
Abstract
It is established that the development of psychological well-being and cognitive skills for Looked After and Adopted Children/Young People (LAACYP) is impacted by their experiences before and after entry into care. Language and communication skills are typically considered to have a reciprocal relationship with cognitive development, but the language skills of the LAACYP population are currently underspecified. The current study explores the severity and specificity of language and communication difficulty in a LAACYP population and the association between these difficulties and several care-related factors, including mental health and Adverse Childhood Experiences (ACEs). Fifty-seven children aged 4–16 either in foster care or an adoptive placement were sampled via carer-report, using the Children’s Communication Checklist 2. Forty-two of these children’s mental health needs were also sampled using the Assessment Checklist for Children. The child’s social worker completed information regarding ACEs and care-related factors. Based on UK norms, the performance of 68% of the children sampled was consistent with the lowest 10% of the general population for language and communication ability. Similar levels of severity were found for both structural and pragmatic abilities. Language and communication difficulties were associated with older children, later age of entry into care and placement type (foster care vs. adoption) but not placement disruption. A significant relationship was found between mental health and language difficulty, but no link was established with ACEs. This study highlights the severity and pervasiveness of language and communication impairment among many of the LAACYP population and its association with psychological well-being.
Keywords
Introduction
Effective language and communication play a crucial role in children’s typical development, with language impairment associated with range of difficulties including poor academic performance, social competence and self-regulation (Armstrong et al., 2017; Cross, 2018; Stock & Fisher, 2006). Many childhood communication difficulties persist into adolescence and adulthood without intervention and thus early identification is associated with improved outcomes (Cohen et al., 2013; Schoon et al., 2010). It is recognized that speech and language services are an underdeveloped resource with Looked After and Adopted Children/Young People (LAACYP) populations (Snow, 2009). Delays in language development may go unnoticed due to complex presentations inherent in LAACYP or the salience of other concerns such as child protection or mental health (Hagaman et al., 2010; Millward et al., 2006). Thus, in line with recent UK legislation (Children and Social Work Act, 2017), research studies have highlighted the need for greater understanding of the specific language and communication needs of LAACYP to support interventions (Cross, 2018; Raby et al., 2019).
Identifying and characterizing the language and communication needs of LAACYP
Chambers et al. (2010) found carers of 52 foster care children reported speech and language difficulties were as prevalent as more widely investigated difficulties in emotional dysregulation (26% and 24% respectively). Furthermore, Chambers et al. found these language and communication needs were the least likely difficulties to be acted upon over a 6–12-month follow-up. McCool and Stevens (2011) assessed language needs in 30 adolescents in residential care using a carer-report measure of pragmatic and structural language difficulty. Nineteen adolescents met the criteria for possible impairment, much of it severe and pervasive in nature and with two thirds falling within the lowest 10% of functioning based on UK norms. None of these children had previous involvement with speech and language therapy. Unfortunately, McCool and Stevens did not report on the profile of pragmatic versus structural language aspects across the population. However, the relatively high proportion of autism-like profiles is suggestive of possible systematic differences in pragmatic impairments.
The mental health of LAACYP and language and communication needs
Young people in care typically have significantly greater mental health needs and more emotional and behavioral difficulties/disorders (EBD) than those not in care (Jacobsen et al., 2020, Rayburn et al., 2016). A recent meta-analysis found that language deficits may occur in up to 81% of children with EBD (Hollo et al., 2014). A further meta-analysis indicated that children with language difficulties are twice as likely to subsequently develop EBD than their typically developing peers (Yew & O’Kearney, 2015). Conti-Ramsden et al. (2013) for example, found that emotional difficulties were reported by over 4 times as many adolescents with a diagnosis of developmental language disorder (DLD; previously referred to as specific language impairment or SLI) than those without DLD (28.3% and 6.6% respectively). Similarly, Beitchman et al. (2001) found that children diagnosed with DLD before age five experience almost twice the frequency of psychiatric symptoms by adulthood as typically developing children (40% and 21% respectively). The direction of the association between quality of mental health and language development is still unclear but it has been argued that the high frequency of EBD in young people with language needs could be partly due to the stress associated with maladaptive social skills in everyday life (Wadman et al., 2011).
Specifically in LAACYP, Chambers et al. (2010) reported similar levels of emotion dysregulation and speech and language concerns although they did not explore the associations between these variables. Giannitelli et al. (2011) found that a foster care sample in an inpatient mental health setting demonstrated greater impairments in complex language tasks, word identification and phonological ability than those who were not in foster care. However, the severity of the mental health presentation which warrants inpatient care limits the generalizability of these findings.
Adverse childhood experiences of LAACYP and their language and communication needs
LAACYP are often subject to significant degrees of adverse childhood experiences (ACEs), such as maltreatment, neglect and other forms of trauma (Rayburn et al., 2016). A recent meta-analysis of 26 studies found that on average maltreated children were 1 SD below the expressive and .5 SD below the receptive language skills of non-maltreated children (Lum et al., 2015). Language acquisition may be particularly sensitive to the impact of maltreatment and trauma due to the importance of environmental stimulation from others for effective acquisition (Tamis-Lemonda et al., 2014). Some evidence suggests that children’s pragmatic language may be particularly sensitive to the effects of maltreatment because this knowledge develops in the context of social interactions and experiences on which maltreated children frequently miss out (Sylvestre et al., 2016).
Zajac et al. (2019) sampled a cohort of young children with a previous history of maltreatment who had either been placed in foster care or continued to reside with their birth parents. Both groups demonstrated impaired receptive language ability, thus highlighting the deleterious impact of early maltreatment on language development. However, the group in foster care had better receptive language scores, falling in the 23rd percentile in comparison to the 10th percentile in children who resided with their birth parents. This suggests that entry into care may have ameliorative effects on language outcomes.
The impact of trauma on development is thought to be cumulative, with developmental delay increasing with the number of concurrent risk factors over time (Horan & Widom, 2014). The longer the pre-care experience the more likely a child is to be exposed to adverse conditions, maltreatment and trauma (Chambers et al., 2010). Tarren-Sweeney (2008) demonstrated that length of time with carers prior to removal into care explained 10% of variance in mental health difficulty as measured by the ACC in a sample of 347 young people in care. Furthermore, Windsor et al. (2011) reported on language learning of young children in foster care who were previously in institutional care. Entry into foster care by 24 months was associated with improvements in language functioning at 6- and 12-month follow-ups which were not present for those still in institutional care or those placed at 24–31 months.
While entry into care is thought to improve outcomes for maltreated children, not every young person’s experience of care is optimal and a range of care-related factors can impact developmental and psychological outcomes (Tarren-Sweeney, 2008). Children in foster care, for example, have been reported to have unfavorable cognitive, educational and psychosocial outcomes in comparison to children in adoptive placements (Jiménez-Morago et al., 2015; Vinnerljung & Hjern, 2011). In addition, adopted children have been shown to develop better-quality peer relationships than foster children (DeLuca et al., 2019).
Another important care-related factor is placement instability, which has been shown to impact emotional and behavioral outcomes (Villodas et al., 2016). Placement instability may in turn have an impact on language development, due in part to children being unable to form a lasting attachment relationship with an alternative caregiver when subject to regular disruption (Bederian-Gardner et al., 2018). Language development is scaffolded by caregiver sensitivity and attunement in the context of a secure attachment relationship (Golinkoff et al., 2015). Raby et al. (2019) demonstrated that improved attachment relationships with alternative caregivers resulted in gains in receptive vocabulary skills in toddlers in care. Children of carers who completed an attachment and biobehavioral training program demonstrated receptive language skills close to the normative mean and over .5 SDs above children whose carers had not received the intervention.
The current study
The primary aim of the current study was to investigate the language and communication needs of LAACYP. Consistent with previous studies (e.g. McCool & Stevens, 2011), we predicted that a sample of LAACYP would demonstrate significant language and communication difficulties as measured by their CCC-2 scores and these difficulties would be under-represented in terms of referrals to relevant Speech and Language services. We also predicted that a LAACYP sample would demonstrate greater difficulty in pragmatic language ability in comparison to structural ability, as measured by CCC-2 subscales.
The secondary aim of the study was to explore care-related factors in the lives of LAACYP that contribute to language and communication difficulty. We hypothesized that greater language and communication difficulties would be associated with older children, later age of entry into care, smaller proportion of life in care, fewer placements (conversely greater levels of placement disruption), and with poorer mental health. We also hypothesized that more children in foster care placements would demonstrate greater language and communication difficulties than those in adoptive placements.
The final aim of the study was to explore how mental health may influence the relationship between ACEs (such as trauma, maltreatment) and language and communication ability. We predicted that mental health measured by the ACC would mediate the relationship between ACEs and language and communication ability in a LAACYP sample.
Methods
Participants
Fifty-seven young people aged 4–16 years old (median = 8 years 8 months, range = 12 years 10 months) registered with a UK Looked After and Adopted Children’s public health service participated in the study. The nature of the language measures meant that only children without a diagnosed learning disability, and with a carer or adoptive parent/s who spoke English as a first language, were eligible to participate. Eleven of the 57 young people shared a carer with another of the participants. Four carers reported on two different children and one carer-reported on three different children.
Both genders (male = 32, female = 25) and placement types (foster care = 31, adoption = 26) were approximately equally represented in the sample (gender: χ2 = .86; placement type: χ2 = .44). The sample included young people who had experienced a range of placements from 1 to 15, 2 being the most frequent number of placements. Two thirds of participants had been in their current placement for 4 years or less, but only 15.8% of participants had been in their placement for less than 1 year. Participants age of entry into care was wide ranging, from birth to 16 years. Only 17.5% of participants entered care at birth, but a substantial proportion (66.7%) of the participants entered care before age 5. Three young people in the sample had a confirmed diagnosis of Autism Spectrum Disorder (ASD). Twenty-nine young people had current or previous involvement with community pediatrics, with eight undergoing assessment and/or intervention through speech and language therapy services. Twenty-seven of the young people had previous or current involvement with mental health services.
The study design was approved by the Research Ethics Committee Northern Ireland, approval # 19/NI/0124.
Measures
Language strengths and difficulties
The Children’s Communication Checklist–2 (CCC-2; Bishop, 2003) is a 70-item carer-report measure designed to measure strengths and difficulties in language and communication in young people between the ages of 4 and 16 years old. The CCC-2 specifically measures production, structure, pragmatics, as well as behaviors associated with ASD. It focuses on behaviors relevant for everyday communication. The frequency of language behaviors is assessed on a 4-point scale from “Less than once a week (or never)” to “several times (more than twice) a day (or always).” The measure contains 10 subscales in total with a mixture of questions asking about potential strengths (positive indices) and difficulties (negative indices). Four subscales can be considered to measure aspects of language production and structure: (A) speech, (B) syntax, (C) semantics and (D) coherence. A further four subscales can be considered to measure the use and understanding of social context in communication (pragmatics): (E) inappropriate initiation, (F) non-verbal communication, (G) use of context and (H) stereotyped language. An additional two subscales assess behaviors potentially indicative of ASD: (I) social relations and (J) interests.
A General Communication Composite (GCC) can be calculated as the sum of the A–H subscale scores. A Social Interaction Deviance Composite (SIDC) can be calculated to profile children as having socio-pragmatic difficulties or difficulties focused on language structure. The SIDC is calculated by subtracting the sum of scales A–D from the sum of scales E, H, I and J. The two non-language scales included in the SIDC ensure it is more sensitive to the discrimination of language difficulties in addition to social impairment characterizing ASD and language difficulties in the absence of social impairment (DLD). An SIDC value of greater than 9 suggests possible Developmental Language Disorder (DLD) and values below 0 are typical of individuals with ASD. Completion of the CCC-2 allows for the generation of age-normed standardized scores and clinical cut-offs based on UK population data. Internal reliability has been demonstrated to be appropriate across all subscales (.66–.80; Bishop, 2003) in typical populations, and the measure has been used successfully to measure language impairment in a sample of looked after children (McCool & Stevens, 2011).
Mental health
The Assessment Checklist for Children (ACC; Tarren-Sweeney, 2007) is a 120-item caregiver report of mental health difficulties in young people aged 4–11 in care or subject to adoption. The ACC has 10 subscales used to comprise an overall total clinical score, reported as a T-score. The subscales measure difficulties typically observed in LAACYP populations, such as anxious-distrustful, pseudomature and indiscriminate interpersonal behaviors and self-injury or suicide discourse. Respondents are asked to record on a 3-point scale the frequency of a range of behaviors and emotional states observed by them over the preceding 6 months. The measure has high rates of internal reliability for the clinical scales (α = .70–.86) and the total clinical score (α = .96) and high construct validity in comparison to similar measures used in non-LAAC populations (r = .89; Tarren-Sweeney, 2007).
Adverse childhood experiences
The Adverse Childhood Experiences Questionnaire (ACE; Felitti & Anda, 2003) is a 10-item measure designed to assess experience of childhood abuse, neglect, maltreatment and trauma. Each question in the measure has a yes or no response indicating the child’s experience of an adverse event. This allows for the generation of a total ACE score to indicate the extent of adverse childhood experiences. ACEs were initially designed to be implemented with adults, but they are also been found to be valid to measure short-term consequences of maltreatment in young people including LAACYP samples (Finkelhor et al., 2013; Rebbe et al., 2017; Turney & Wildeman, 2017).
LAACYP care-related factors
A short questionnaire was developed for the study to determine: (1) age at entry into care, (2) number of placements to which the young person has been subject, and (3) any previous involvement with health services, including speech and language services. The questionnaire was designed to be completed by each young person’s social worker using case-note information.
Design and procedure
Respondents were the child’s carer or adoptive parent (CCC-2 and ACC) and current social worker (ACE and LAACYP care factors). Caregivers were provided with written information packs and consent forms and contacted within 5 days to answer additional questions. Written consent was obtained from adoptive parents or carers and the child’s social worker prior to data collection. Assent was obtained from each young person at this time although they were not directly involved in completion of the measures. In the case of children in foster care, birth parents were also contacted by post to obtain informed consent. All participating young people in the sample were in the care of the study respondents for at least a 5-month period prior to data collection. Most caregivers who completed data for the study were female (M = 8, F = 39).
Data collection with carers/parents was undertaken either via telephone or in person, with an identical protocol followed in both instances. Caregivers completed the measures during a 30-minute appointment in the presence of a member of the research team. Each question was read out in turn and participants were asked to indicate their response, which was recorded by the researcher. All participants completed the CCC-2 measure, while participants reporting on young people between the ages of 4 and 11 also completed the ACC. Participants were then debriefed in full and encouraged to ask any questions if required. They were also offered the opportunity for an additional consultation with a relevant Trust professional if distressed or seeking further support following administration of measures.
Social workers were contacted via their secure trust email address and asked to complete the ACE questionnaire and demographic form and return via the same means.
Results
Language and communication difficulties
Prior to analysis, all UK age-normed subscale scores of the CCC-2 were rescaled to T-scores and the General Communication Composite (GCC) was also converted to a T-score. Most of the CCC-2 subscales did not approximate a normal distribution, with most being slightly positively skewed (toward poor performance), but two subscales (semantics and syntax) being slightly negatively skewed (toward normative population performance, see Figure 1(a)). Because a normal distribution could not be assumed, a permutation test of the one-sample t-test (two-tailed) was run with 5000 permutations using the implementation designed by Groppe (2020) where corrections for multiple comparison are made using the tmax method (Blair & Karniski, 1993).
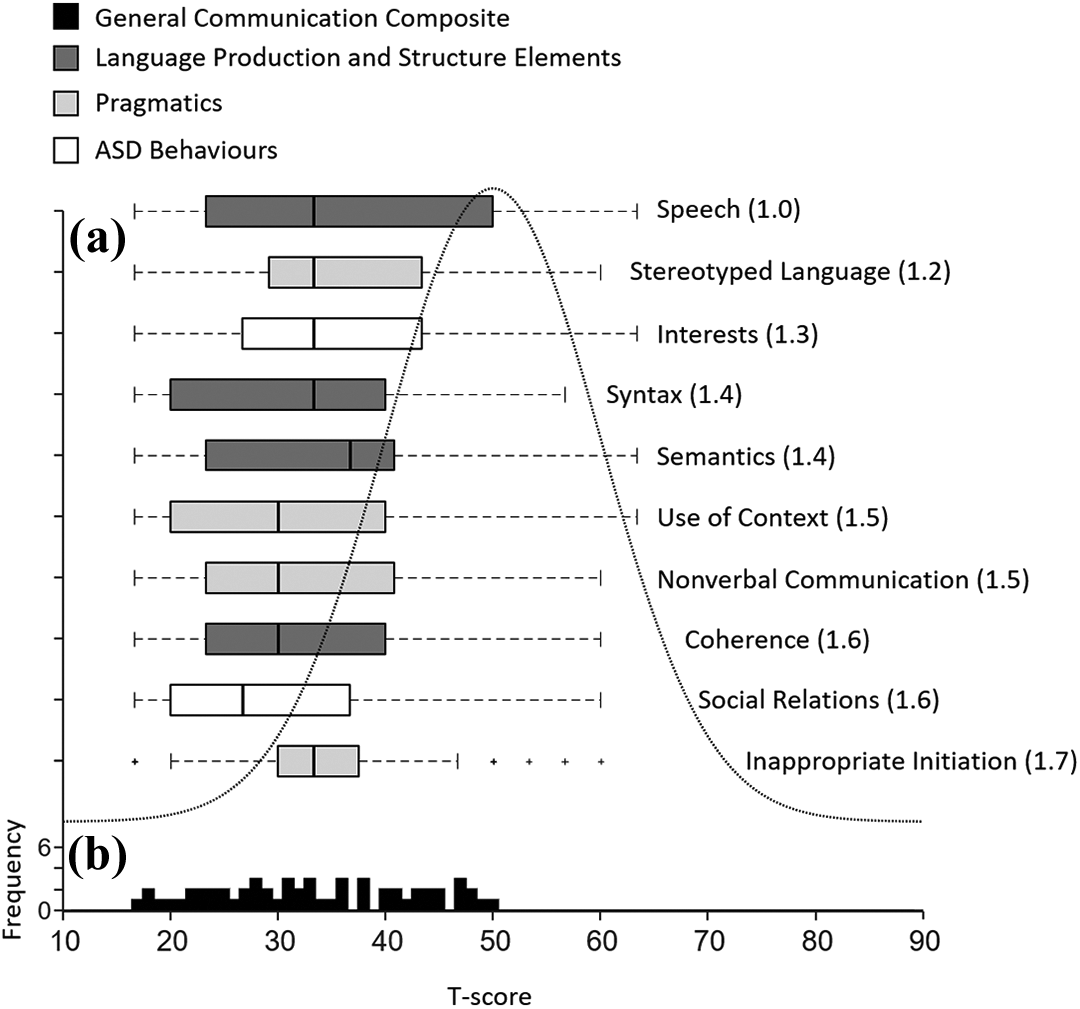
(a) Box plots of T-score distribution for CCC-2 subscales ordered according to the magnitude of the effect with the smallest difference from the UK norm at the top and largest at the bottom. Cohen’s d effect sizes are shown in parentheses. Plus sign markers identify cases >1.5 IQR from the median. A normal distribution based on the UK test norms is depicted by the dotted line. (b) Frequency of sample achieving each General Communication Composite T-score.
The LAACYP sample performed significantly below the population mean T-score of 50 on all CCC-2 subscales. T-score differences ranged from the smallest at −7.4 (speech) to −13 (inappropriate initiation) all p < .01 (see Figure 1(a)). The standardized effect sizes calculated (Cohen’s d) indicated that all subscale scores were between 1 and 2 SD below the UK population mean. It is worth noting that several outliers were identifiable for Inappropriate Intonation which may have erroneously inflated the effect-size for this subscale.
The effect sizes of the weaknesses in the subscales considered to measure pragmatics and those considered to measure language production and structure were similar as indicated by the very small spread of effect sizes (see Figure 1(a)). However, to test the hypothesis that LAACYP would show significantly weaker pragmatic ability than their ability with language production and structure, an a priori within subjects t-test (two-tailed) was conducted on the summed scores for the four pragmatics subscales and the four language production and structure subscales. The difference was small (m = .19, SD = 10.19) and not statistically significant (t[56] = .14, p = .89). For comparison with the wider literature GCC/SIDC cut-offs devised for the CCC-2 were used to quantify the number of LAACYP with characteristic DLD and ASD profiles. Of the 39 LAACYP who presented with an impaired language profile, 9 (23%) presented with a profile consistent with DLD and 14 (36%) presented with a profile consistent with ASD (see Figure 2).
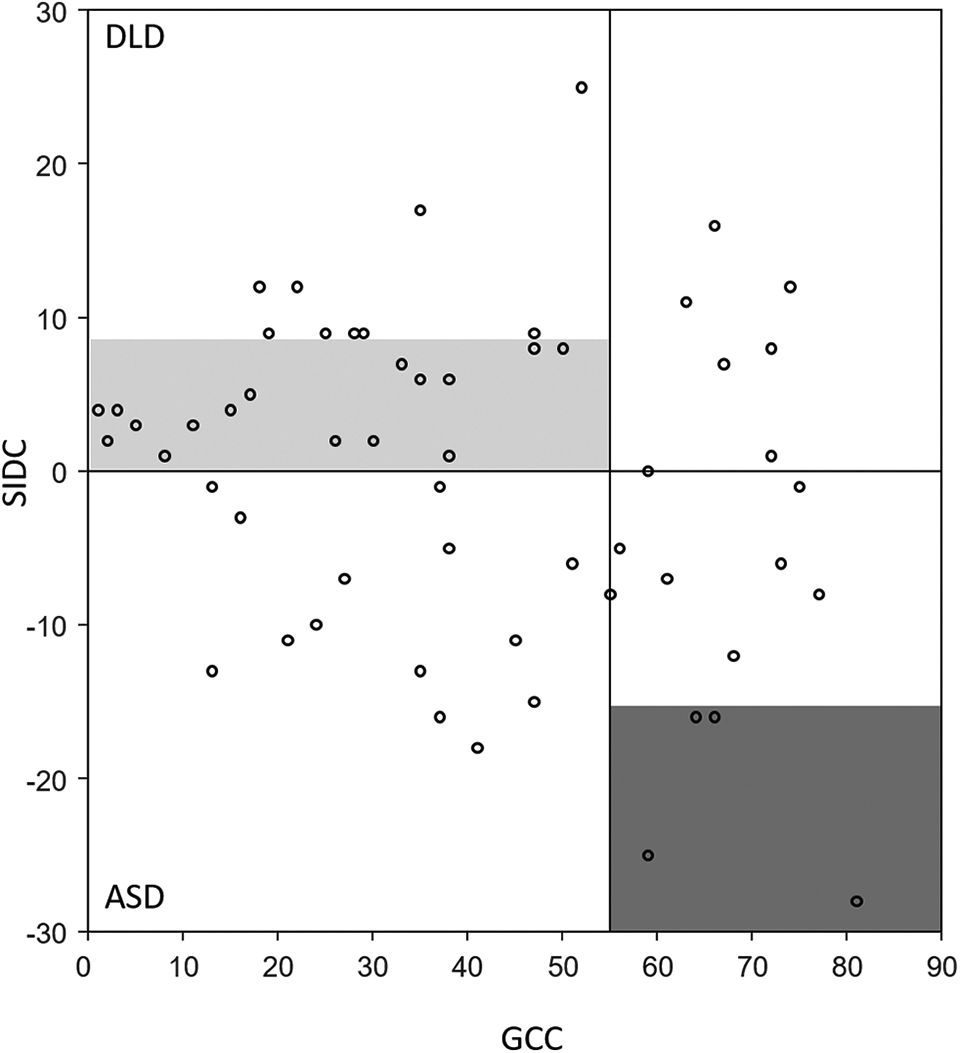
Scatter plot of individual GCC by SIDC scores identifying language and social-pragmatic profiles. GCC scores of less than 55 are indicative of language impairment. Combined with a negative SIDC value this is characteristic of an ASD like profile (bottom left quadrant), whereas combined with a positive SIDC value this is characteristic of DLD (top left quadrant). The light gray box identifies the quadrant where scores are considered to fall on the spectrum between DLD and ASD. The dark gray box identifies values which show substantial pragmatic and social difficulties relative to disproportionately good structural language skill, which is consistent with the profile of Asperger syndrome.
The CCC-2 composite scores (GCC) approximated a normal distribution with scores ranging from >3 SDs below the standardized test mean to within 1 SD of the standardized test mean (see Figure 1(b)). An a priori one-sample t-test was conducted to assess the sample’s composite score performance against the UK test norm for a population of the same ages. The sample performed significantly below the UK population norm at the time of testing. The GCC score was on average 1.7 SDs below the UK population norm (95% CI of between 1.4 and 1.9 SDs below the UK population norm). Using the CCC-2 clinical cut-offs, caregiver scores identified 68.42% of the young people’s language behaviors as being consistent with the lowest 10% of the normal population. Furthermore, the performance of over half of the sample (54.39%) was consistent with the lowest 3% of the normal population.
The current study hypothesized that more children in foster care would demonstrate a greater degree of language and communication difficulty than those with adoptive placements. This was explored by dividing the sample into four groups based on 1 SD intervals around and below the standardized test mean (see Figure 3(a)).
A Fisher’s Exact Test, with a bootstrapped confidence interval using 5000 bootstrapped samples, identified that the degree of language and communication difficulty differed by the type of placement (p < .01; 95% confidence interval ϕ = .29–.66). A higher proportion of the young people in foster care were reported to have a greater degree of language difficulty than those who were adopted. To confirm a difference in the severity of language difficulties between the two placement types, the young people in each placement type were compared using a permutation test of the independent sample t-test (two-tailed) with 5000 permutations. Since the between samples test is sensitive to differences in variability between samples, we confirmed the variability of scores for the young people in each placement type was remarkably similar using the robust coefficient of variation RCVQ described by Arachchige et al. (2020). RCVQ was 0.35 for those in foster care and 0.27 for those in an adoption placement. Nevertheless, Welch’s t statistic, which is more robust to samples of unequal sizes and variances, was used as a conservative estimate of the sample differences. It was found that young people in foster care had significantly more severe language and communication difficulty than those in an adoption placement (see Figure 3(b); t[55] = −3.03, p < .01).
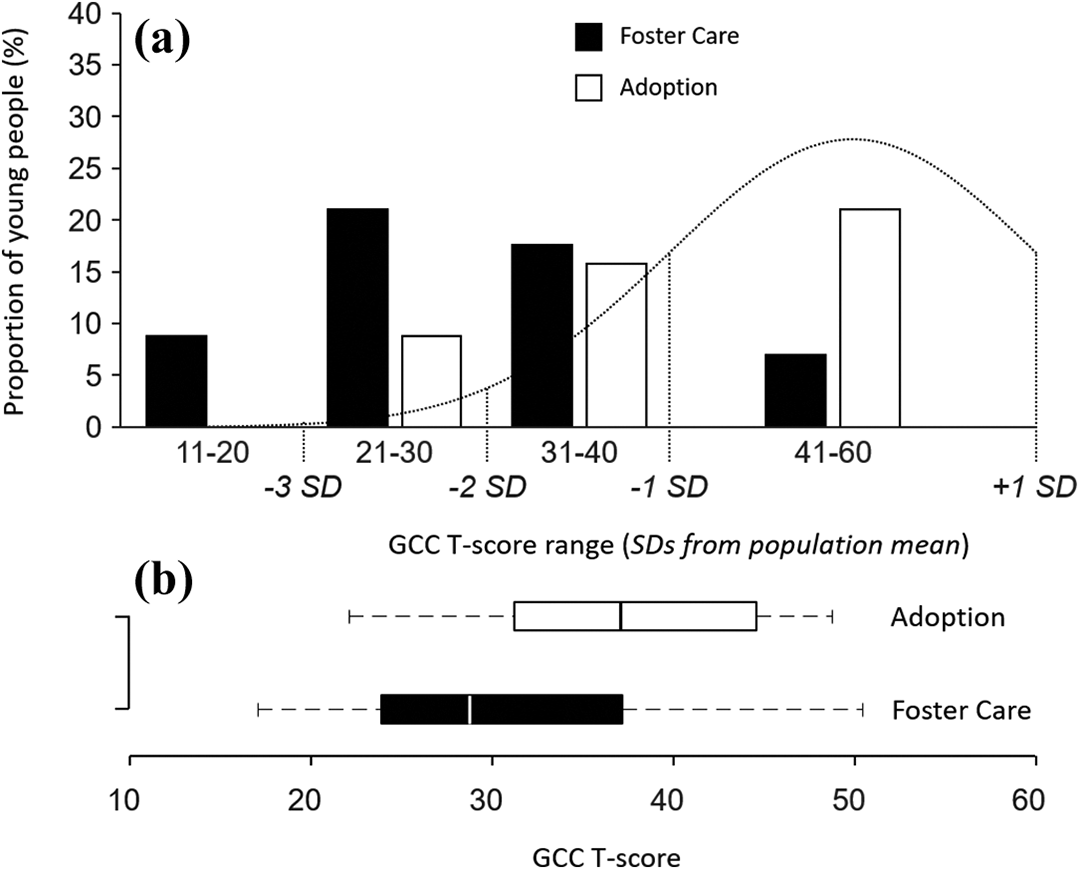
(a) Clustered bar chart demonstrating spread of GCC T-Scores in foster care and adoption subgroups, based on 1 SD intervals from the norm. Normal distribution curve also included based on UK population norms. (b) T-score distribution of GCC scores in foster care and adoption subgroups.
Association between care-related factors and language and communication difficulties
To test the hypothesis that language and communication difficulty would be associated with specific care-related factors, a series of non-parametric Spearman’s rank order correlations (two-tailed) were computed between individual GCC T-scores and each care-related factor, namely: age of young person, age of entry into care, number of placements, placement disruption computed as
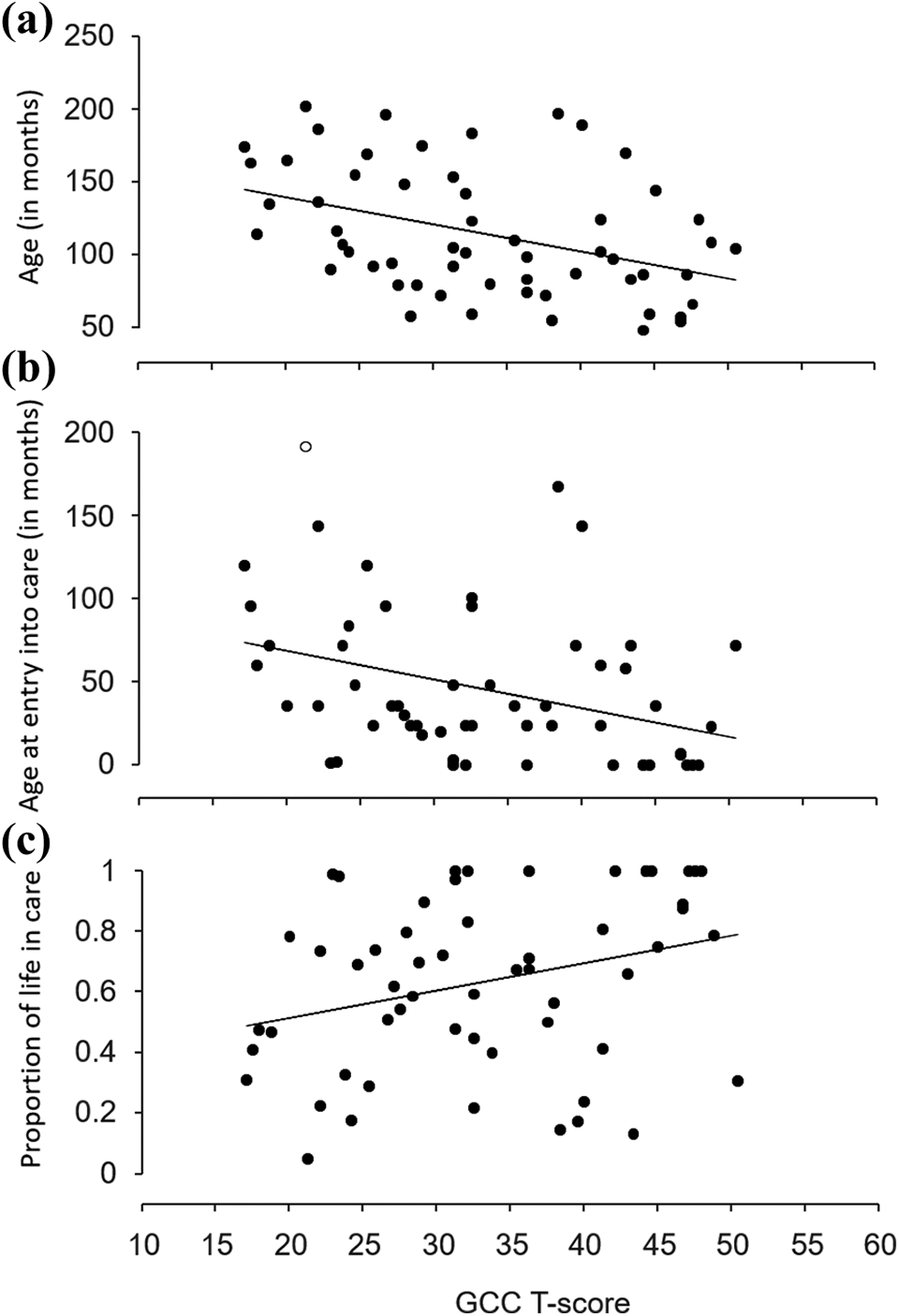
Scatterplot of association between individual GCC T-scores and (a) age of young person (months), (b) Age of entry into care (months), and (c) proportion of life in care. One participant entered care at 16 years old (identified by the unfilled circle), substantially outside the distribution of the other participants (>1.5 IQRs). The relationship remained when the data point was removed (rs = −.38, p < .01), with only a small reduction in explained variance of 2.1%.
Associations between language and communication ability and mental health were examined in the proportion of the sample who completed the ACC (n = 42) using a Pearson’s correlation (two-tailed) for normally distributed samples. A significant negative association was found (r = −.47, p < .01; see Figure 5).
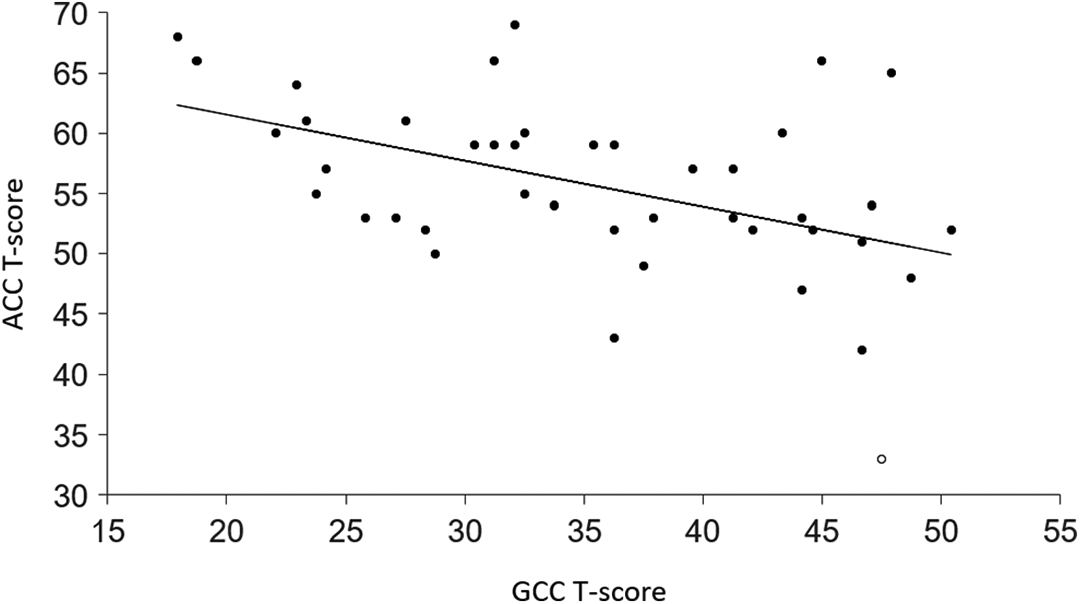
Scatterplot of association between individual GCC T-scores and individual ACC total clinical T-scores. One participant’s ACC total clinical T-score was substantially outside the distribution of the other participants identified by the unfilled circle (>1.5 IQRs). The relationship between variables remained when this data point was removed (r = −.44, p < .01), with a reduction in explained variance of 3.6%.
Impact of adverse childhood experiences on language and communication ability
A mediation analysis was conducted using the PROCESS V3 macro for SPSS (Hayes, 2018) to assess the influence of mental health on the relationship between ACEs and language difficulties in a LAACYP sample. The independent variable was ACE total Score, the dependent variable was GCC T-score and the mediator variable was ACC total clinical T-score.
In step 1 of the mediation model, the regression of ACE Total Score on GCC T-score, ignoring the mediator, was non-significant (see Figure 6; t(42) = 1.50, p = .14). Step 2 demonstrated that the relationship between ACE total score and the mediator (ACC total clinical T-Score) was significant (t[42] = 3.19, p < .01). Step 3 demonstrated that ACC total clinical T-score, controlling for ACE total score, had a significant relationship with GCC T-score (t[42] = −2.94, p < .006). Step 4 reported that there was no significant relationship between ACE total score and GCC T-score when controlling for ACC total clinical T-score (t[42] = −.14, p = .89).
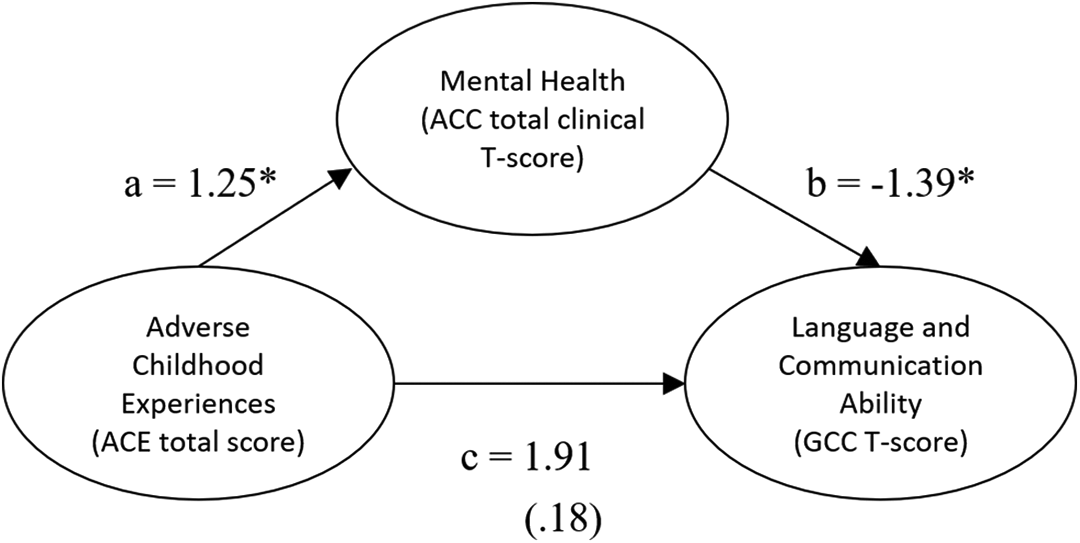
Standardized regression coefficients for the relationship between ACE total score and GCC T-score, as mediated by ACC total clinical T-score. Standardized regression coefficients are reported between (a) ACE total score and ACC total clinical T-score, (b) ACC total clinical T-score and GCC T-score, and (c) ACE total score and GCC T-score. The standardized regression coefficient between ACE total score and GCC T = score, controlling for ACC total clinical T-score, is in parentheses. The asterisk identifies significant predictions at p < .01.
Discussion
Language and communication difficulties
A high proportion (68%) of the LAACYP sample demonstrated language and communication difficulties consistent with the lowest 10% of the general population. Only 14% of the sample had previous or current involvement with speech and language services. These findings are highly comparable with McCool and Stevens (2011), who reported that 63% of 30 children in care performed at similar levels, as measured by the CCC-2, with none previously receiving speech and language intervention. These findings suggest speech and language needs often appear to be either unidentified or not prioritized when evaluating the needs of individual LAACYP (Snow, 2009).
In the current study difficulties were found across all CCC-2 subscales, suggesting notable difficulties in language production and comprehension including vocabulary, discourse and pragmatics. The CCC-2 enables the assessment of language performance in everyday settings, which is particularly important for the characterization of pragmatics. Previous research has shown the CCC-2 to be a preferable measure of pragmatics in comparison to similar psychometric tools (Volden & Phillips, 2010). However, objective measures of language ability other than pragmatics are often better quantified in further assessments (Adams, 2015). Although the CCC-2 is standardized for use by carers, many foster carers and adoptive parents specifically receive training in child development, attachment and therapeutic parenting practices. These carers therefore may be particularly sensitive to identifying additional needs in their young person.
Interestingly, the LAACYP population had CCC-2 subscale scores on average more than 1 SD below UK norms for similarly aged children indicating more significant levels of difficulty than suggested by Lum et al.’s. (2015) meta-analytic study in relation to maltreated children (1 SD expressive and .5 receptive below the average for non-maltreated children). This suggests there may be additional care-related factors impacting the language difficulties experienced by LAACYP, not just those linked to maltreatment.
No significant differences were established between structural and pragmatic aspects of language. The adverse experiences typically experienced by children in care appear to have had a global effect on language rather than a differential impact on pragmatics as hypothesized. McCool and Stevens (2011), the closest comparable study, did not report individual subscale scores, but using the SIDC they did report that 8 of 19 (42%) LAACYP with demonstrable language and communication impairment had clinical profiles consistent with ASD (consistent with pragmatic difficulties). A similar proportion of 36% presented with clinical profiles consistent with ASD in the current study. Using the individual CCC-2 subscales the results of the current study suggest that, as a group, the LAACYP sample had a profile indicative of language and communication needs. However, consistent with McCool and Stevens (2011) the LAACYP sample was formed from participants across the continuum of socio-pragmatic function. There is clear heterogeneity with some individuals displaying scores consistent with language difficulties and a comorbid socio-communicative disorder, and others without. Importantly, the number of individuals with an ASD profile is in excess of the three participants with diagnosed ASD where pragmatics would typically be expected to be poorer than structural language ability (Geurts & Embrechts, 2008).
Association between care-related factors and language and communication difficulties
Overall language ability was negatively associated with age of the young person. Children in the sample tend to fall further behind their age-matched peers as they enter adolescence. Prior studies have demonstrated that early language difficulties often persist or increase in adolescence (Conti-Ramsden & Botting, 2008). The additional pressure on communication makes social interaction stressful thus making these children increasingly susceptible to mental health difficulties (Cohen et al., 2013; Wadman et al., 2011).
Age of entry into care was significantly associated with language and communication difficulty, with later entry associated with greater difficulty. This mirrors other findings in the literature (e.g. Lum et al., 2018; Windsor et al., 2011). It is an obvious interpretation that the greater length of time spent by a child in circumstances not adequately nurturing and stimulating, the more likely there will be negative impacts on development. Removing a child into care is one of the potential interventions for this, as is providing adequate supports and interventions for families in the community. It is also interesting to consider how in some cases, the impacts of undetected developmental difficulties may have contributed to the burdens experienced by vulnerable families, emphasizing the importance of early detection and intervention, particularly for families with high levels of need.
Children in foster care were found to perform significantly below those who had been adopted, a finding that requires exploration. Achieving a permanent home with responsive, nurturing parents or carers as early as possible is likely to be associated with better outcomes. Adoption can be a route to early permanence and increased parental responsiveness, both of which have been shown to positively impact language development in adopted children (Stams et al., 2002).
Interestingly, we did not detect a significant relationship between language ability and the number for placements or placement disruptions. Although placement disruption is considered a risk factor in psychiatric symptomatology in young people in care (e.g. McGuire et al., 2018), an association has not been demonstrated with individual language ability. More frequent changes in placement represent repeated disruption in attachment relationships and compromise a child’s opportunities to form meaningful bonds that may help mitigate early delays. It may be in the current study that the spread of the number of placements was insufficient or that the impact of placement stability is not linear, with high placement instability having a large impact on language ability, but low instability having less impact.
Impact of adverse childhood experiences and mental health on language and communication ability
A significant relationship was established between mental health difficulty and language and communication impairment. Mental health difficulty explained 22.5% of variance in language and communication scores in the sample and thus appears to be a risk factor for communication impairment in the LAAC population. LAACYP are at greater risk of experiencing mental health difficulties than the general population. Co-occurring language and communication difficulties may exacerbate mental health problems by: (1) reducing the ability to regulate affect by limiting understanding and differentiation of emotions based on physiological sensations, external cues and categorical knowledge (Lindquist et al., 2015); (2) reducing the effective expression of emotion in a healthy and constructive manner (Monopoli & Kingston, 2012); (3) limiting access to protective factors such as positive peer relationships and academic success (Toppelberg, 2014).
The current study found no significant relationship between ACEs and language and communication needs, and as a result no significant mediation effect was established. It was hypothesized, based on prior research, that exposure to ACEs would have a cumulative impact on development (DeJong et al., 2016). Past research has indicated that these risk factors have been reliably and linearly associated with child psychiatric symptomatology (Raviv et al., 2010). Pears and Fisher (2005) reported that quantity of adverse experiences was positively associated with language ability in 2–6 year-old children in care. It is possible that LAACYP experience a threshold effect in ACEs, like that argued by Morales and Guerra (2006), wherein ACEs have a significant impact up to a certain point, then plateau with subsequent adverse experiences not contributing further. Consistent with this proposal, Horan and Widom (2014) found ACEs to have a curvilinear relationship with educational attainment. One or two risk factors led to an exponential decrease in functioning, with less differentiation reported as ACEs increased beyond this threshold. While it is possible that there is a curvilinear relationship between cumulative risk and language impairment, it may also be the case that ACEs are insufficiently sensitive to discern significant differences between these young people. Tarren-Sweeney (2008) previously found that length of exposure to maltreatment was a more significant influence on outcomes than cumulative maltreatment types. Assessment of the impact of trauma in LAACYP may require a tool which accounts for length and magnitude of exposure to trauma rather than cumulative adverse experiences.
An alternative explanation of the lack of relationship between ACEs and language and communication impairment may be that protective factors brought about by the care experience (e.g. supportive and attuned caregivers, access to healthcare and community supports) or factors associated with resiliency (e.g. positive coping skills, higher IQ) buffer the impact on language and communication. Previous research has found that protective factors moderate the relationship between adversity and trauma symptoms in maltreated children (Racine et al., 2020).
Study limitations and clinical implications
This measurement of language ability and mental health relied solely on carer-report checklists. The rationale for this approach was to reduce the burden on LAACYP. Adequately measuring mental health in LAACYP requires posing questions on sensitive topics such as sexualized behaviors and suicidal ideation that may be very distressing for vulnerable young people, so the use of a carer-report is often more appropriate. In contrast, language structure is arguably most reliably measured using conventional diagnostic instruments which objectively probe language production and comprehension. Conventional tests of pragmatics typically use hypothetical situations to test pragmatic ability (e.g. Test of Pragmatic Language 2nd Edition; TOPL-2; Phelps-Terasaki & Phelps-Gunn, 2007). These tests typically fail to quantify the application of pragmatics in conversation, which may be distinct from the ability to respond to hypothetical situations (i.e. knowing how to respond is not the same as typically responding that way; Schoen Simmons et al., 2014). In contrast, the checklist of the CCC-2 uses questions of the frequency of language behaviors observed by an individual who is in regular contact with the young person being assessed. However, it has already been found that CCC-2 pragmatics subscales were differentially scored by parents to give lower scores in pragmatics than suggested by the child’s clinical profile and teacher’s rating (Bishop, 2003). It is currently unknown if there is a similar differential impact of parents/carers of LAACYP. It is possible that because parents/carers are heavily invested in gaining support for their LAACYP, they may tend to report elevated levels of difficulty. Equally, since these parents/carers are given specific training in child development, attachment and therapeutic parenting practices, atypical behaviors may be more recognizable to them than to typical birth parents. The addition of tasks that use probing activities to illicit socio-pragmatic behaviors and communication during clinical observation in future studies will enable evaluation of parent/carer bias on the ratings (see for example the Pragmatic Activity Checklist of the CELF-5; Semel, Wiig, Secord, 2013).
One strength of this study is that it assessed the impact on a wide age range of children with varying ages of entry into care, allowing for the evaluation of general trends in a relatively heterogenous group. However, this also limited some of the conclusions of the study. Specifically, developmental trends in the impact of socio-pragmatic impairments could not be considered within this sample. Larger studies where covariation in age of entry into care can be controlled within age subgroups will be essential in the future.
The results of this study indicate that LAACYP demonstrate significant language and communication impairments in comparison to what is expected of other children their age. These impairments remain under-recognized within care-giving systems as most recently highlighted by Cross (2018). The current study again highlights the need to become attuned to language and communication difficulties as an important aspect of trauma-informed care delivery. This includes ensuring that Speech and Language Therapy Services are adequately represented within the multidisciplinary response to these young people, that therapeutic formulations are adequately informed by assessment of speech and language need—as well as other neurodevelopmental presentations—and that a range of creative psychological therapies which do not require language as the main mode of communication are available as part of therapeutic provision for LAACYP.
Conclusion and future directions
Language difficulties in the LAACYP population are frequent and can be severe, impacting on all aspects of language and communication ability. The extent of language and communication impairment in this population requires greater attention given the social, psychological and functional implications of language delay (e.g. Maggio et al., 2014; Stock & Fisher, 2006). Further research should explore how verbal reasoning may be impacted by the language difficulties experienced in this population. Many challenges require verbal reasoning via internal or external dialogue in order to problem-solve effectively and these in turn have a self-regulatory function (Snow, 2009). One recent study found that 4–7 year-old children with DLD performed significantly worse on a planning task than their typically developing peers, impaired children being up to 2 years behind their peers at this early stage of development (Abdul Aziz et al., 2017). Similar findings have been found for 7–11 year-old children (Lidstone et al., 2012).
The impact of language impairments on the effectiveness of emotional and behavioral interventions for LAACYP also requires investigation since interventions often rely heavily on language and dialogue with adults, intervention for the observed language difficulties may be necessary to supporting treatment of mental health difficulties. Future studies that examine treatment effectiveness for LAACYP and its relationship to the nature of language impairment from predominantly structural to predominately socio-pragmatic difficulties are also required.
Importantly, future research should assess for differential developmental trends in socio-cognitive and structural language impairments on mental health and vice versa. Some evidence suggests that socio-pragmatic impairments have specifically severe impact during adolescence and adulthood, for example on reduced peer relationships (St Clair et al., 2011; Whitehouse et al., 2009). Whereas structural language difficulties may have the greatest impact during early childhood. For example, while 2-year-olds with expressive language delay (a group often referred to as late talkers) tend to have more behavioral problems than their typically developing counterparts, there is no relationship between late talking and behavioral problems from 5 to 17 years old (Whitehouse et al., 2011). Longitudinal studies with LAACYP will be most effective in elucidating the causal direction of the relationship between mental health and language difficulties, and specifically the potential differences in the causal relationship between structural and socio-pragmatic difficulties and mental health.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.