
Abstract
Background
Cerebral Venous Thrombosis (CVT), accounting for 3% of strokes, can be assessed using non-invasive Transcranial Doppler (TCD) ultrasound to measure cerebrovascular function in real-time. The TCD-derived pulsatility index (PI), highly correlates with intracranial pressure (ICP) and serves as a reliable non-invasive monitoring tool.
Aim
This study aims to correlate PI by TCD with clinical outcomes in CVT patients.
Methods
A prospective observational study of 41 CVT patients admitted between June 2022 to December 2022 was conducted in the Department of Neurology of MBS Hospital. Each patient was subjected to TCD and the PI was also recorded. The results were analysed with SPSS.
Results
Out of the 41 patients, two patients died and 39 patients were discharged. The PI at admission in the left middle cerebral artery (MCA) was 1.19 ± 0.20 amongst discharged and 1.64 ± 0.10 amongst those who died (p = .003). Similarly, the PI at admission in the right MCA was 1.23 ± 0.21 amongst those discharged and 1.63 ± 0.20 amongst those who died (p = .02). Also, PI in both left and right MCA positively and significantly correlated with CVT GS score at admission (r = 0.70, p < .05; r = 0.64, p < .05).
Conclusion
PI at admission is both right and left MCA was found to be significantly higher in patients who died during the hospital stay. Also, PI significantly correlated with the CVT GS score at the presentation. Thus, PI at admission by TCD can predict the clinical outcome of patients with CVT.
Keywords
Introduction
Cerebral venous thrombosis (CVT) constitutes less than 5% of all strokes, and its recognition has been on the rise due to the increasing utilisation of Magnetic Resonance Imaging (MRI) and growing clinical awareness. 1 Given its diverse aetiology and symptomatology, CVT is a condition that demands attention not only from neurologists and neurosurgeons but also from internists and emergency clinicians. The annual incidence varies between 1.16 and 2.02 cases per 100,000 individuals and is more prevalent among females compared to males, 2 with a ratio of 3:1 and an overall 30-day mortality of around 3% and 1-year mortality of 6%. 3 According to the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT), the typical age of individuals with CVT was 37 years, 4 and just 8% of the patients were above 65 years old. 5 Among the genders, females had a substantially lower median age (34 years) in comparison to males (42 years). 3
Transcranial Doppler (TCD) ultrasound is a fast, non-invasive method for measuring cerebrovascular function in real time. The TCD technique can measure flow velocity in the brain’s arterial system to identify changes in flow, diagnose vascular stenosis, or detect embolic signals in these arteries. It is a valuable tool in the clinical diagnosis of various cerebrovascular disorders such as acute ischemic stroke, traumatic brain injury, subarachnoid haemorrhage, idiopathic intracranial hypertension, and other conditions such as brain death. 6 Increasingly, TCD has now proven to be a useful non-invasive technique for monitoring intracranial pressure (ICP) in CVT patients and has demonstrated a strong correlation with clinical outcomes and changes in ophthalmological parameters. 7
The TCD-derived pulsatility index (PI) has been shown to be highly correlated with ICP and is recommended as a dependable non-invasive monitoring tool. 8 PI is a dimensionless index that is not affected by the angle of insonation, making it an easy test to perform with acceptable reliability even for less-experienced paramedics. 7 The current research aims to study the correlation of PI by TCD in the clinical outcome of CVT patients.
Materials and Methods
A prospective observational study was conducted in the Department of Neurology of MBS Hospital, Kota. The diagnosis of CVT was confirmed by clinical examination and imaging (CT Venogram/MR Venogram brain). The grade of cerebral edema was also recorded based on NCCT/MRI brain. TCD was performed using a Delica EMS-9D portable machine for assessment of the PI. Patients of both genders above the age of 18 years presenting with CVT in the neurology department of MBS Hospital between June 2022 and December 2022 were included in the study. The study excluded patients who were already receiving anticoagulant therapy for indications other than CVT and those who had undergone neurosurgical intervention. Individuals with a previous history of cerebrovascular accident (CVA) or recurrent CVT were also excluded from the analysis. The final sample size comprised a total of 41 patients. Written informed consent was obtained from all the study participants prior to their inclusion in the study. Also, the study received approval from the ethical committee of the institution.
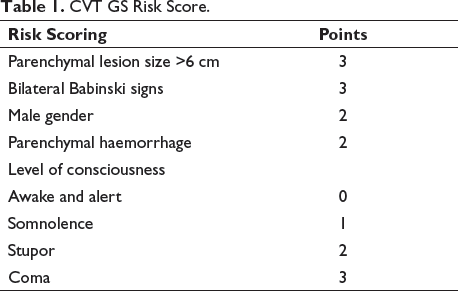
Every patient underwent TCD evaluation at admission (day 1) and on day 3 of admission. Using a 1.6/2 MHz probe, TCD recordings were taken by insonating both sides of the middle cerebral artery (MCA) through a temporal acoustic window at a depth of 40–65 mm and the PI was recorded during each session. Each patient was assessed using the CVT GS score, which ranges between 0 and 13 (Table 1). Based on the result, they were categorised into the mild (≤2 points), moderate (3–7 points) and severe (≥8) categories. Statistical tool SPSS version 22 was used to analyse the data collected during the study.
CVT GS Risk Score.
Results
The study included a cohort of 41 patients diagnosed with CVT, with a median age of 29 years. The majority of participants were female, that is, 25 (61%). The most prevalent risk factors observed in CVT patients were vitamin B12 deficiency (51.22%) and hyperhomocysteinemia (46.34%). Tobacco use emerged as the most common addiction among CVT patients, with a prevalence of 26.83%. Notably, among female patients, OCP use was identified as a significant risk factor (32%). Headache (97.56%) was the most frequently reported symptom, followed by nausea (85.37%) and vomiting (70.73%). Papilledema was present in 95.12% of the CVT patients. The right transverse sinus was the most commonly involved site, followed by the superior sagittal sinus. Each patient was assigned a CVT GS score, with approximately half falling into the mild category. The overall outcome showed that 95% of patients were discharged, while 5% died during hospitalisation (Table 2).
Clinical Characteristics of Study Population.

A statistical analysis was conducted to examine how the severity of CVT as assessed by CVT GS score at admission relates to the duration of hospital stay. The results revealed a significant difference in the mean CVT GS score between patients with hospital stays of seven days or less and those with stays exceeding seven days (1.22 ± 1.09 vs. 3.78 ± 2.97; p = .016). Notably, patients who stayed in the hospital for more than seven days exhibited a higher mean CVT GS score compared to those with stays of seven days or less.
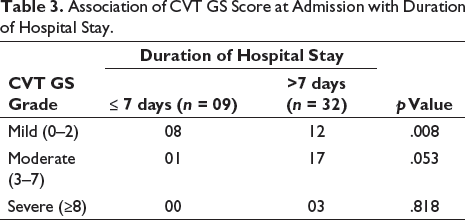
Additionally, the relationship between the severity of CVT assessed by CVT GS grade at admission and length of hospitalisation was investigated. The results revealed that a significantly larger proportion of patients with mild CVT GS grade upon admission had a hospital stay exceeding seven days (p = .008). Similarly, for patients with moderate and severe CVT GS grades, a higher number of individuals also remained hospitalised for more than seven days, although the results for both moderate and severe CVT GS grades were not statistically significant (p = .053, .818). Hence, it can be concluded that CVT GS grade observed at the time of admission does not serve as a reliable predictor of the duration of hospital stay (Table 3).
Association of CVT GS Score at Admission with Duration of Hospital Stay.
The PI by TCD ultrasound was calculated both at admission (day 1) as well as at day 3 of hospital stay in both right and left MCA. The mean PI in the left MCA was 1.22 at admission while 0.84 at day 3. Further, the mean PI in the right MCA was 1.25 at admission while it was 0.87 at day 3. Further, the association of PI at admission was analysed with clinical outcomes. The PI in left MCA at admission was significantly higher amongst those who expired as compared to those who survived (1.64 vs. 1.19; p = .003). Similarly, the PI in the right MCA at admission was also high amongst expired as compared to the survivors (1.63 vs. 1.23; p = .012).
Results discovered that the fatality rate among individuals with severe grades of CVT GS score is 66.67%, whereas no fatalities were observed in individuals with mild and moderate grades. The association between CVT GS score and clinical outcome was also analysed. The mean CVT GS score at admission was found significantly higher amongst those who expired in comparison to those who survived during the hospital stay (8.50 ± 0.70 vs. 2.94 ± 2.66; p = .006).
The association between Papilledema and clinical outcome was also studied. Among the group of 39 patients with Papilledema, 37 were discharged after treatment, and unfortunately, two patients did not survive. In the subset of 2 patients without Papilledema, both were successfully discharged. Our statistical analysis revealed that there is no significant association between these two variables (p = .742). This suggests that Papilledema alone cannot reliably predict clinical outcomes.
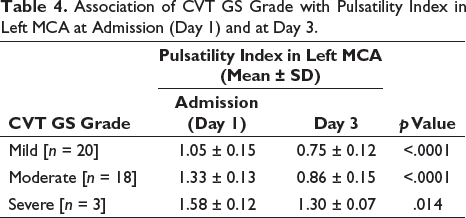
The association between PI at admission with CVT GS grading (mild, moderate and severe) was also studied. PI in left MCA was found significantly associated with CVT GS grade (1.05 ± 0.15 vs. 1.34 ± 0.13 vs. 1.58 ± 0.12; p < .05). Similarly, PI in right MCA was also significantly associated with CVT GS grade (1.10 ± 0.18 vs. 1.35 ± 0.15 vs. 1.59 ± 0.15; p < .05). However, as highlighted earlier, CVT GS grade alone is not a reliable predictor of the duration of hospital stay.
The analysis investigated the correlation between the CVT GS grade and the PI in the left MCA upon admission and on day 3. The results consistently revealed that the PI upon admission was significantly higher compared to the PI on day 3, across all CVT grades (Table 4). This indicates a considerable decrease in the PI values over time, suggesting potential improvements in cerebrovascular dynamics. These findings underscore the importance of monitoring the PI in the left MCA as a valuable parameter for evaluating cerebrovascular status and gauging the response to treatment in patients with CVT.
Association of CVT GS Grade with Pulsatility Index in Left MCA at Admission (Day 1) and at Day 3.
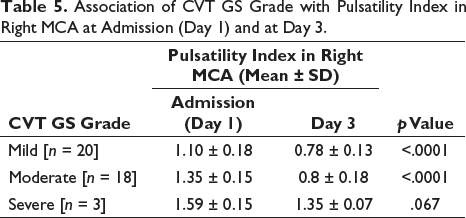
Furthermore, the analysis extended to examine the association between the CVT GS grade and the PI in the right MCA at admission and day 3. Similar to the findings in the left MCA, it was observed that the PI in the right MCA was higher at admission compared to day 3. This implies a decrease in PI values over time, suggesting potential improvements in cerebrovascular dynamics in the right MCA as well. However, it is noteworthy that the analysis revealed a non-significant result for the severe CVT GS grade when assessing the association between CVT GS grade and PI in the right MCA. This suggests that for patients with severe CVT GS grade, the reduction in PI from admission to day 3 may not be as pronounced or consistent as observed in other CVT GS grades (Table 5). Nonetheless, the overall trend of decreasing PI values from admission to day 3 in the right MCA indicates a potential improvement in cerebrovascular function during the early stages of CVT.
Association of CVT GS Grade with Pulsatility Index in Right MCA at Admission (Day 1) and at Day 3.
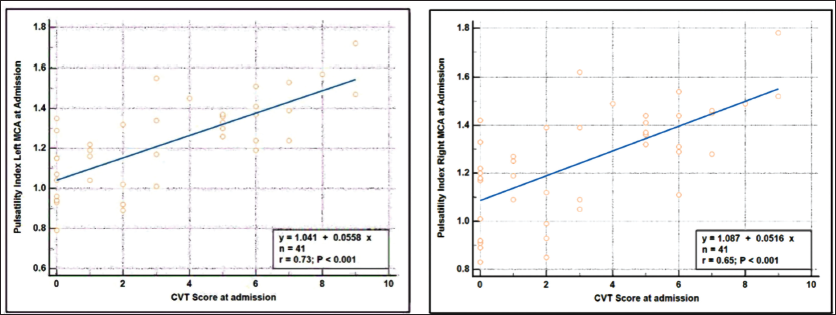
To assess the relationship between the PI in the left and right MCA at admission and the CVT GS score, the Spearman rank correlation coefficient test was employed. The findings revealed a strong positive and statistically significant correlation between these variables, suggesting that any alteration in the PI in the left and right MCA will lead to a significant change in the CVT GS score (r = 0.729, 0.646; p < .05) (Figure 1).
Spearman’s Rank Correlation Coefficient Between PI at Admission in Left and Right MCA with CVT GS Score.
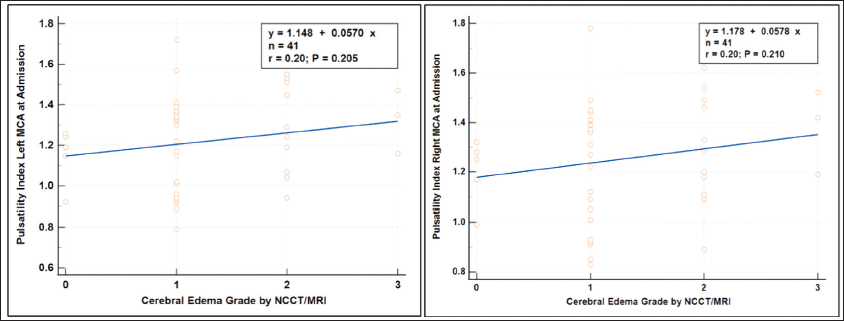
Furthermore, we assessed the correlation between PI in the left and right MCA at admission and the severity of cerebral edema as determined by NCCT/MRI brain scans. Cerebral edema was graded as follows: grade 0 indicating no cerebral edema, grade 1 indicating focal brain edema covering up to one-third of the hemisphere, grade 2 indicating involvement of more than one-third of the hemisphere, and grade 3 indicating cerebral edema with midline shift. Analysis using the Spearman rank correlation coefficient revealed a weak positive correlation between PI in both the left and right MCA and the severity of cerebral edema, although this correlation was not statistically significant (Figure 2).
Spearman’s Rank Correlation Coefficient Between PI at Admission in Left and Right MCA with Cerebral Oedema Grade.
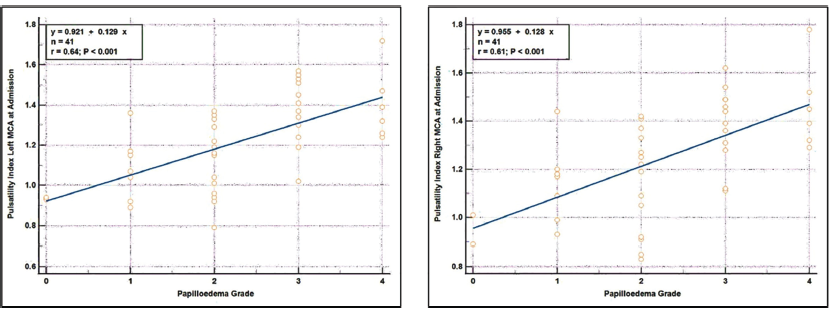
Moreover, an additional analysis was conducted to investigate the relationship between PI in the left and right MCA and the severity of papilledema. The results consistently revealed that for both MCAs, the mean PI was significantly higher in cases with a papilledema grade ≥ 3 compared to cases with a papilledema grade < 3. This indicates a clear association between higher PI values and increased severity of papilledema in both MCAs. These findings emphasise the potential of PI as an objective measure for assessing the severity of papilledema and its impact on cerebrovascular dynamics (Table 6).
Association Between Pulsatility Index of Left and Right MCA at Admission with Papilledema Severity.
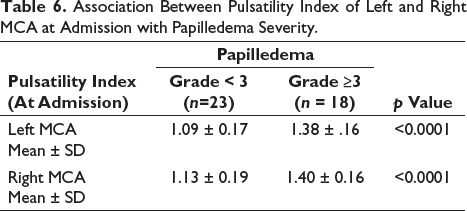
Furthermore, the Spearman rank correlation coefficient test was conducted to examine the relationship between the PI in the left and right MCA at admission and the papilledema grade. The findings reveal a strong, positive, and statistically significant correlation between the PI in the left and right MCA and the papilledema grade. This implies that any alteration in the PI in either the left or right MCA at admission will correspondingly result in significant changes in the papilledema grade as well (r = 0.64, p < .05; r = 0.61, p < .05) (Figure 3).
Spearman’s Rank Correlation Coefficient Between PI at Admission in Left and Right MCA with Papilledema Grade.
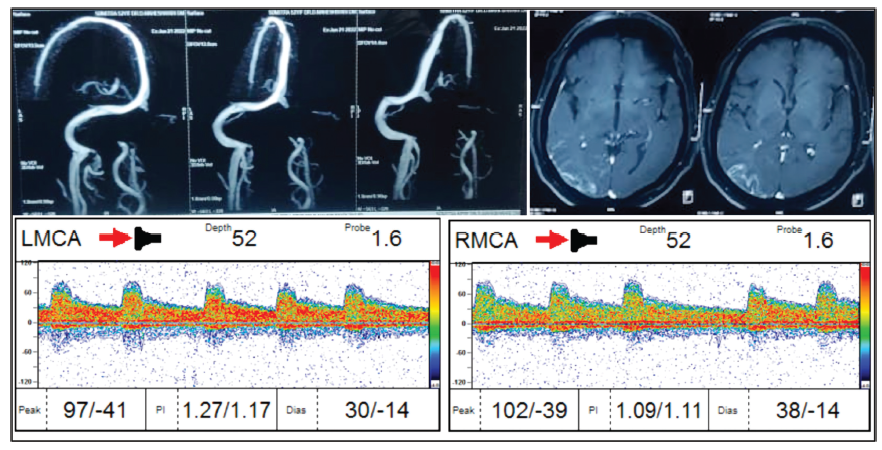
Illustrated is a patient case of CVT featuring thrombosis in the right transverse sinus and sigmoid sinus. MR Venogram imaging confirms the presence of thrombosis in these regions. The corresponding axial section of the MRI brain reveals parenchymal injury consistent with the thrombosed sites. Additionally, TCD findings indicate PI values for the left and right MCA (Figure 4).
Image Showing MR Venogram and Axial Section of MRI Brain along with the TCD Findings.
Discussion and Conclusion
The present study’s results stated that the overall participants’ median age was 29 years. The gender-specific median age was 27.5 years for males and 29 years for females. In the ISCVT study, the patients’ median age was 37 years. 4 Furthermore, the gender-specific median age found in one of the previous studies was 34 years for males and 42 years for females. 3 This suggests that the current study had a comparatively younger population. There were 31% males and 69% females included in the present study reflecting more females as compared to males. Previous studies have shown that there were 52% of females in one study 9 and 53% of females in the other respectively. 2 These results reflect that the current study had a higher incidence of CVT amongst females as compared to males.
Further, the present study found that one of the most common risk factors was Vitamin B12 deficiency (51%) followed by hyperhomocysteinemia (46%). The findings of the previous study indicated that individuals with CVT had notably elevated amounts of total homocysteine (measuring 14.7 ± 6.5 µmol/L) and reduced levels of vitamin B12 (measuring 185.4 ± 58 ng/mL), as compared to the control group (tHcys: 6.4 ± 2.7 µmol/L, vitamin B12: 299 ± 75 ng/mL). Hyperhomocysteinemia and low vitamin B12 were significantly more prevalent in CVT patients than in control subjects. 10 Another study revealed that nearly 70% of CVT patients had hyperhomocysteinemia and nearly 50% of the patients had low Vitamin B12 levels. 11
Other important risk factors that were found prevalent in the present study were tobacco chewing (27%), smoking (20%) and alcohol (17%). One of the studies found that 13.3% of the study population were smokers. 12 On the contrary, the study which assessed the addictions in the CVT patient revealed 72.2% were alcoholics and 60.6% were either addicted to tobacco chewing or smoking. 13 The varying addiction patterns may be due to differences in the inclusion of urban and rural populations.
OCP use is one of the most important risk factors in the present study among women CVT patients (32%). In a previous study, it was found that among women with CVT, the usage of oral contraceptives was more widespread, with 96% of them reporting using them, while the control group reported only 32% usage of oral contraceptives. 14 The ICVST study found that 54% of females with CVT reported using oral contraceptives. 4 Our study mainly comprised Indian participants, while the ICVST study primarily included individuals from a white population. Therefore, the difference in the pattern of oral contraceptive use may be due to variations in the use of contraception methods.
The present study found that the most common sinus involved in CVT patients is the right transverse sinus (41%) followed by the superior sagittal sinus (37%) and left transverse sinus (34%). 10% of the patients were found to the involvement of straight sinuses. A previous study stated that 46% of the patients had involvement of superior sagittal sinus while 32% had transverse/sigmoid sinus involvement. 15 On the contrary, another observational study found that superior sagittal sinus was involved in 62% of the patients followed by left and right transverse sinus (44.7%; 41.2%), while 18% of patients had straight sinus involvement. 4
The present study found that 49% of the patients had mild grade (0–2) of CVT GS score followed by 44% of the patients falling in the moderate grade category (3–7) and only 7% of patients falling in the severe grade (≥8) category. The current study found that the fatality rate is 66.67% amongst severe grades of CVT GS score while no fatality was found in the mild and moderate grades. A previous study also found similar results in the severe grade category where the fatality rate was found to be 61.4%. However, it is important to note that the study has also reported 0.4% fatality in the mild grade and 9.9% fatality in the moderate grade category. 16 The variation in the results may be attributed to two factors. First, the study population in the current research was relatively smaller compared to the previous study. Second, the difference in study locations may have also contributed to the disparity in findings, as the current study was conducted among the Indian population, while the earlier study was conducted among the Mexican population.
The current study revealed the presence of papilledema in 95% of the patients making it the most important clinical sign in CVT patients. In contrast, a previous study had only 26% of patients who had papilledema on fundoscopy 15 while another study had 28.3% of patients. 4 Moreover, the current study’s analysis revealed that the presence of papilledema did not exhibit a significant association with in-hospital outcomes for CVT patients. Similarly, the previous study also did not establish any link between papilledema and clinical outcomes. 17 These consistent findings across studies imply that while papilledema may serve as a valuable clinical tool for CVT, it may not necessarily predict or influence patient outcomes during the hospital stay.
In light of the limited existing clinical research on the subject, this novel study aimed to explore the relationship between CVT GS scoring, TCD-derived PI, and clinical outcomes among patients with CVT. The study found a correlation between PI at admission with in-hospital clinical outcomes. The PI in both right and left MCA was significantly higher amongst those who died during the hospital stay as compared to those who were discharged. Thus, PI at admission can be used as a prognostic marker amongst CVT patients. Similarly, a correlation between CVT GS score at admission and clinical outcome was also studied, revealing that CVT GS score was significantly higher amongst those who expired during the hospital stay. This result highlights that in addition to PI, CVT GS score can also be used to assess the prognosis in CVT patients.
The analysis utilising Spearman’s Rank Correlation Coefficient unveiled a statistically significant positive linear correlation between the PI assessed in the left and right MCA with the CVT GS score. The findings suggest a direct and proportional relationship between the PI and the severity of CVT. The observed correlation supports the notion that changes in the PI reflect alterations in the cerebrovascular dynamics associated with CVT. These results have important implications for prognostic evaluation in patients with CVT. The PI, derived from TCD measurements, can serve as a non-invasive tool to assess hemodynamic abnormalities in CVT patients. Moreover, the significant correlation with the CVT GS score underscores the potential of the PI as a prognostic marker for disease severity and progression. This can aid in early risk stratification, treatment planning, and monitoring of therapeutic interventions, ultimately leading to improved patient management and outcomes.
One of the limitations of the study is its relatively small sample size. Furthermore, it is a single-centred study conducted exclusively in the Hadoti region, which restricts the generalisability of the findings. Additionally, the study only assessed in-hospital outcomes and did not conduct a longer follow-up period. Moreover, no control group was included to enable a comparison of the PI values. It is also important to note that patients with a history of CVA or recurrent CVT were excluded, which could potentially affect the relevance of PI values in such cases. Furthermore, MCA PI might get effected by vascular diseases both intracranially as well as extracranially.
Conclusion
In conclusion, the TCD-derived PI has a significant correlation with the clinical outcome amongst CVT patients. Thus, TCD can be incorporated as a bedside tool for the prompt evaluation of patients with CVT. The role of PI assessment of bilateral MCA can help in early prognostication and further management. This prognostic capacity further extends to its usage in making informed decisions regarding the optimal timing of patient discharge and in facilitating longitudinal monitoring during follow-up. Nevertheless, additional randomised studies of greater scale are necessary to further reinforce this conclusion.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Patient information remained confidential throughout the study, with careful safeguards in place.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.