
Abstract
For young people the online world affords creative, entertainment and socialisation opportunities but also poses risks including cyberbullying, grooming and harmful content. Little is known about online experiences of care-experienced young people, a vulnerable group who may benefit from online experiences but may be at increased risk online. This cross-sectional study used data from 11- to 16-year-olds in Wales from the School Health Research Network (SHRN) Student Health and Wellbeing Survey 2017/18 (n = 103,971). Cyberbullying, face-to-face bullying and other online experiences were analysed. The prevalence of these experiences and associated mean wellbeing scores were compared for young people in care (n = 1,921) and not in care (n = 83,551), controlling for socio-demographic variables gender, ethnicity and year group. Higher numbers of young people in care were involved in cyberbullying, bullying, sharing explicit images, problematic social media use and regular contact with online only friends. These online experiences were associated with lower mean wellbeing scores. Lower numbers of young people in care had access to smartphones and social networking sites from age 12, and lower numbers were regularly in online contact with close friends and a wider peer group. These online experiences were associated with higher mean wellbeing scores. Young people in care appear to be less involved with online experiences that positively impact wellbeing and more involved in online experiences that negatively impact wellbeing. Promoting positive online experiences and education around problematic social media use may be particularly valuable in helping young people living in care develop healthy, safe and positive online lives.
Introduction
The online lives of young people looked after
Young people spend large amounts of time online, with 32% of teens spending up to three hours on social media per day and 35% spending over three hours online (Scott, et al., 2019). Ofcom (2022) data show that 97% of young people aged 12 to 15 and 100% aged 16 to 17 have their own mobile phone. The online world is an important part of daily life for entertainment and socialisation (boyd, 2014), but also poses risks, including cyberbullying, grooming, and access to inappropriate or harmful content (Machimbarrenar et al., 2018). While there is an abundance of international research devoted to online and social media experiences, little attention has been paid to its impact on young people who are looked after.
In Wales in 2017 there were 5,960 children and young people looked after, representing .95% of the population aged under 18 (Stats Wales, 2021). Being looked after refers to any child or young person who is cared for by a local authority, either living within the family home, in foster care, in a residential home, or in a kinship care placement (Welsh Government, 2021). Being looked after is also commonly called being in care. Children may become looked after for varying reasons including as a result of, or being at risk of, abuse or neglect, child or parental disability or illness, and where families are considered to be in acute stress or with chronically inadequate parenting. Children and young people looked after are particularly vulnerable having poorer outcomes than their peers in relation to education (Sebba et al., 2015), employment (Stein, 2006), mental and physical health (Ford et al., 2007; Hill et al., 2003) and wellbeing (Selwyn et al., 2017). Children and young people looked after may have particular risks related to being online. They often have reduced online access compared with their non-looked after peers which can further increase susceptibility to online harm due to reduced confidence, lack of awareness of new technologies, and limited understanding of dangers (Cross et al., 2009). Unregulated online contact with birth families may also be a concern for children and young people looked after (McDowell et al., 2019). However, there are also particular opportunities for children and young people looked after through being online which can be a ‘leveller’ for vulnerable children and young people (Cross et al., 2009). For example, there are online communities catering to vulnerable groups (The Rees Foundation, 2022; Voices from Care Cymru, 2022), and family and peer relationships can be maintained online when young people move home and school often. Seemingly, both online risks and online opportunities may differ for children and young people looked after from the general population.
Research in relation to cyberbullying, online experiences and face to face bullying for children and young people looked after is limited. An exploratory study by Sen (2016) found that for participants with experience of care (n = 10) their usage of digital media did not differ significantly from their peers. Additionally, 17% (n = 13) of looked after children in Glasgow had been bullied at school within the previous year (Vincent & Jopling, 2018). Due to the small sample sizes of these studies, the findings should be carefully considered. In contrast, Guardian Saints' (2017) online survey of foster carers (n = 329) in the UK suggested 56% of young people in care have been at further risk through social media and being online including cyberbullying, inappropriate contacts and material, and grooming or attempted grooming (Corliss, 2023). However, these findings reflect the views of foster carers, not young people themselves. Increased understanding is needed regarding the online lives of children and young people looked after, including the benefits and challenges they may experience online (Sen, 2016).
Cyberbullying
Cyberbullying has been defined as “wilful and repeated harm inflicted through computers, cell phones, and other electronic devices” (Hinduja & Patchin, 2015, p. 11) and “an aggressive, intentional act carried out by a group or individual, using electronic forms of contact, repeatedly and over time against a victim who cannot easily defend him or herself” (Smith et al., 2008, p. 376). In this study the SHRN survey question describes cyberbullying as ”e.g. sent mean instant messages, email or text messages, wall postings, created a website making fun of someone, posted unflattering or inappropriate pictures online without permission or shared them with others”. There are differences in research findings regarding levels of cyberbullying perpetration and victimisation. A systematic review found cyberbullying perpetration varied between 6% and 46%, victimisation rates varied between 14% and 58%, and prevalence rates increased significantly between 2015 and 2019 (Zhu et al., 2021). According to the Office for National Statistics one in five children experienced online bullying in the year ending March 2020 (ONS, 2020). Recent figures for children and young people in mainstream schools in Wales found 9% reported having cyberbullied others and 18% reported being victims of cyberbullying (Page et al., 2021). Some research suggests links between online experiences including cyberbullying and young people’s mental health. Problematic social media usage as defined by the Social Media Disorder Scale (Van den Eijinden et al., 2016) has been shown as positively correlated with cyberbullying victimisation and perpetration (Craig et al., 2020) which have in turn been shown as associated with mental health problems (John et al., 2018; Zhu et al., 2021).
Bullying
Research suggests links between experiences of face-to-face bullying (hereafter termed bullying) and cyberbullying. Kowalski et al.’s (2012) study of students aged 11 to 18 (n = 4,531) showed bullying perpetration and victimisation were associated with higher frequency of cyberbullying perpetration and victimisation. A similar study in Canada of students aged 12 to 15 (n = 432) showed those who were cyberbullied were likely to be bullied and were likely to cyberbully others (Beran, 2007). A study of a large representative sample of adolescents in England (n = 120,115) showed that whilst bullying is more common than cyberbullying, both were associated with poorer wellbeing (Przybylski & Bowes, 2017).
Wellbeing
There is concern in the UK and internationally around decreasing wellbeing for young people (Casas & González‐Carrasco, 2019; Gromada et al., 2020; The Children’s Society, 2020). There are many and varied influences on wellbeing and young people’s increased social media usage, problematic social media usage, and cyberbullying have been shown to reduce life satisfaction (Viner et al., 2019). Some research shows that cyberbullying perpetration is linked to lower wellbeing (Kircaburun et al., 2019) but other research has found no relationship between cyberbullying perpetration and depression and anxiety (Giordano et al., 2021). More nuanced understandings of the impacts of different kinds of online experiences on wellbeing have been shown by Anthony et al. (2023) where regular contact with close friends and wider friendship groups was associated with higher levels of wellbeing, and regular contact with virtual friends was associated with lower levels of wellbeing.
In the UK, there are differences in how young people report subjective wellbeing. Girls report generally lower overall wellbeing and more mental health symptoms than boys, but boys are less likely to report mental health issues and access support (Department for Education, 2019). However, some research indicates that there are no observed wellbeing differences by gender until relationship factors such as family, peers and school connectedness are introduced (Patalay & Fitzsimons, 2016). Similarly, research suggests that there are no differences in subjective wellbeing according to ethnicity (Nazroo et al., 2018). Wellbeing has been shown to decrease as young people get older (Children’s Society 2020) and young people in care report lower wellbeing than young people not in care (Long et al., 2017). Overall young peoples’ subjective wellbeing is influenced by many factors and the intersections between wellbeing, online lives, living in care, and other demographic factors requires further exploration.
Purpose of the study
The purpose of this study was to compare cyberbullying involvement and online experiences of young people in care with those not in care, and to compare wellbeing scores related to cyberbullying involvement and different kinds of online experiences. Wellbeing in this study refers to a holistic measure of mental wellbeing as defined by the short version of the Warwick-Edinburgh Mental Wellbeing Scale (Warwick Medical School, 2021).
This study has two key hypotheses: (1) Young people living in care are more likely to be involved in cyberbullying than those not living in care. (2) Young people involved in cyberbullying are more likely to have lower wellbeing scores than young people not involved in cyberbullying.
The study also has two exploratory research questions: (1) Are there any factors that influence the likelihood of being involved in cyberbullying for young people in care? (2) Do some online experiences promote better wellbeing for young people living in care and involved in cyberbullying?
Methods
This cross-sectional study used data from the School Health Research Network (SHRN) Student Health and Wellbeing Survey (SHW) 2017/18 obtained from 11- to 16-year-olds in Wales, UK. The 2017/18 data were selected as opposed to the more recent 2019/20 survey data due to a wider range of variables relating to online experiences being available in the 2017/18 version.
Ethical approval for this study was granted by Cardiff University School of Social Sciences Research Ethics Committee. Informed consent was obtained from schools, parents and students. Schools had to register to take part in the survey and parents had the option to withdraw their child(ren) from data collection. Students’ participation was optional, with the first question in the survey asking for their consent to take part. All questions included an additional response option, ‘I do not want to answer’, except for the consent and year group questions.
School health research network survey
The SHRN 2017/18 survey was administered by schools and completed online by students themselves. Ninety-seven percent of all maintained mainstream secondary schools in Wales are members of SHRN. 210 SHRN member schools were invited to take part in the 2017/18 survey along with 6 independent schools. 193 schools (89%) took part in SHRN 2017/18. Parents were able to withdraw their child and 150 students were withdrawn. Of 142,631 students there were 103,971 respondents (73%) meaning the overall response rate was 65%. The SHRN survey sample matched the population of Wales closely and no survey weights were applied.
To maximise the capacity for a broad range of questions to be included, the survey consisted of three routes, with some common items included within all routes (asked of all students) and some included only in certain routes (asked of subsamples of students). Whilst the SHRN survey takes place every two years it is also part of the Health Behaviour in School-Aged Children (HBSC) international study on a four-yearly basis. The 2017/18 SHRN survey was part of the HBSC study and therefore one of the three survey routes included questions specified for the HBSC study. The HBSC study special focus for the 2017/18 data collection was online experiences. Further details about the HBSC study are available at www.hbsc.org.
Figure 1 shows the sample sizes for each of the three survey routes. The HBSC route, with 29,073 participants, asked additional electronic media communications questions that were not asked in the SHRN 1 and SHRN 2 routes. The sample sizes for questions asked through only one survey route remain large enough to develop robust national estimates. Sample sizes for each variable are shown in the results tables. These vary due to missing data because of participants skipping questions. Detailed methods for each SHRN survey year can be found elsewhere (Hewitt et al., 2019). Sampling and response rate for SHRN 2017/18.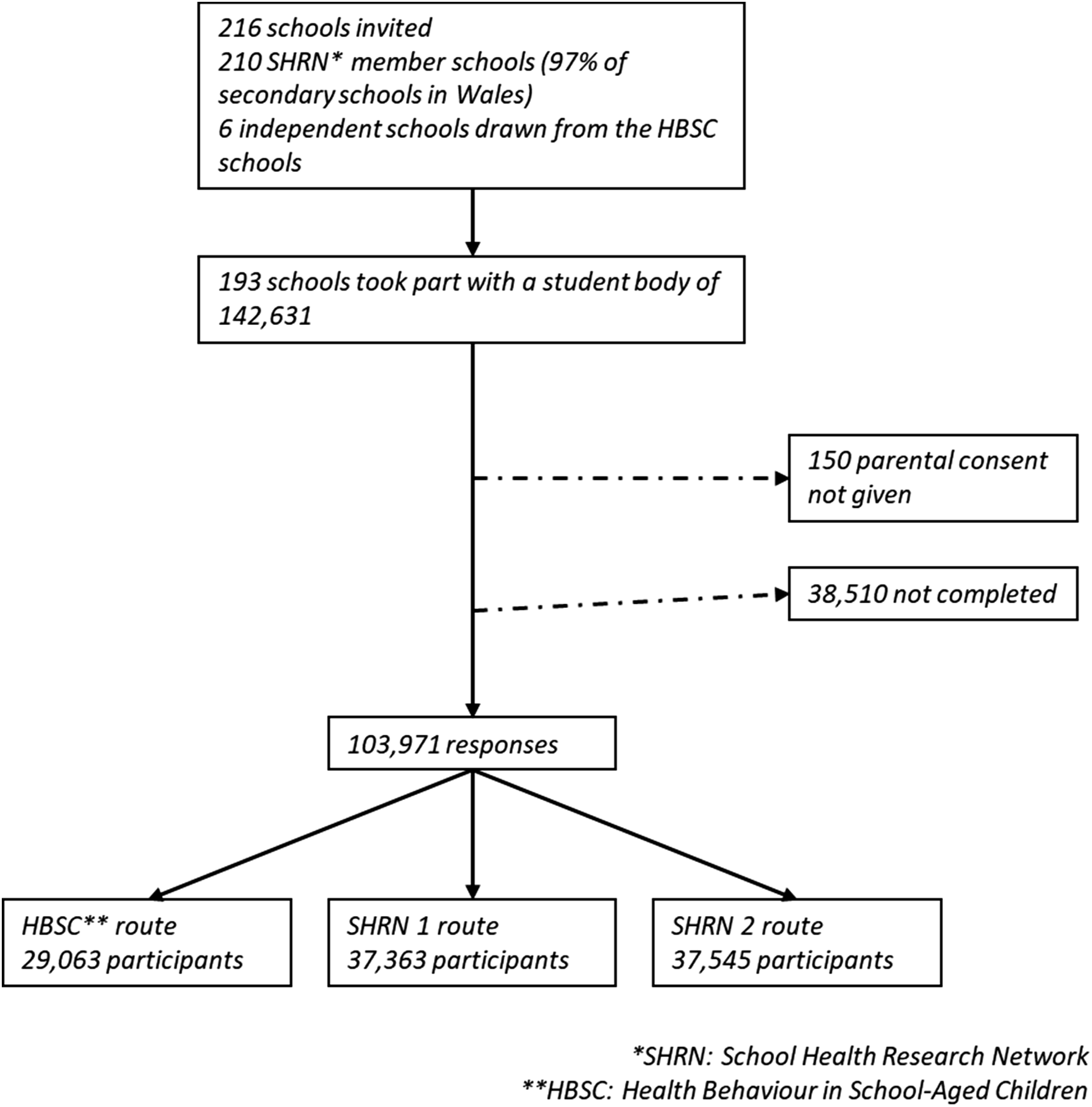
Primary outcomes
Cyberbullying involvement
In the SHRN 2017/18 survey cyberbullying is described as: “e.g. sent mean instant messages, email or text messages, wall postings, created a website making fun of someone, posted unflattering or inappropriate pictures online without permission or shared them with others”. All 103,971 participants were asked if they had been cyberbullied on a 5-point scale ranging from ‘I have not been cyberbullied in the past couple of months’ to ‘several times a week’. The responses were recoded to a binary variable of ‘has not been cyberbullied in the last couple of months’ or ‘has been cyberbullied once or more’.
29,063 participants following the HBSC route were also asked if they had cyberbullied others. The responses were structured and recoded in the same way as for having been cyberbullied. In total 24,471 respondents answered both questions about having been cyberbullied and having cyberbullied others. A binary variable was created for cyberbullying involvement (N = 24,471) and answering yes to either or both cyberbullying questions was coded as ‘involved in cyberbullying’ and answering no to both questions was coded as ‘not involved in cyberbullying’.
Wellbeing
The SHRN surveys use the SWEMWBS scale, a short version of the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS) (Warwick Medical School, 2021). WEMWBS was developed to monitor mental wellbeing in the general population and the short version SWEMWBS has been validated for populations of young people aged 15 to 21 (McKay & Andretta, 2017; Ringdal et al., 2018). Furthermore, SWEMWBS has been shown to be a valid scale for measuring differences in mental wellbeing for younger people (age 11–15 years) and young people in care (Anthony et al., 2022). The SWEMWBS metric score ranges from 5 to 35 with higher scores indicating better wellbeing. The mean SWEMWBS score from the SHRN 2019/20 survey was 24 (Page et al., 2021). Benchmarking of SWEMWBS on PHQ-9 and GAD-7 suggests that a SWEMWBS score >18–20 is indicative of possible mild depression, and a score <18 is indicative of probable clinical depression (Shah et al., 2021). In SHRN 2017/18 all participants were asked to complete the SWEMWEBS scale (N = 103,971) and there were 94,476 valid responses.
Covariates
Gender
Gender in the SHRN 2017/18 survey was established by asking in relation to how participants describe themselves today ‘Are you male or female?’. Gender was used as a covariate due to suggested differences in cyberbullying by gender (Page et al., 2021) and differences in the ways in which young people report wellbeing according to their gender (The Children’s Society, 2020).
Ethnicity
The SHRN 2017/18 survey used a 13-category measure of ethnicity. Given the small numbers of participants in all ethnic groups except White British a binary variable was created for ethnicity of White (White British, White Irish, White – Gypsy/Traveller, White – Other) and non-White (Mixed or multiple ethnic group, Pakistani, Indian, Bangladeshi, Chinese, African, Caribbean or Black, Arab, Other). Whilst there is little research linking ethnicity with cyberbullying or wellbeing, the influence of ethnicity on life outcomes including mental health, life satisfaction and wellbeing requires further exploration.
Year group
Participants were asked which year group they were in, and this variable was selected as a covariate because research suggests that subjective wellbeing decreases as young people get older (Children’s Society 2020).
Living in care
Being looked after refers to any child or young person who is cared for by a local authority, either living within the family home, in foster care, in a residential home, or in a kinship care placement (Welsh Government, 2021). Living in care is a commonly used term when referring to children and young people who are looked after. To establish whether a participant was in care at the time they completed the survey the participants were asked which adults live in the home where the participant lives all or most of the time (see Anthony et al., 2022 for further details of survey question and categorisation of care status). As a result of this question structure, young people living at home with a care order or receiving care and support from their local authority, and young people who have previously lived in care, would not be included as young people in care. Being in care was used as a covariate because there is evidence to suggest lower subjective wellbeing of young people in care (Long et al., 2017) and there is a lack of research comparing the online experiences of young people in care with those not in care.
Face to face bullying
The same question structure and recoding as cyberbullying was used in relation to bullying. The SHRN survey describes bullying as follows We say a person is BEING BULLIED when another person, or a group of people, repeatedly say or do unwanted nasty and unpleasant things to him or her. It is also bullying when a person is teased in a way he or she does not like or when he or she is left out of things on purpose. The person that bullies has more power than the person being bullied and wants to cause harm to him or her. It is NOT BULLYING when two people of about the same strength or power argue or fight.
Bullying was used as a covariate because of its strong relationship with cyberbullying (Beran 2007; Kowalski et al., 2012).
Online experiences
The SHRN survey 2017/18 asks participants about other aspects of their online lives such as: - Whether they have shared a sexually explicit image of themselves online, or had a sexually explicit image of themselves forwarded or shared by someone else. - How regularly they have online contact with close friends, with larger friendship groups, and with online friends (who they have not met in person). - The age they first had a smartphone, and the age they first had access to social networking sites such as Facebook, WhatsApp and Snapchat. - A social media disorder scale.
The Social Media Disorder scale (Van den Eijinden et al., 2016) uses nine questions around the prevalence of issues that may arise from social media usage (see Appendix 2). Answering yes to six or more of the nine questions is considered to indicate ‘problematic social media use’.
These various online experiences were used as covariates to explore these examples of online experiences in relation to the chosen demographic covariates as well as their potential links with the primary outcomes of cyberbullying involvement and subjective wellbeing.
Statistical analysis
The survey results were analysed using Stata (Version 13) and descriptive statistics were developed. Descriptive statistics and Log likelihood tests were used to identify significant variables, which were also tested for multicollinearity. Mean wellbeing scores across different groups were compared using t tests, and Chi-squared tests were used to compare numbers of young people involved in different online experiences according to the socio-demographic variables gender, ethnicity, year group and being in care or not. Logistic regression tested for factors associated with cyberbullying involvement and wellbeing. Odds Ratios (ORs) were reported. Cluster-robust standard errors for the estimated ORs were used to account for clustering within schools.
Results
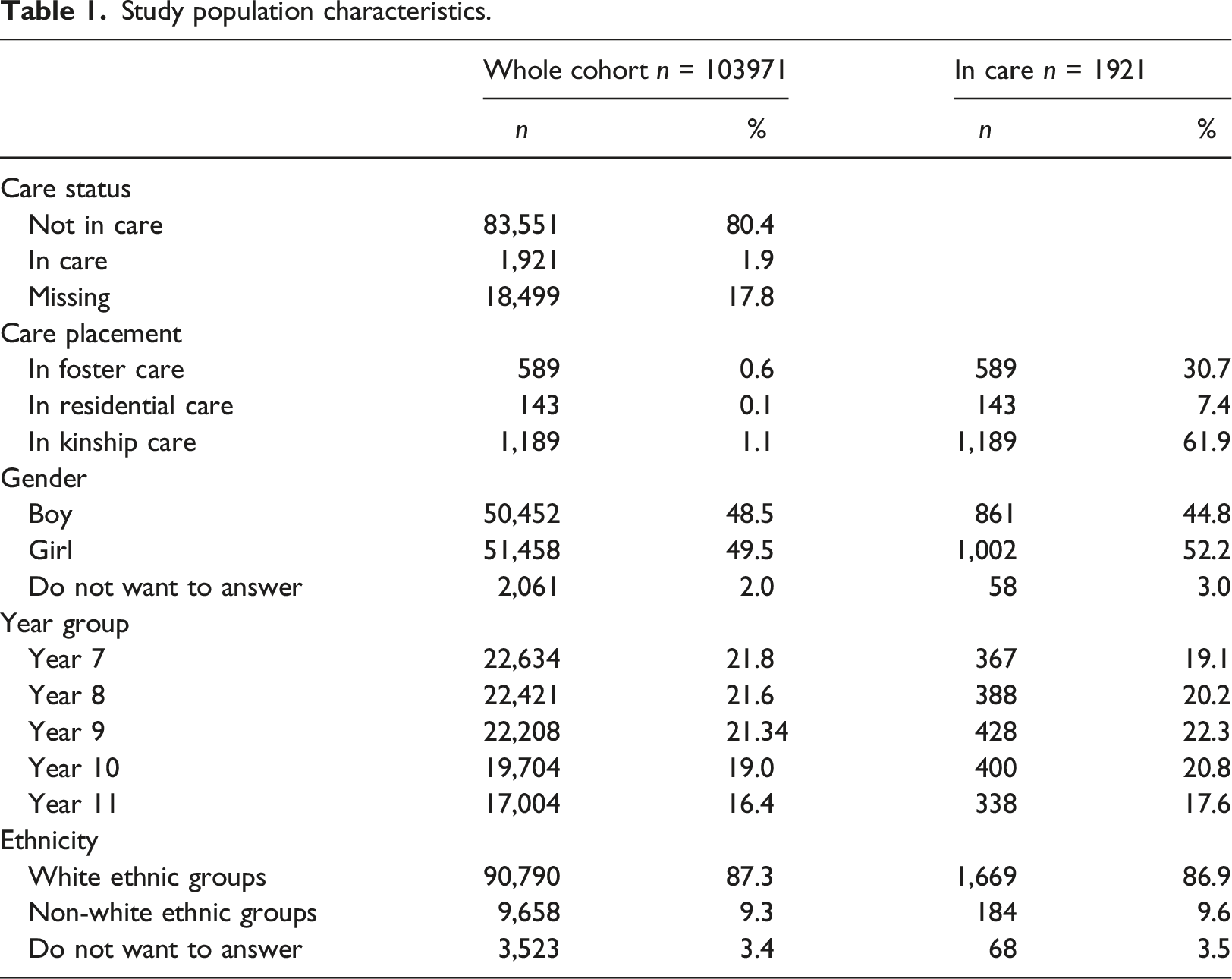
Study population characteristics.
Online experiences
Chi-squared results for young people not in care and in care for variables associated with online experiences.
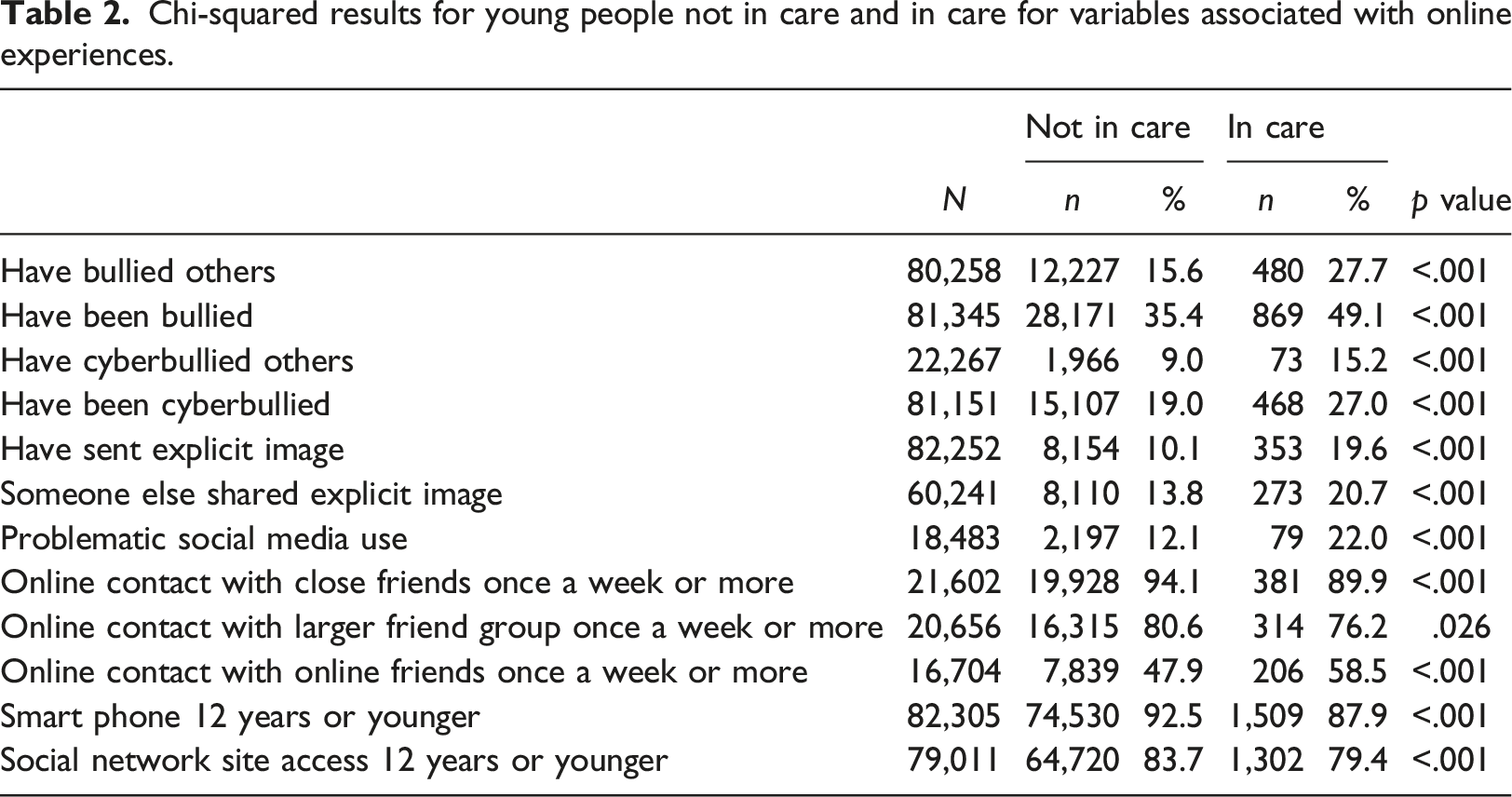
It is important to note the large sample sizes will increase the likelihood of statistical significance in these tests. For the in care cohort there were higher percentages of young people involved in bullying and involved in the online experiences cyberbullying, sharing explicit images, problematic social media use, and online contact with online only friends. By contrast, there were lower percentages for the in care cohort involved in the two online experiences of online contact with close friends and online contact with a larger friend group. In addition, the percentages of young people in care who had a smart phone and had access to social networking sites (SNS) by age 12 years were lower than for the not in care cohort.
Involvement in cyberbullying
Of all 103,971 participants 16.43% (n = 17,081) said that they had been cyberbullied one or more times in the last few months. Of the 29,063 participants who were asked if they had cyberbullied others 8.24% (n = 2,395) said that they had done so one or more times in the last few months. Of the 24,471 participants who answered both questions about being cyberbullied and cyberbullying others 20.31% (n = 4,970) answered yes to one or both questions and were therefore considered to be involved in cyberbullying.
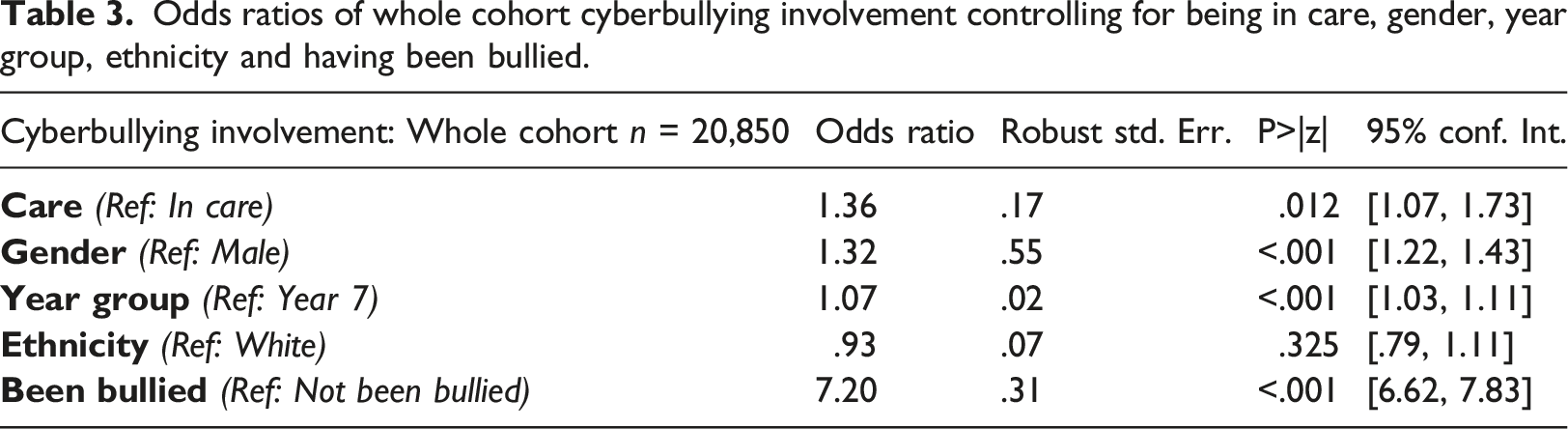
Odds ratios of whole cohort cyberbullying involvement controlling for being in care, gender, year group, ethnicity and having been bullied.
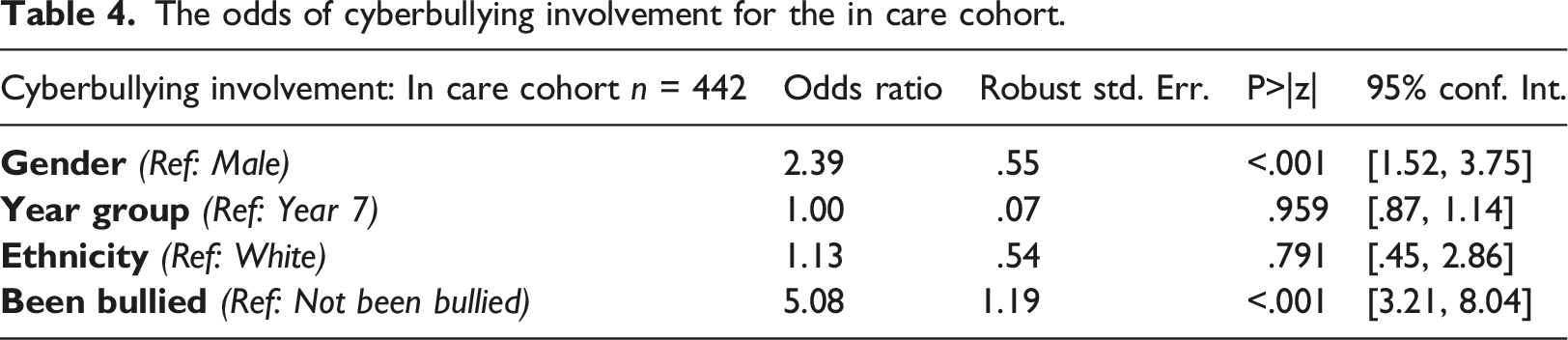
The odds of cyberbullying involvement for the in care cohort.
Cyberbullying and wellbeing
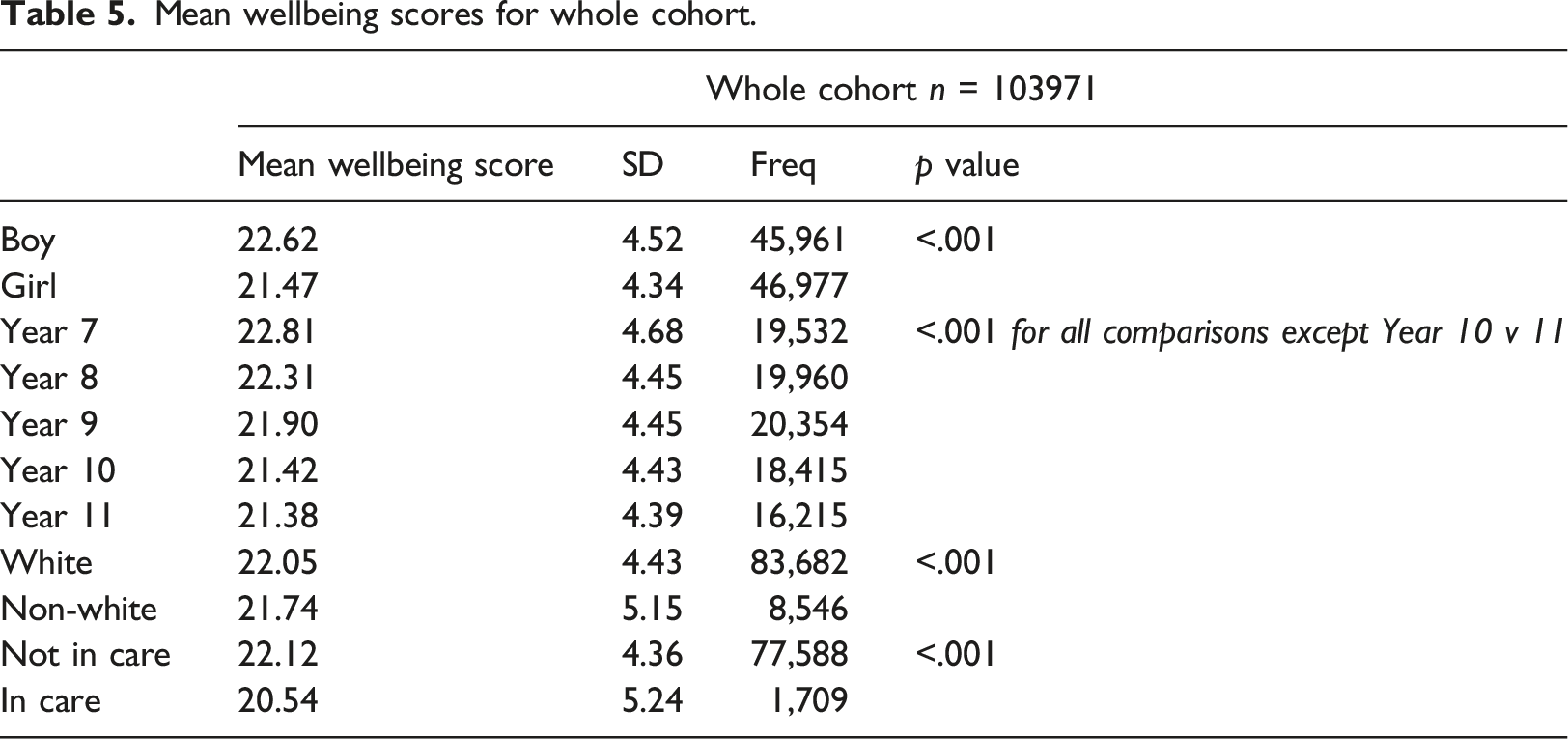
Mean wellbeing scores for whole cohort.
Mean wellbeing scores for not living in care and living in care cohorts.
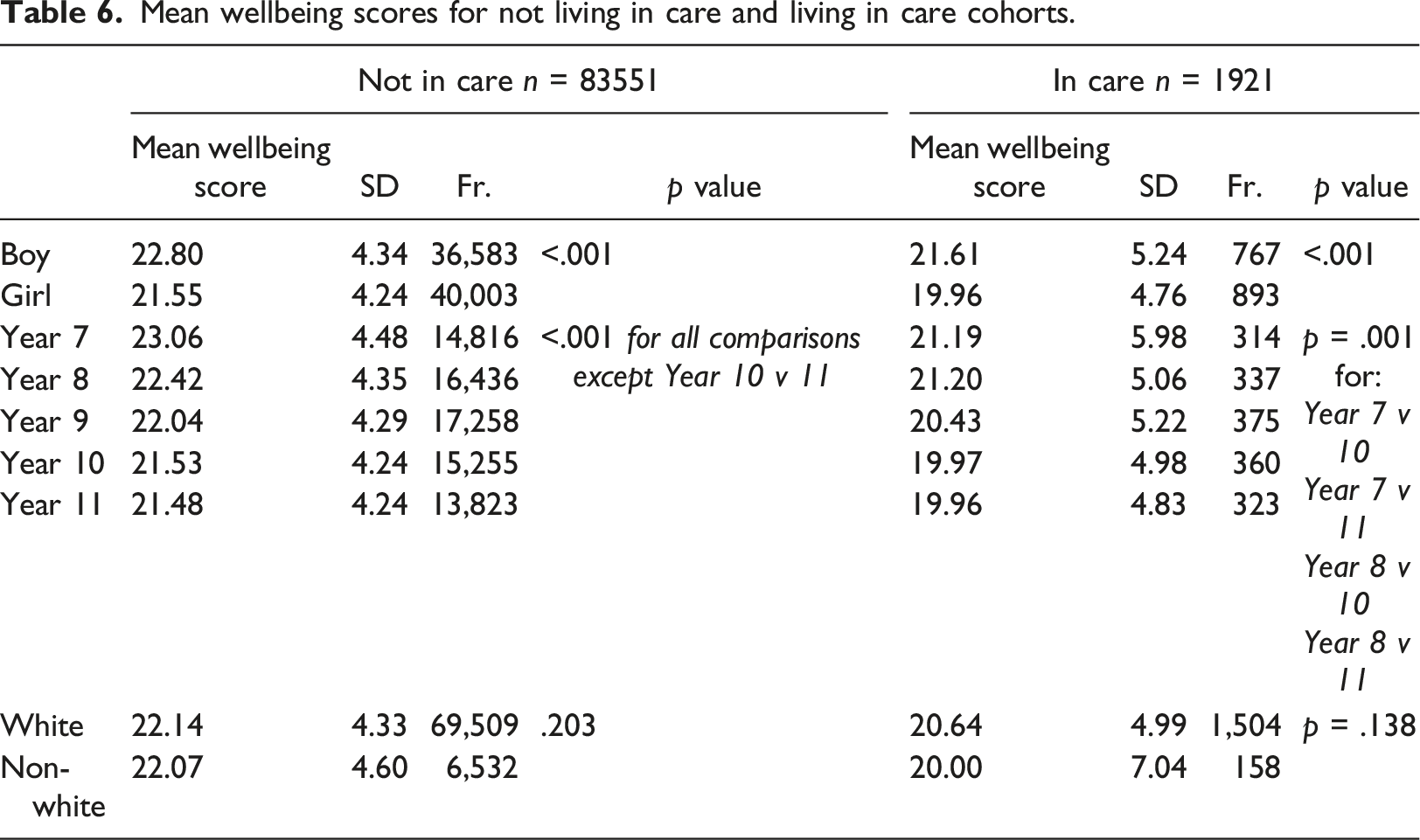
All three cohorts show statistically significantly lower wellbeing scores for girls than for boys, with the wellbeing score for girls in the in care cohort dropping below 20. A wellbeing score of less than 20 in the SWEMWBS questionnaire indicates possible mild depression. Whilst the difference in mean wellbeing scores between White and non-White respondents was statistically significant, these differences were no longer statistically significant when looking just at the in care cohort or just the not in care cohort.
The results show a decrease in wellbeing scores as young people get older for all three cohorts. In the whole cohort and not in care cohort the decreases are statistically significant except for the difference between years 10 and 11. For the in care cohort the only statistically significant differences were found when comparing year 7 with year 10 and with year 11, and when comparing year 8 with year 10 and with year 11. For young people in care in year 10 and year 11 the mean wellbeing score again drops below 20.
Overall, the results show that girls, young people in care, and older young people report significantly lower wellbeing.
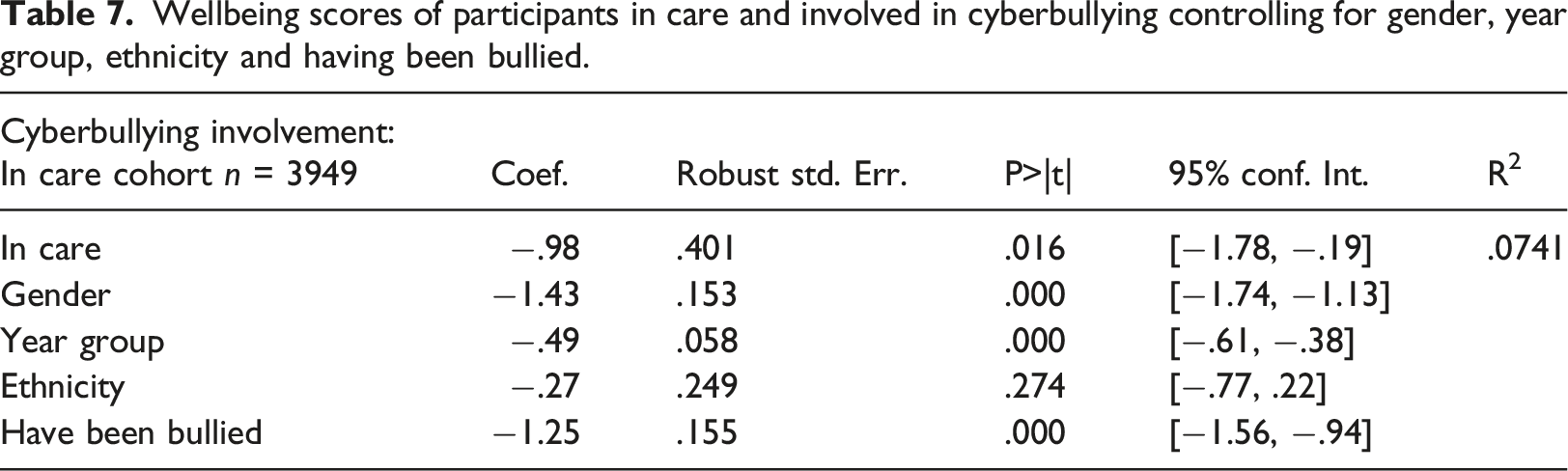
Wellbeing scores of participants in care and involved in cyberbullying controlling for gender, year group, ethnicity and having been bullied.
Online experiences and wellbeing
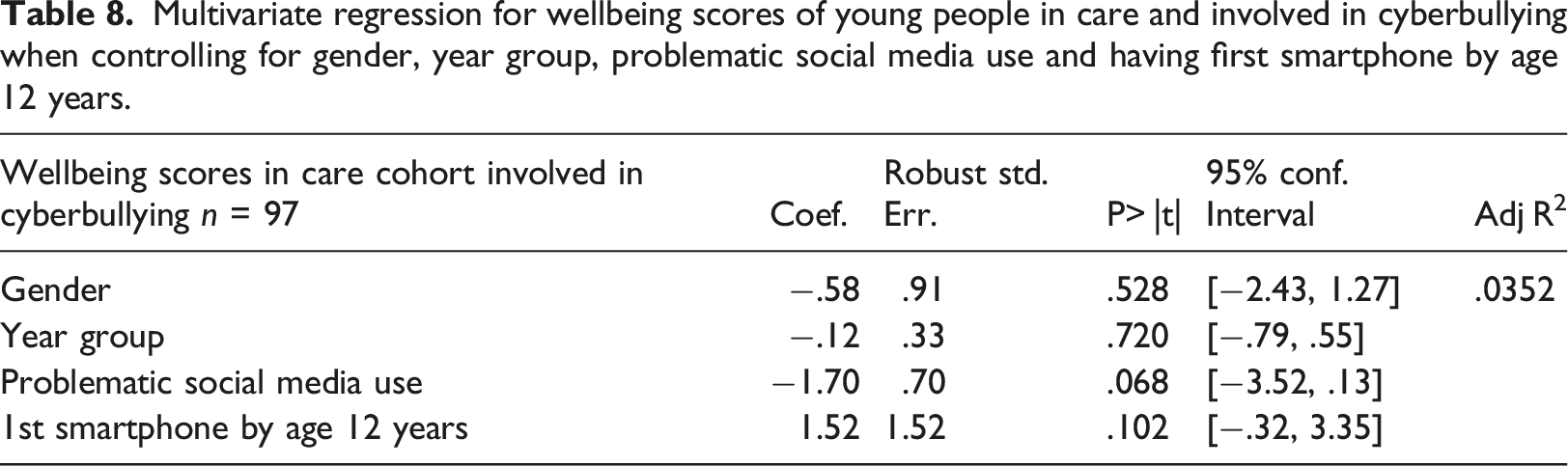
Multivariate regression for wellbeing scores of young people in care and involved in cyberbullying when controlling for gender, year group, problematic social media use and having first smartphone by age 12 years.
Young people who had their first smartphone by age 12 reported higher wellbeing than those who had their first smartphone age 13 or older. The same was true for young people who had first accessed social networking sites by age 12. However, it is important to note that in no cases do the mean wellbeing scores drop below 20 which would indicate possible mild depression.
Multivariate regressions were carried out to look at the impact of different online experiences on wellbeing for young people in care and involved in cyberbullying whilst controlling for gender, year group and ethnicity. Many of the dependent variables relating to online experiences were correlated. As a result, multivariate regressions tests were carried out separately for each of the online experience dependent variables, controlling for gender, year group and ethnicity. Many of the online experiences no longer had a statistically significant association with wellbeing for young people in care and involved in cyberbullying. Ethnicity appeared to have a greater impact on wellbeing for this cohort, but these results were treated with caution due to the large difference in sample size between White and non-White participants. Ethnicity was therefore dropped from further multivariate logistic regression models.
The two online experiences that lead to statistically significant changes in wellbeing for young people in care and involved in cyberbullying were: having problematic social media use and having their first smartphone by age 12 years. Having problematic social media use showed a −1.76 drop in wellbeing score when controlling for gender, year group and ethnicity. Having their first smartphone by age 12 years showed a 2.31 increase in wellbeing score when controlling for gender, year group and ethnicity. Both of these differences in wellbeing were statistically significant (p < .001) and these two dependent variables were not correlated.
A multivariate regression test was carried out for young people in care and involved in cyberbullying using the dependent variables gender, year group, problematic social media use and having first smartphone by age 12 years. The results are shown in Table 8. The results show that for young people in care and involved in cyberbullying, problematic social media use shows a −1.70 decrease in wellbeing scores that is statistically significant. Having a first smartphone by age 12 years is no longer statistically significant.
Discussion
The study confirmed our first hypothesis that young people living in care are more likely to be involved in cyberbullying than those not living in care. When controlling for gender, year group, ethnicity and having been bullied, the odds of being involved in cyberbullying are 35% higher for young people in care than young people not in care.
In keeping with existing literature, this study demonstrates a clear link between cyberbullying involvement and having been bullied. Young people were more than seven times as likely to be involved in cyberbullying if they have been bullied. This is also true for young people in care who were five times more likely to be involved in cyberbullying if they had been bullied. Girls were more likely to be involved in cyberbullying than boys for those in care and for those not in care.
The study also confirmed our second hypothesis that young people involved in cyberbullying are more likely to have lower wellbeing scores than young people not involved in cyberbullying. Our findings suggest that for young people in care being cyberbullied was associated with a mean wellbeing score 1 point lower than young people not in care. For young people in care who were already involved in cyberbullying changes in mean wellbeing scores associated with other online experiences were no longer statistically significant. This suggests that the decrease in wellbeing associated with being in care and involved in cyberbullying means other negative online experiences have no further negative impacts on wellbeing. Similarly, having weekly or more contact with close friends or larger friendship group no longer have positive impacts on wellbeing for this cohort. Involvement in cyberbullying is a particularly important online experience to monitor for young people in care.
With regard to our exploratory research questions, other online experiences such as having a first smartphone by age 12, having access to social networking sites by age 12, and having weekly or more online contact with close friends appear to be associated with better wellbeing. However, young people in care are less likely than their peers not in care, to demonstrate these experiences. By comparison, being involved in bullying and cyberbullying, having problematic social media use, sharing explicit images online or having explicit images shared by others, and having weekly or more online contact with online friends (who you have not met in person) appear to be associated with lower wellbeing. The results suggest young people in care are more likely than their peers not in care to be involved in these online experiences.
These findings suggest it is important for carers and professionals to be aware that young people in care are less likely to be involved with positive online experiences and are more likely to be involved in negative online experiences. Education around positive online experiences, staying safe online, and experiences that might constitute problematic social media use may be particularly important for young people in care.
A very high percentage of young people have access to their first smartphone and social networking sites by age 12 years, and those who do appear to have higher mean wellbeing scores. However, young people in care are less likely than their peers not in care to have access to their first smartphone and social networking sites by age 12 years. It is important to note however, the minimum sign-up age for Facebook and Snapchat is 13 years, and for WhatsApp and Instagram is 16 years. Participant age is not verified resulting in high numbers of young people accessing social networks younger than suggested minimum ages.
For young people in care and involved in cyberbullying who may be particularly likely to have lower wellbeing, having had access to a first smartphone by age 12 could improve their wellbeing. However, developing problematic social media use can further decrease wellbeing leaving the positive impact of having a smartphone no longer significant. It is hypothesised that whilst having access to a smartphone can be associated with higher wellbeing, this increase can be outweighed by negative online experiences such as cyberbullying and problematic social media use. This is an important consideration for practitioners and carers working with young people in care in relation to how online access for young people in care is managed and monitored.
Strengths and limitations
There is limited research looking at the online lives of children and young people looked after. This study expands online experience beyond cyberbullying by including other types of online experiences. Whilst existing research looks at impacts of bullying and cyberbullying on wellbeing, this research looks at the interactions between a variety of online experiences with wellbeing, specifically for young people in care.
The SHRN survey is a large representative survey of young people in Wales representing the views and experiences of young people themselves. However, self-report surveys represent what participants are willing to share and can be subject to reporting biases such as memory recall and social desirability, particularly when covering sensitive or emotional issues. The survey is completed within mainstream schools only, meaning that young people in specialist educational provision are not represented, and those truanting or suspended from school may be under-represented.
Participants were asked whether they would describe themselves today as male or female. Non-binary gender identities were therefore not captured in the 2017/18 survey but have been included in later cohorts. By asking participants which adults live in their current home the survey does not rely on phrases that could be misinterpreted such as ‘looked after’ or ‘in care’. However, this means the in care cohort includes participants who ticked ‘foster carers’ or ‘I live in a residential or children’s home’ and does not include those living at home in local authority care. 1.85% of participants were included in the in care cohort. Whilst Welsh Government population data for 2017 shows .95% of children and young people under 18 years were looked after, the highest numbers of children and young people looked after are aged 10–15 years and the SHRN survey age range is 11–16 which may explain the higher percentage of survey respondents in care.
Welsh Government data shows more boys are looked after than girls including those age 10 to 15-year whereas the in care cohort from the SHRN 2017/18 survey was 45% male and 52% female. This discrepancy with Welsh Government data should be further explored but suggests that boys in care may be less likely to complete the survey than girls. With regard to year group, the results are in-keeping with research that suggests subjective wellbeing decreases as young people get older, and therefore the online lives of older young people beyond age 16 years should be explored.
Cyberbullying is used as a primary outcome in this study, but the survey question refers only to cyberbullying ‘in the past few months’. Different definitions and timeframes in relation to cyberbullying could provide greater insights.
Recommendations
Education around positive social media use as well as the risks of negative online experiences may be particularly important for young people in care. Consideration should be given to the age at which young people in care have their first smartphone and access to social networking sites compared with their peers who are not in care. Regular online contact with friends and peers is to be encouraged. However, regular contact with online only friends should be considered in the context of other online contacts and may require closer monitoring by primary caregivers. Signs of problematic social media use should be carefully monitored to ensure that the potential benefits of social media to young people in care are not outweighed by problematic use and subsequent negative impacts on their wellbeing.
Footnotes
Acknowledgements
The CASCADE Partnership receives funding from Health and Care Research Wales and this study was funded as part of the Health and Care Research Wales Social Care Grant funding scheme.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health and Care Research Wales and Wolfson Foundation.
Data availability statement
Data underpinning this analysis is available upon reasonable request to the School Health Research Network and completion of the necessary data application documentation ![]() .
.