
Abstract
Peroral endoscopic myotomy (POEM) has been shown to be an effective treatment for achalasia and with few adverse events. Only a few cases of delayed bleeding have been described. This current case report describes a patient with delayed bleeding in the submucosal tunnel on the eighth day after POEM. The patient was a 21-year-old woman with a 4-month history of dysphagia, vomiting and excessive weight loss. Achalasia was diagnosed according to her symptoms, barium oesophagogram, oesophageal manometry and endoscopy examination. POEM was performed by an experienced operator. On the eighth day after POEM, the patient suddenly developed continuous haematemesis presented with vomiting of fresh blood and melena. An emergency exploratory esophagogastroduodenoscopy was performed. A large number of blood clots were found at the wound and a long haematoma was found along the lining of the submucosal tunnel. Re-entry into the submucosal tunnel and exposure of the haemorrhagic site was attempted but failed because of severe submucosal tissue adhesion. An emergency angiography was undertaken and haemostasis was achieved with superselective arterial microcoil embolization.
Introduction
Achalasia is a rare cause of dysphagia resulting from failed lower oesophageal sphincter relaxation and oesophageal dysmotility. Peroral endoscopic myotomy (POEM) has been shown to be an effective treatment for achalasia and with few adverse events.1,2 Common complications of POEM include inadvertent mucosotomy, pneumoperitoneum, oesophageal leak, pneumonia, bleeding, pneumothorax and reflux oesophagitis. 3 Only a few cases of delayed bleeding have been described.4–6 Most of the delayed bleeding occurred during the first day to the third day after the POEM procedure. 7 This current case report describes a patient with delayed bleeding in the submucosal tunnel on the eighth day after POEM.
Case report
In December 2014, a 21-year-old woman with a 4-month history of dysphagia, vomiting and excessive weight loss presented to the Department of Gastroenterology, The Second Hospital of Hebei Medical University, Hebei Key Laboratory of Gastroenterology, Hebei Institute of Gastroenterology, Hebei Clinical Research Centre for Digestive Diseases, Shijiazhuang, Hebei Province, China. Achalasia was suspected because of the symptoms that she presented with. This was confirmed by barium oesophagogram, oesophageal manometry and endoscopy (Figure 1). There were no predisposing factors to bleeding, such as coagulation disorders and antiplatelet/anticoagulant therapy.

The diagnostic evidence in a 21-year-old woman that presented with a 4-month history of dysphagia, vomiting and excessive weight loss suggested achalasia: (a) barium oesophagogram; (b) oesophageal manometry; (c) oesophageal endoscopy and (d) oesophageal endoscopy. The colour version of this figure is available at: http://imr.sagepub.com.
Peroral endoscopic myotomy was performed by an experienced operator (L.L.). The initial incision was made on the left oesophageal wall after submucosal injection. Circular muscle myotomy was undertaken from approximately 7 cm above the gastroesophageal junction (GEJ) and extended for a distance of 2 cm toward the stomach. Coagulation with haemostatic forceps was performed when bleeding occurred. No major bleeding occurred during the procedure. At last, the entry was closed using haemostatic clips (Figure 2). She was given a full liquid diet from the third postoperative day. On the eighth day after POEM, the patient suddenly developed continuous haematemesis presented with vomiting of fresh blood and melena. Her haemoglobin level fell from 8.5 g/dl to 6.0 g/dl, with the lowest blood pressure of 96/76 mmHg. So delayed bleeding was considered. Proton pump inhibitors (omeprazole, 8 mg/h, intravenous pumping), antibiotics (ceftriaxone sodium, 3.0 g, once a day, intravenous transfusion), haemocoagulase (lyophilized thrombin powder, 1000 U, every 6 h, oral administration) and blood transfusions were administered to the patient for 5 days. Chest computed tomography imaging showed a haematoma in the oesophagus. An emergency exploratory oesophagogastroduodenoscopy was performed. A large number of blood clots were found at the wound. After the blood clots were removed, a long haematoma was found along the lining of the submucosal tunnel and there was no ulcer or tunnel-entry dehiscence found (Figure 3). Re-entry into the submucosal tunnel and exposure of the haemorrhagic site was attempted, but this failed because of severe submucosal tissue adhesion. An emergency angiography was undertaken. Written informed consent was provided by the patient before the operation. A point of contrast medium extravasation from a branch of the left gastric artery was identified. Haemostasis was achieved with superselective arterial microcoil embolization (Tornado® Embolization Coil; COOK MEDICAL LLC, Bloomington, IN, USA) (Figure 4). Satisfactory healing was seen at the 9-month follow-up endoscopy. The Eckardt scores had decreased between pretreatment and posttreatment from 7 to 1, respectively, by the 9 month follow-up. The patient provided written informed consent for their treatment. Ethical approval was not required because the manuscript was a case report. The patient provided consent for use of her data to be used for scientific research. The reporting of this study conforms to CARE guidelines. 8

The peroral endoscopic myotomy procedure in a 21-year-old woman that presented with a 4-month history of dysphagia, vomiting and excessive weight loss diagnosed with achalasia: (a) the initial incision was made on the left oesophageal wall after submucosal injection; (b) circular muscle myotomy was undertaken from approximately 7 cm above the gastroesophageal junction and extended for a distance of 2 cm toward the stomach; (c and d) coagulation with haemostatic forceps was performed when bleeding occurred; (e) no major bleeding occurred during the procedure and (f) the entry was closed using haemostatic clips. The colour version of this figure is available at: http://imr.sagepub.com.
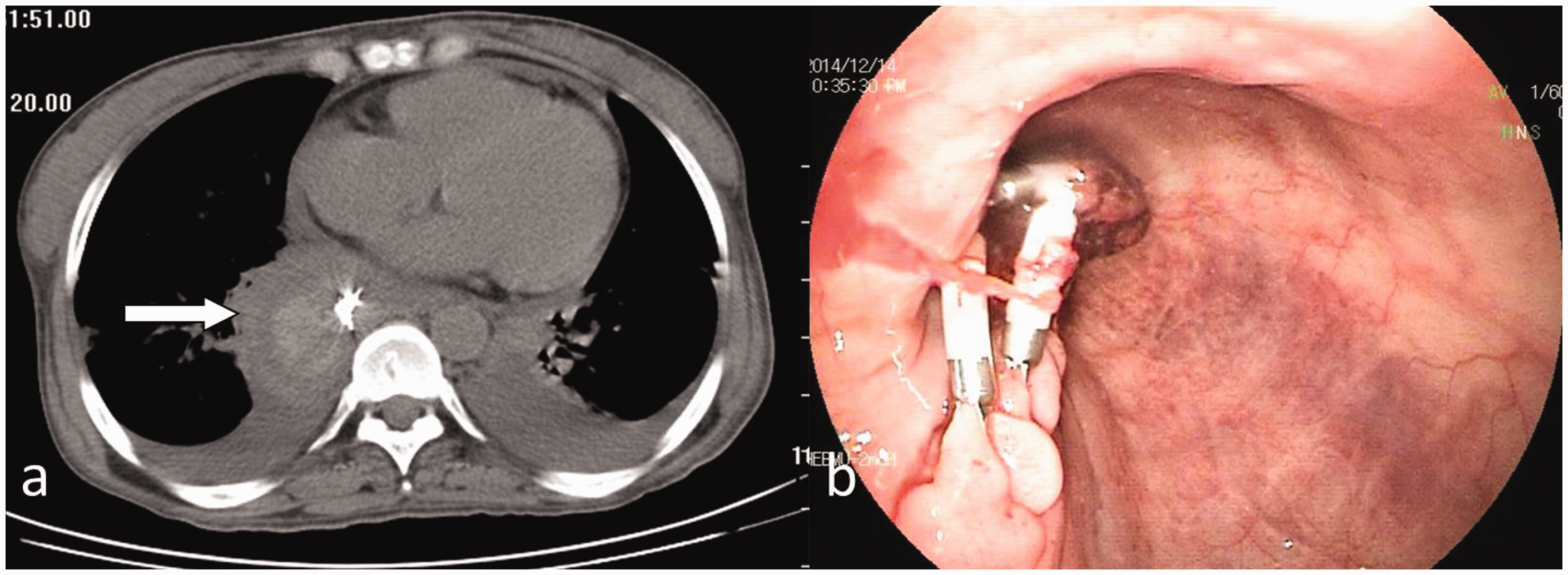
Delayed bleeding was evident on a chest computed tomography scan (a) and gastroscopic image and (b) in a 21-year-old woman diagnosed with achalasia that underwent peroral endoscopic myotomy. The colour version of this figure is available at: http://imr.sagepub.com.

Angiographic images of a 21-year-old woman that experienced delayed bleeding after peroral endoscopic myotomy showing a point of contrast medium extravasation (arrow) from a branch of the left gastric artery (a) and the successful use of superselective arterial microcoil embolization (arrow) to achieve haemostasis (b).
Discussion
Peroral endoscopic myotomy usually has few complications, but when these happen they may be very severe and possibly life-threatening.3 Delayed bleeding is one of the serious complications. The incidence of delayed bleeding was noted to be 1.1% in a meta-analysis of 1122 patients undergoing POEM. 9 Most of the cases of delayed bleeding were due to haematoma in the submucosal tunnel, and a few were caused by ulcers in the oesophagus or cardia. 9 In the submucosal tunnel, bleeding usually occurs at the cut muscular edges and locates at the GEJ or distal on the stomach side due to increased vascularity.6,10 The treatments include conservative treatment, Sengstaken–Blakemore tube or self-expanding metal stents (SEMS) compression, endoscopic vessel coagulation and surgical intervention.4,11 For this current patient, conservative treatment and emergency endoscopy both failed to result in haemostasis. Sengstaken–Blakemore tube or SEMS placement as a treatment for delayed bleeding has been reported. 6,11 But delayed bleeding leading to mediastinal haematoma has been reported even though there was no Sengstaken–Blakemore tube compression. 12 As the conservative treatment did not work in this current patient they were then treated with angiographic embolization. This technique as a haemostasis treatment for uncontrolled bleeding of endoscopic retrograde cholangiopancreatography or endoscopic submucosal dissection (ESD) has been reported for several years.13,14 To the best of our knowledge, this is the first case of delayed post-POEM bleeding treated with superselective arterial microcoil embolization. The culprit vessel was a branch of the left gastric artery. Based on the experience with this current case, angiographic embolization may also be an effective diagnostic and therapeutic alternative for delayed bleeding after POEM.
In conclusion, it is difficult to predict and prevent delayed bleeding after the POEM procedure. The incidence of delayed bleeding may be decreased because of more precise visual control and using established ESD haemostasis techniques. Careful intraoperative haemocoagulation may prevent delayed bleeding.6,15 Angiographic embolization could be another option for achieving haemostasis for delayed bleeding after POEM.
Research Data
Research Data for Superselective arterial microcoil embolization for delayed bleeding after peroral endoscopic myotomy
Research Data for Superselective arterial microcoil embolization for delayed bleeding after peroral endoscopic myotomy by Xuechen Liu, Yonghong Zhou, Xiaoyu Jiang, Li Liu, Dongqiang Zhao, Huihui Ma, Hui Tian and Huiqing Jiang in Journal of International Medical Research
Footnotes
Author contributions
Xuechen Liu and Li Liu were mainly responsible for the diagnosis and treatment of the patient. Xuechen Liu, Yonghong Zhou and Xiaoyu Jiang drafted the manuscript. Xuechen Liu was in charge of revising the manuscript and submitting the revisions. Huihui Ma and Hui Tian assisted with the therapeutic procedures. Li Liu, Dongqiang Zhao and Huiqing Jiang took part in the multidisciplinary treatment of the patient and put forward some suggestions for references.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt (pending publication) of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hebei Provincial Department of Science and Technology (project number: 182777117D).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.