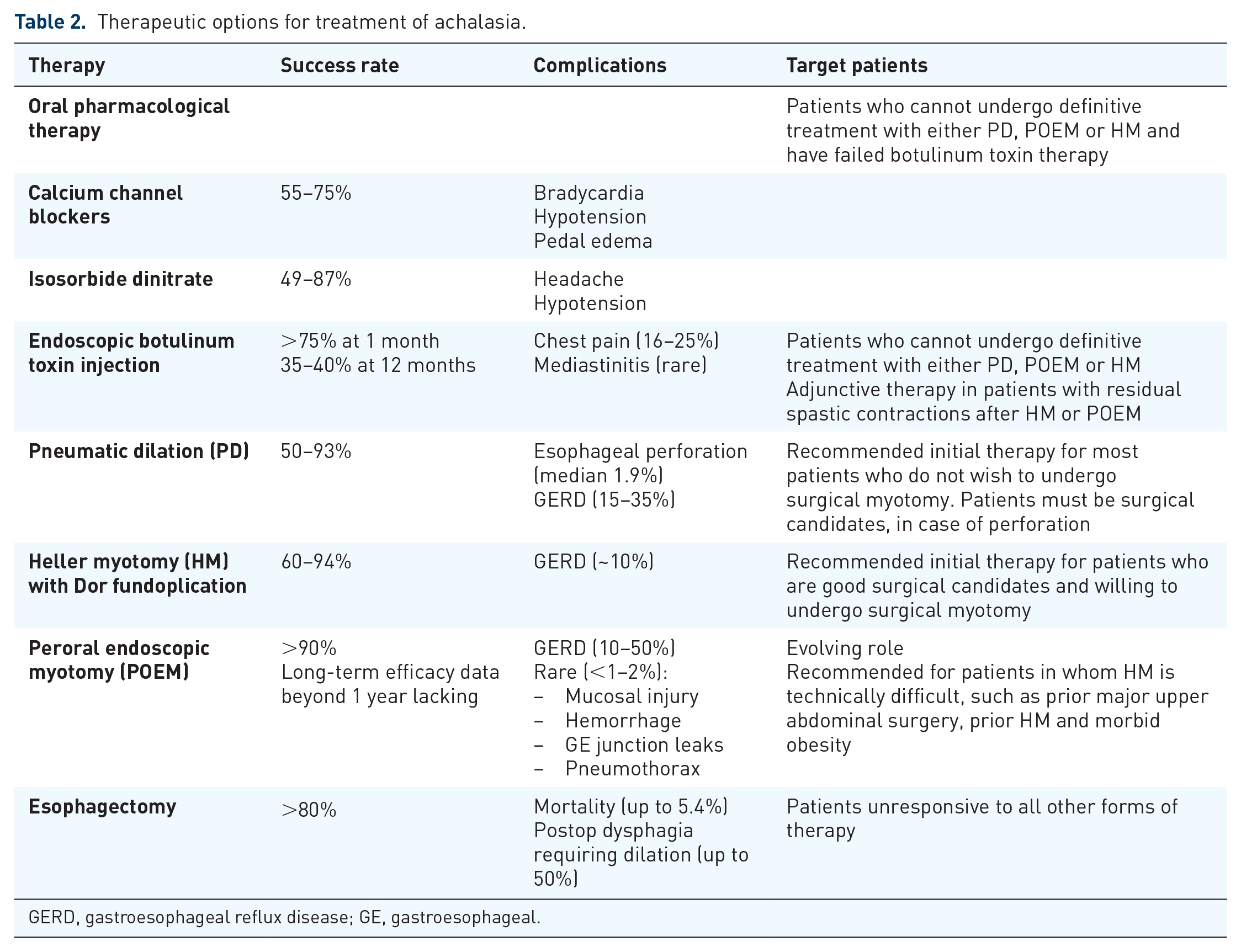
GERD, gastroesophageal reflux disease; GE, gastroesophageal.
Oral pharmacological therapy
Several oral pharmacological agents have been employed in the management of achalasia. These include calcium channel blockers (e.g. nifedipine), long-acting nitrates (e.g. isosorbide dinitrate), phosphodiesterase-5-inhibitors (e.g. sildenafil), anticholinergics (e.g. atropine, dicyclomine), and beta-adrenergic agonists (e.g. terbutaline), with calcium channel blockers and long-acting nitrates being the most commonly used. 10 These agents work by facilitating esophageal emptying by decreasing smooth muscle tone and causing smooth muscle relaxation of the LES. Oral agents, however, are among the least effective treatment options, with only transient benefit and significant potential for side effects due to their mechanisms of action. 12 As a result, oral pharmacological therapy is generally only reserved for those patients who are not candidates for other therapies as detailed below.
If oral pharmacological agents are employed, current guidelines recommend the use of nifedipine 10–30 mg, sublingually 30–45 min before meals or isosorbide dinitrate 5 mg, 10–15 min before meals for best response. 10
Endoscopic botulinum toxin injection
Injection of botulinum toxin into the LES via upper endoscopy has been shown to be a useful treatment option for achalasia. By causing presynaptic inhibition of acetylcholine release, botulinum toxin blocks the unopposed excitatory cholinergic stimulus to the LES, which is characteristic of achalasia. This leads to paralysis of the LES muscle due to neuronal inhibition but has no effect on the resting muscle tone, which is mostly driven by myogenic influence. 10 Thus, the overall effect of botulinum toxin injection is an approximate 50% reduction in LES pressure. 13 This reduction is sufficient to permit esophageal emptying and it provides symptomatic relief in nearly two thirds of patients. 13
The standard technique for botulinum toxin therapy involves the use of 100 units of toxin diluted in normal saline and injected in four quadrants just above the squamocolumnar junction using an injection needle via standard upper endoscope. This technique is user friendly with low risk of serious complications. 10
The initial response rate of as high as 82% has been reported at 1 month and the effect can last several months.10,13,14 However, most patients require repeated injection every 6–24 months because the effect wears off.14–16
There is some evidence to suggest that endoscopic botulinum toxin therapy may make subsequent surgical myotomy or POEM, if needed, more difficult due to obliteration of the sub-mucosal plane secondary to inflammation from repeated injections.17–19 This may lead to worse outcomes, including more intrasurgical and postsurgical complications and higher failure rates. 19
According to current guidelines, endoscopic botulinum toxin injection is reserved for patients who are not candidates for pneumatic dilation or surgical myotomy. 10 In addition, it can be used as an adjunct in patients with residual spastic contractions after myotomy. 10
Pneumatic dilation
Pneumatic dilation utilizes graded, sized polyethylene balloons which are intraluminally dilated, leading to disruption of the LES circular muscle fibers due to air pressure. Pneumatic dilation balloons come in diameters of 3.0, 3.5 and 4.0 cm and are much larger than the standard through-the-scope balloons that have a maximum diameter of 2.0 cm. As a result, the pressure generated by pneumatic dilation balloons is significantly more than standard through-the-scope balloons or bougie dilators, which are not effective in fracturing the muscularis propria of the LES. Pneumatic dilation is currently the most effective nonsurgical option for treatment of achalasia.10,20
Pneumatic dilation is generally performed under sedation with fluoroscopic guidance to accurately position the balloon across the LES. The balloon is distended to a pressure of 8–15 psi and held for 15–60 s while confirming the effacement of balloon waist on fluoroscopy. Current guidelines recommend obtaining gastrograffin study followed by barium esophagram in all patients after pneumatic dilation to exclude esophageal perforation.10,21,22
Initial dilation for most patients is performed using a 3.0 cm balloon with subsequent symptomatic and objective evaluation after 4–6 weeks. For patients who continue to remain symptomatic, dilation with next-sized dilator can be employed. This serial pneumatic dilation approach has been shown to have excellent success rates, with some series reporting good-to-excellent relief of symptoms in up to 93% of patients.12,23,24 Additionally, the risk of perforation may be lower with the serial pneumatic dilation approach. 10 However, the serial pneumatic dilation approach may be less effective among younger males <45 years of age who have thicker LES muscle. In this group of patients, current guidelines recommend the use of a 3.5 cm balloon or surgical myotomy as the initial therapeutic intervention. 10 Pneumatic dilation carries a significant inherent risk of esophageal perforation, with a reported median rate of 1.9% in the hands of expert operators.24,25 For this reason, surgical backup must be available and patients undergoing pneumatic dilation must also be candidates for surgical repair, in case of esophageal perforation. Patients undergoing pneumatic dilation must be made aware and counseled regarding this risk and understand that surgical repair may be necessary. Other complications of pneumatic dilation include the occurrence of gastroesophageal reflux disease (GERD) after pneumatic dilation in 15–35% of patients. 10 This should be treated with proton pump inhibitor therapy to prevent the formation of peptic strictures. Prolonged postdilation chest pain, intramural hematoma and traumatic diverticuli have also been described after pneumatic dilation. 25
Surgical Heller myotomy
Surgical myotomy for the treatment of achalasia involves the surgical division of the circular muscle fibers of the LES and was first described by Ernst Heller in 1913. 26 Although originally described through a thoracotomy, the technique has evolved over the years, initially through a thoracoscopic approach and finally via laparoscopic approach, which is currently the method of choice.27,28 This is because of reduced rates of postoperative morbidity, including pain, shorter hospitalization, better resolution of dysphagia, and less postoperative heartburn as compared with other approaches. 29
Results from a European randomized controlled trial comparing the efficacy of pneumatic dilation versus laparoscopic Heller myotomy (LHM) showed no significant difference in the efficacy of the two modalities after 2 years of follow up. 30 The rate of success at 2 years, as defined by an improvement in Eckardt Score to ⩽3 was noted to be 86% with pneumatic dilation, and 90% with LHM, with no statistically significant difference between the two treatment strategies (p = 0.46). Additionally, there were no significant differences in postprocedural LES pressure, height of barium-contrast column, or quality of life between the two groups. A follow-up study with long-term data from the trial showed similar efficacy, even at 5 years. 31 However, 25% of patients treated with pneumatic dilation required redilation.
These results, however, differ somewhat from the results of meta-analyses. A meta-analysis of 105 articles reporting on 7855 patients that compared the efficacy of various endoscopic and surgical options in the treatment of achalasia found that LHM provided better symptom relief than other endoscopic or surgical approaches. 23 Symptomatic improvement was noted in nearly 90% of patients after laparoscopic myotomy, compared with 85% of patients treated with open transabdominal approach, 83% with open transthoracic approach, and 77.6% with thoracoscopic myotomy. However, a drawback of the meta-analysis was that included studies were heterogeneous in terms of length of follow up and definition of treatment success. Additionally, the included studies consisted of cohort or case-control study designs and lacked any randomized controlled trials. A subsequent meta-analysis of randomized controlled trials comparing pneumatic dilation versus LHM in 346 patients showed significantly higher cumulative response rate with LHM (86%) than with pneumatic dilation [76%; odds ratio (OR) 1.98, p = 0.02]. Additionally, rates of major adverse events requiring subsequent intervention were significantly lower with LHM (0.6%) than with pneumatic dilation (4.8%; p = 0.04). 32
The discordance between results from randomized controlled trials and meta-analyses may be explained by the fact that rate of treatment response differs among the different subtypes of achalasia. A cohort study of 45 achalasia patients who underwent pneumatic dilation demonstrated higher response rate in patients with type II achalasia (90%) than in type I achalasia (63.3%) or type III achalasia (33.3%). 8 Additionally, analysis of data from the European achalasia trial further revealed that success rates in patients with type II achalasia was significantly higher for pneumatic dilation (100%) than for LHM (93%; p < 0.05). However, in patients with type III achalasia, LHM had a higher success rate (86%) than pneumatic dilation (40%; p = 0.12). For type I achalasia, LHM and pneumatic dilation had similar success rates (81% versus 85%, respectively; p = 0.84). 33
Although effective, one major complication of surgical myotomy is the development of postoperative GERD in nearly one third of patients. 23 As a result, Heller myotomy is frequently combined with a partial fundoplication to prevent acid reflux, based on recommendations from current surgical guidelines. 34 Although there is concern and debate regarding the possibility of increased postoperative dysphagia with the performance of fundoplication, the rates of dysphagia were found to be similar in patients with or without fundoplication. 23 Additionally, the rate of postoperative GERD after Heller myotomy was noted to decrease to around 10% with the addition of a partial fundoplication. 23 Furthermore, addition of partial fundoplication was also found to be more cost effective than myotomy alone because of cost savings from the long-term treatment of GERD. 35
Esophagectomy
Patients unresponsive to other forms of therapy may require esophagectomy for relief of symptoms. However, given its significant morbidity and mortality, esophagectomy is generally reserved for patients with end-stage achalasia who are good surgical candidates and who have failed pneumatic dilation with or without Heller myotomy in the past. Although symptomatic improvement is reported in over 80% of patients undergoing esophagectomy, complications include postoperative dysphagia requiring dilation in up to 50% of patients, and a mortality risk of up to 5.4%.10,36
Peroral endoscopic myotomy
POEM is a hybrid endoscopic–surgical procedure utilizing the concept of natural orifice transluminal endoscopic surgery to perform endoscopic myotomy. The technique was developed in Japan with the first POEM performed in 2008. 37 Initially described as an investigational procedure, it is now fast being recognized as one of the standard treatments for achalasia, with some experts even utilizing it as a first-line therapy, given its excellent efficacy and safety profile. 38 Even though thousands of cases of POEM have been reported worldwide since its initial description, the availability of POEM remains limited to highly specialized centers in the United States.
Even though there are minor variations in the POEM technique practiced at different centers, one of the most widely accepted techniques, as practiced by Inoue et al., the original developers of POEM, was recently described in detail. 39 According to the authors, the technique has been used to safely perform POEM in patients as young as 3 years old and without any upper age limit. 40 However, POEM is contraindicated in patients who are unable to tolerate general anesthesia, or who have coagulopathy, portal hypertension, or prior radiation, ablation, or mucosal resection in the planned operative field, due to an increased risk of perforation or hemorrhage. 41
In brief, the POEM procedure involves the use of a high-definition upper endoscope with a clear cap attached at the tip. Using carbon dioxide insufflation and a specialized needle knife, a longitudinal mucosal incision is made in the lower esophagus proximal to the GEJ. The submucosal space is then entered and a tunnel created along the length of the esophagus to a point along the lesser curvature of the stomach around 2–3 cm distal to the GEJ. Myotomy of the circular muscle fibers is then performed and the mucosotomy finally closed with linear and symmetric deployment of hemoclips.
Given the recent advent and novelty of the procedure, the learning curve for POEM has been an area of interest and investigation. In an initial prospective series from Portland (OR, USA), it was observed that the procedure length per centimeter of myotomy and incidence of mucosal perforation plateaued after approximately 20 cases, which was estimated to be the number of cases required by an experienced endoscopist to reach competency. 42 Another similar single-center study from China with two operators reported a plateau in learning after around 25 cases. 43 In a recent study from New York (NY, USA), Patel et al. reported relative mastery in POEM after approximately 60 cases. 44
POEM is especially useful for patients in whom laparoscopic myotomy is technically difficult, such as prior major upper abdominal surgery, prior Heller myotomy and morbid obesity. There have been several studies comparing the efficacy of POEM to other achalasia treatment modalities. In our reported experience, utilizing a two-person technique, we found equivalent efficacy of POEM, pneumatic dilation and Heller myotomy at 2 months. 45 Similar results have been reported in multiple meta-analyses that have found equivalent efficacy and safety for POEM and Heller myotomy.46,47 However, results are limited due to lack of randomized controlled trials, as well as lack of efficacy data beyond 1 year. In general, the efficacy of POEM has been reported as >90%. 48 Additionally, the length of hospital stay after POEM has been shown as significantly lower than HM. 46
POEM has also been found to be remarkably safe and well tolerated. Serious adverse events are rare but can include inadvertent mucosotomies, leaks near the GEJ requiring urgent surgical intervention, intraprocedural pneumothorax or pneumoperitoneum, intrasurgical or postprocedural tunnel or luminal bleeding. 48 The incidence of these most serious adverse events, however, is <1–2%. Similar to Heller myotomy, postoperative GERD has been observed after POEM. The reported rate of GERD after POEM has varied somewhat in literature between 10% and 50%. However, more recent data suggest similar rates of GERD after POEM and Heller myotomy with Dor fundoplication.48–50 Long-term studies comparing the efficacy of POEM with Heller myotomy and pneumatic dilation are needed.
Other therapies
Ethanolamine oleate is a sclerosing agent that can induce inflammatory response and fibrosis, thus causing excitatory neuron damage and decreasing the LES pressure. 51 A few case series have shown good initial symptom response after intrasphincteric injections with ethanolamine oleate comparable with botulinum toxin injection. 52 Another novel technique is the use of a specially designed temporary metal stent available in 20, 25 and 30 mm diameters. 53 The stent is left in place for 4–5 days and then retrieved. Use of a 30 mm stent was associated with 87% clinical remission rate on >7 years of follow up. Although these results appear to be promising, more confirmatory studies are needed before implementing into regular clinical practice.
Conclusion
Achalasia is a chronic incurable primary esophageal motility disorder causing symptoms of dysphagia, regurgitation, chest pain and weight loss. Treatment for achalasia is mainly focused on improving esophageal emptying in order to provide symptomatic relief to patients. Therapeutic options include a variety of medical, endoscopic and surgical techniques and the choice of treatment depends on appropriate patient selection.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.