
Abstract
Background:
Cardiovascular disease increases the risk for cerebrovascular disease (CBVD) and cognitive decline. The retina has become an ideal target for imaging cerebrovascular changes via optical coherence tomography angiography (OCTA). Whether OCTA metrics map onto clinical outcomes in adults at high risk for CBVD and cognitive decline remains unknown.
Objectives:
This study examined the relationship between OCTA metrics and domain-specific cognition in older adults recently discharged from a 12-week cardiac rehabilitation program, who are at high risk of both CBVD and cognitive decline.
Design:
This was a prospective, feasibility/pilot study to determine whether OCTA metrics are related to cognition in this unique population of high-risk adults.
Methods:
Twenty-two older adults recruited within 3 months of completing a 12-week cardiac rehabilitation program participated in a single visit consisting of cognitive assessment and OCTA imaging. Cardiac/exercise metrics were compared pre- and post-rehabilitation. Primary outcomes were analyzed using partial correlation, and multiple regression assessed whether exercise moderates the relationship between retinal vasculature and cognition.
Results:
Higher performance in episodic memory predicted retinal vascular perfusion. Change in time spent performing exercise and change in systolic blood pressure from pre- to post-cardiac rehabilitation were associated with higher logical memory performance post-rehab. Exercise did not moderate the relationship between retinal vascular perfusion and cognition.
Conclusion:
The results of this study support a direct relationship between retinal vascular integrity and cognition in those at high risk for cognitive impairment and cardiovascular disease (CVD). Future research in larger samples with data collection both pre- and post-cardiac rehabilitation will inform whether this relationship is mediated by exercise.
Introduction
Cardiovascular disease (CVD) is a risk factor for cerebrovascular disease (CBVD), cognitive decline, and Alzheimer’s disease (AD). 1 Modification of CVD risk factors reduces rates of CBVD and AD. 2 Cardiac rehabilitation programs, prescribed after cardiac events, effectively improve both cardiac metrics (i.e., cardiorespiratory fitness, blood pressure, and weight) and cognition in older adults. 3 Meta-analysis shows that moderate exercise improves both global and domain specific (e.g., executive function and working memory) cognition in various age groups, who are otherwise healthy or have a clinical diagnosis (e.g., CVD, CBVD, mild cognitive impairment (MCI), and AD).4,5 One review highlighted several studies demonstrating that acute and chronic exercise-induced effects on the cerebrovascular system, as measured through retinal vessel density, are correlated with improved cognitive performance. 6 For example, incorporating physical exercise breaks during periods of prolonged sitting resulted in improvements to executive functioning and retinal vessel density in college students. 7
Current biomarkers for monitoring vasculopathy in CBVD and AD, such as magnetic resonance imaging are costly and require specialized equipment and staff. In this study, we examine the feasibility of using the retina, an extension of the central nervous system that shares embryological origin, neurovascular composition, and neurobiology with the cerebral cortex, as a minimally invasive, cost-efficient, and accessible biomarker of cerebral vasculature and cognition in older adults recently discharged from cardiac rehabilitation, a population that is highly vulnerable to cognitive decline. The cardiac rehabilitation program represents an intervention that could help mitigate the risk of repeated cardiac incidents and cognitive decline.
Here, we examined the relationship between retinal vasculature and cognition in a group of older adults vulnerable to persistent CVD and cognitive decline within 3 months of completion of a 12-week cardiac rehabilitation program. In addition, we examined exercise changes from pre- to post-rehabilitation as a potential moderator of this relationship. Retinal vascular changes occur in CBVD, MCI, and AD, related to the level of cognitive impairment. 8 Data shows that a 12-week exercise intervention improved the integrity of retinal microvasculature in older adults, 9 and that myogenic vasoconstriction may be reduced in response to exhaustive exercise and reflect age-related loss of vascular reactivity in older adults. 10 We hypothesize that retinal vascular metrics and domain-specific cognition will be related in older adults recently discharged from cardiac rehabilitation, and that exercise will moderate this relationship in older adults recently discharged from 12-week cardiac rehabilitation. We also hypothesize that both cardiac rehabilitation metrics and exercise metrics will show a positive association with domain-specific cognition in this population.
Methods
Participants
Twenty-two participants (44 eyes; 5 female (F), 17 male (M), mean age = 63, SD = 8) were recruited within 3 months of completion of cardiac rehabilitation at the Miriam Hospital Cardiac Rehabilitation Center. 20 participants were White (90.9%), one participant was African American, and another participant preferred not to include their ethnicity. Inclusion/exclusion criteria can be seen in Table 1.
Inclusion and exclusion criteria.

Procedure
All participants were seen at a single visit at the Lifespan Clinical Research Center within 3 months of completion of cardiac rehabilitation. All participants had the decisional capacity to provide written informed consent independently (see Table 1, inclusion criteria). All participants completed neuropsychological assessment and retinal OCTA imaging using the Heidelberg SPECTRALIS 2. Outcome measures can be seen in Table 2.
Outcome measures for cognition, cardiac rehabilitation, exercise, and retinal vasculature.

BMI, body mass index; DCTclock, Digital Clock Drawing Test; DSST, Digit-Symbol Substitution Test; EMR, Electronic medical record; FAS, F-A-S Verbal Fluency Test; FAZ, foveal avascular zone; ISLT, Cogstate International Shopping List Test total score; OCTA, Optical coherence tomography angiography.
Cardiac rehabilitation program
All participants completed cardiac rehabilitation for one of the following reasons: myocardial infarction, congestive heart failure, heart valve repair/replacement, heart transplant surgery, and heart bypass surgery. The cardiac rehabilitation program consisted of 3 × 90-min sessions (60-min exercise and 30-min education, counseling, and behavior modification) per week for 12 weeks. 11 Patients completed a baseline exercise maximum stress test to assess current cardiorespiratory fitness as well as psychosocial outcomes using PHQ-9 12 (depression symptoms), GAD-7 13 (for anxiety), and SF36 14 (for physical and psychosocial function). Based on the results of the exercise stress test, patients were prescribed aerobic exercise in the first 4 weeks, after which resistance training started, with gradual increases in both aerobic and resistance workload based on the rate of perceived exertion and heart rate, and the workload achieved during the baseline exercise stress test. All baseline tests were repeated at program completion to assess for change and generate exercise prescriptions for discharge.
OCTA image acquisition
OCTA was used for imaging retinal vasculature. All images were acquired on the Heidelberg SPECTRALIS® OCT Plus with BluePeak™ and processed using Eye Explorer (HEYEX) version 1.10.4.0. Our OCTA imaging protocol has been published previously. 15 Briefly, prior to imaging, all participants were dilated with two drops of tropicamide (Mydriacyl 1%) per eye. We obtained 20 × 20° OCTA images consisting of 512 B-scans, 512 A-scans per B-scan, 12 μm spacing between the B-scans, and 5 frames averaged per B-scan location of the central fovea.16,17 The signal quality values (range for SPECTRALIS = 0–40) from the vendor software were at least 30 to ensure good image quality. All scans were visually inspected for motion and shadowing artifacts. To increase our sample size, both eyes from participants were selected for the purpose of image analysis. Processing methods for OCTA images have been published previously. 17 For a full description, see Supplemental File 1. Key outcomes include the foveal avascular zone (FAZ) area, FAZ diameter, and vessel density.
Cognitive testing
Neuropsychological tests administered included the Cogstate International Shopping List Test (ISL, with delayed recall) 18 and Wechsler Memory Scale Logical Memory Test (WMSLM; WMS-III) 19 for episodic memory, the FAS Verbal Fluency Test 20 for language, the Digit-Symbol Substitution Test (DSST) 21 and the DCTclock Test 22 for executive function, attention, visuospatial construction, and processing speed.
Cardiac rehabilitation and exercise metrics
Vital signs, including height, weight, blood pressure, and heart rate were collected through chart review from baseline and final cardiac rehabilitation visits. In rehab, blood pressure was measured twice, 15 min apart, while the participant was seated in a quiet room. Demographic information, including date of birth, sex, relevant medical history (including cardiac, neurological, and psychiatric history), and family history, was collected through chart review. Self-reported number of minutes of moderate or vigorous exercise per week in the last 30 days, as well as workload achieved at the time of cardiac rehab completion (based on the highest workload achieved in the last week of the rehab sessions and graduation exercise testing performance), were also collected. Change scores for max metabolic equivalents (METs), exercise minutes per day, exercise minutes per week, and exercise days per week were calculated according to the following equation:

Statistical analysis
Analyses were completed using RStudio software for Windows (version 4.3.1). A paired-sample t-test determined whether cardiac rehab metrics differed significantly within subjects, pre- and post-rehab. Partial correlations controlling for age determined the relationship between retinal vasculature metrics and cognition, cognition, exercise, and cognition and cardiac rehabilitation outcomes (see Table 1 for outcome measures by category). We also examined the relationship between exercise change pre- to post-rehab and retinal vasculature, as previous studies have shown improvements in retinal vascular health with exercise. Missing data was accounted for using casewise deletion. Following partial correlation analysis, multiple regressions (with age as a covariate) were used to examine whether exercise was a moderator of the relationship between retinal metrics and cognitive function for previous significant partial correlations. For each of the relevant cognitive outcomes, three exercise measures were tested as moderators: exercise minutes per day, minutes per week, and days per week. These metrics included both regular exercise at cardiac rehabilitation and prescribed exercise outside of cardiac rehabilitation.
Results
Cardiac and exercise changes pre- and post-rehabilitation
Results from paired t-tests showed a statistically significant increase in total exercise workload (METs) and duration at the end of cardiac rehabilitation compared to pre-cardiac rehabilitation (p < 0.001). Participants’ weight (kg) also significantly decreased after completing cardiac rehab. Other cardiac metrics collected did not change significantly from pre- to post-rehab.
Primary outcome: Cognition and retinal vascular metrics
Table 3 shows associations between retinal vascular metrics and cognitive testing within 3 months of completion of cardiac rehabilitation. Notably, significant positive linear relationships were demonstrated between performance on the ISL trial 1 and ISL delayed recall with FAZ area and effective diameter (see Figure 1(a)).
Pearson’s partial correlation coefficients (controlling for age).
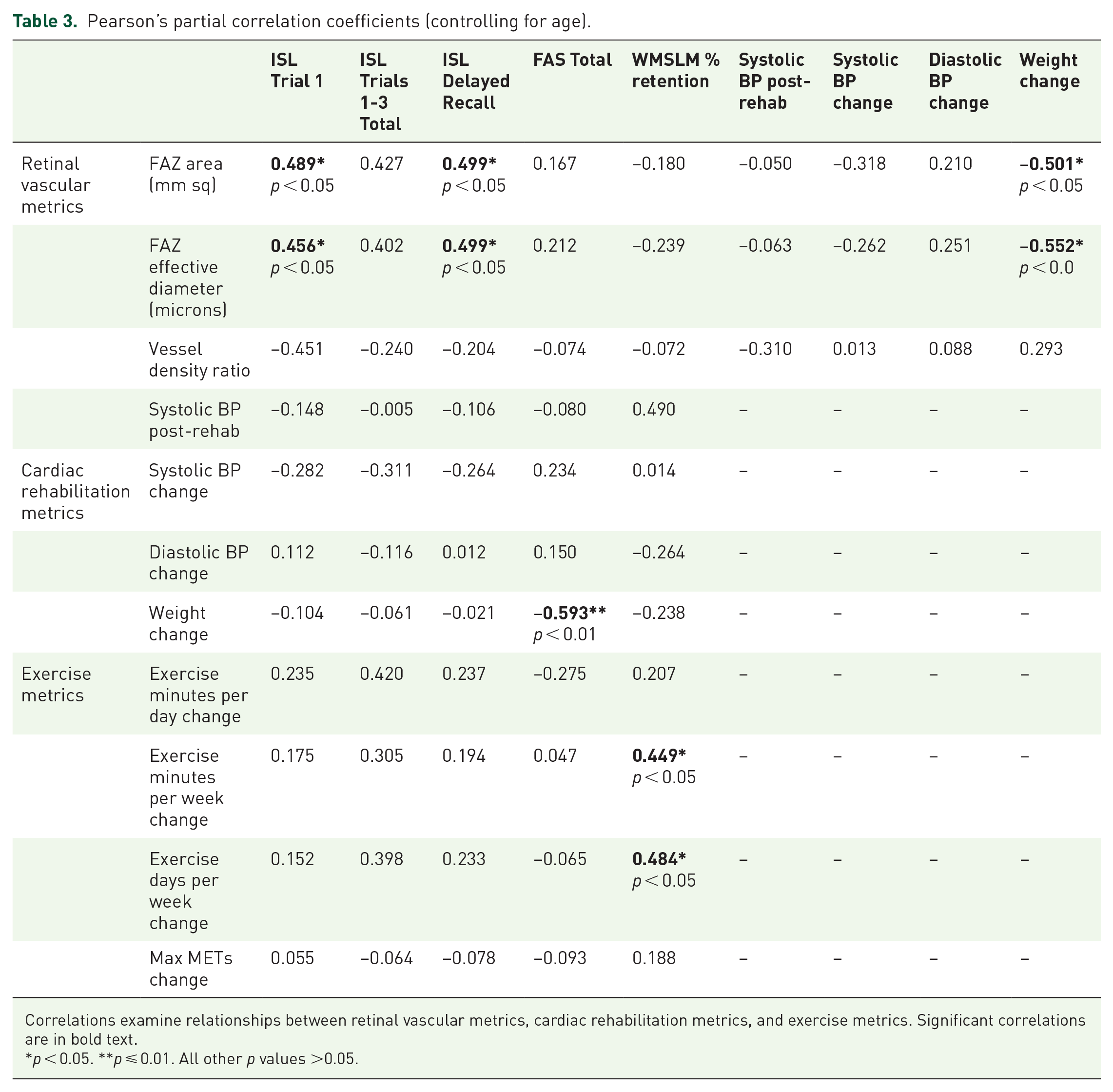
Correlations examine relationships between retinal vascular metrics, cardiac rehabilitation metrics, and exercise metrics. Significant correlations are in bold text.
p < 0.05. **p ⩽ 0.01. All other p values >0.05.
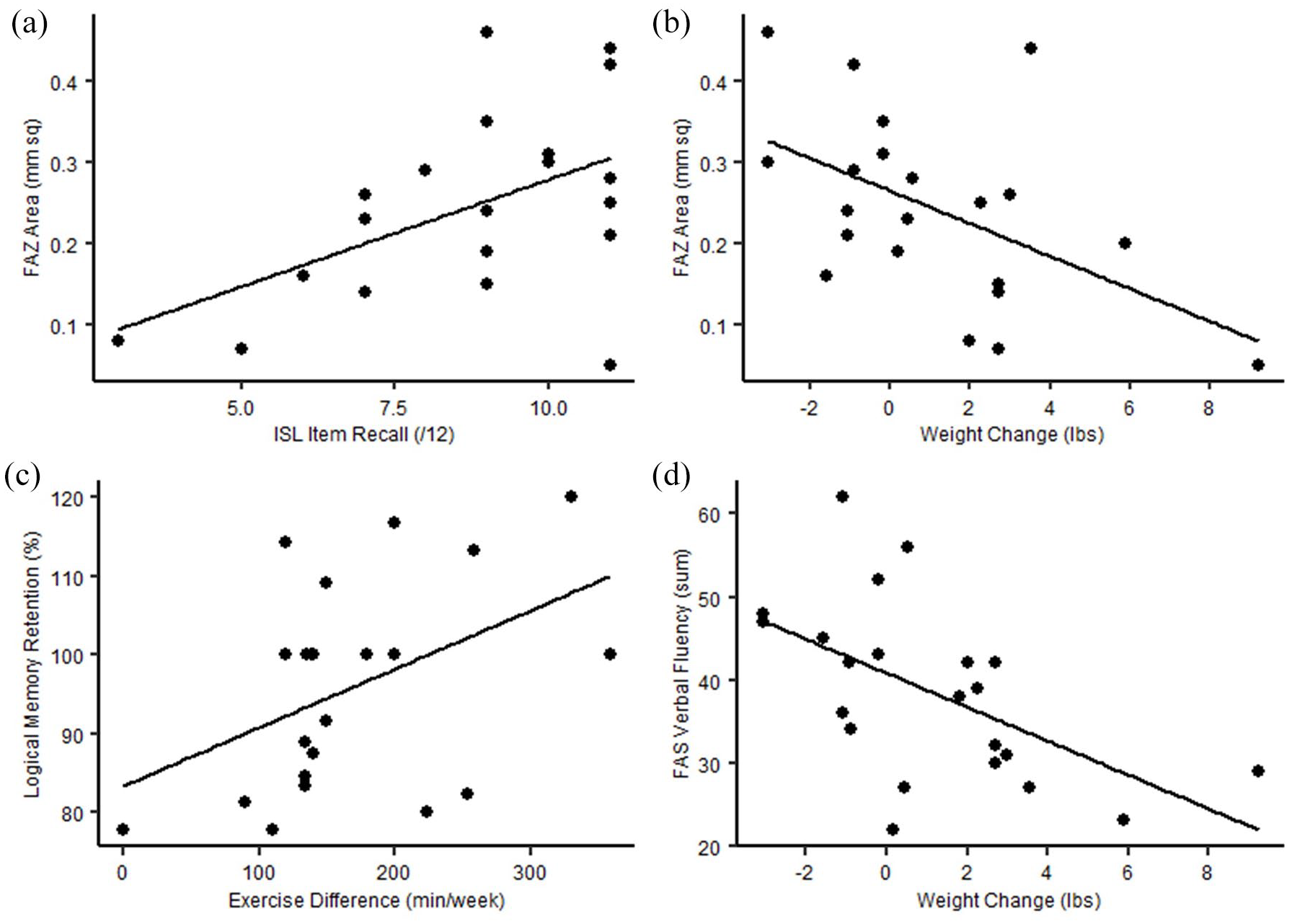
Scatterplots showing significant associations between ISL Item Recall and FAZ Area (a), weight change and FAZ area (b), exercise difference and logical memory percent retention (c), and weight change and FAS verbal fluency sum (d). Dark lines represent lines of best fit.
Exercise as a moderator of the relationship between retinal vascular metrics and cognition
Given the linear relationships demonstrated in Figure 1, multiple regressions were run to examine whether exercise metrics (minutes per day change, days per week change, and minutes per week change) moderate the relationship between retinal metrics and cognition. While the FAZ area significantly predicted ISL delayed recall (adjusted R2 = 0.27, F(6, 13) = 2.175, p < 0.05), exercise metrics did not moderate the relationship between FAZ area and performance on the ISL, FAS, or WMSLM tests (all p > 0.05; see Supplemental Table 1).
Secondary outcome: Cognition and cardiac metrics
As seen in Table 3, participants who lost more weight from pre- to post-rehab had better scores on the FAS, a measure of verbal fluency (see Figure 1(b)).
Secondary outcome: Cognition and exercise metrics
Better episodic memory retention on the WMLSM was associated with adding more exercise pre- to post-rehab in minutes per week and days per week (see Figure 1(c)). There was a trend-level correlation between ISL total learning with exercise change in minutes per day and days per week (see Table 3).
Retinal vasculature and cardiac rehabilitation anthropometrics
As weight loss pre- to post-rehab increased, both FAZ area and FAZ effective diameter decreased, indicating improvements in retinal vascular health associated with weight loss pre- to post-rehab (see Table 3).
Discussion
The retina has emerged as an ideal target for understanding pathological vascular dysfunction in the brain. 15 Previous literature demonstrates structural and microvascular changes in the retina of cognitively unimpaired older adults, CBVD patients, as well as MCI/AD patients.1,15,23 This study demonstrates the feasibility of using retinal vascular health, specifically FAZ area and diameter, and episodic memory as biomarkers in those with CVD at high risk for cognitive decline. To our knowledge, this is the first to examine the relationship between retinal vascular health and domain-specific cognition in this population.
Our results show better episodic memory performance was associated with a measure of oxygen metabolism (FAZ area) and retinal vascular health, as well as increased exercise frequency and duration over the 12-week cardiac rehabilitation period. Verbal fluency scores improved with increased weight loss over the 12-week cardiac rehabilitation period, and increased weight loss was associated with improved retinal vascular health. Decreased FAZ area suggested improved episodic memory performance post-rehab. However, exercise did not moderate this relationship.
Enlargement of the FAZ represents progressive capillary non-perfusion and has long been considered a clinical indicator of progressive retinopathy in the context of diabetes and other cardiometabolic changes. Increased FAZ area could indicate particular vulnerability to cerebrovascular and downstream cognitive changes in older adults with a history of major cardiac events.
It is well established that aerobic training improves performance on global 22 and domain-specific24,25 cognition in cognitively unimpaired older adults, MCI/AD patients, and CVD patients. 26 Our findings extend this literature by supporting the relationship between cognition and a) cardiac health and b) exercise in older adults with a recent history of cardiac events and providing feasibility data for the relationship between OCTA metrics and cognition in a group of older adults at high risk for pathologic and cognitive decline.
We expected that exercise may serve as a moderator of the relationship between cognition and retinal vascular health, given its established positive effects on both; however, we did not find any evidence of moderation. This could be due to limited sample size or differences in the sensitivity of our cognitive assessments to subtle changes of cognition in disease pathogenesis (i.e., our common neuropsychological assessments for dementia vs more sensitive standardized cognitive batteries). 27 Employing more objective operationalizations of exercise (such as a FitBit or actigraphy watch) may lead to improvements in construct validity for obtaining exercise data.
Our sample and data collection were limited by several factors, including a lack of demographic data obtained, the disproportionate number of males compared to females, and a small sample size (N = 22, N = 44 eyes), which may limit statistical power. No power analysis was conducted a priori, as we wanted to demonstrate the feasibility of the approach and collected data from a convenience sample. Future work should examine larger samples of individuals who have experienced significant cardiac events both pre- and post-rehab to assess how relationships between retinal vascular health and general/domain-specific cognition over time in this population. In addition, cognition could have been differentially affected by different cardiac events. Due to the small sample size, we elected not to perform a subanalysis, but future studies should investigate the differential cognitive outcomes of cardiac incidents. Similarly, we did not perform a sex-based subanalysis due to the small sample size. Despite the limitations presented, our results demonstrate relationships between cognitive function and retinal vascular integrity, cardiac health, and exercise measures, respectively, following a 12-week cardiac rehabilitation program in a sample of older adults at high risk for persistent CVD and cognitive decline. Taken together, our findings suggest that retinal vascular integrity predicts episodic memory performance in a small group of older adults highly vulnerable to persistent CVD, CBVD, and cognitive decline, which was not, in this instance, mediated by duration or frequency of exercise during 12 weeks of cardiac rehabilitation. Future studies with larger samples should examine exercise as a modifier of the relationship between retinal vascular health and cognitive function, given the enthusiasm for exercise as a potential neuroprotectant in preclinical 28 and clinical 29 CBVD, CVD, and dementia.
Supplemental Material
sj-docx-1-oed-10.1177_25158414251340541 – Supplemental material for Pilot study examining the relationship between retinal vasculature and cognition in older adults recently discharged from a 12-week cardiac rehabilitation program
Supplemental material, sj-docx-1-oed-10.1177_25158414251340541 for Pilot study examining the relationship between retinal vasculature and cognition in older adults recently discharged from a 12-week cardiac rehabilitation program by Jordan Sergio, Emma Gosselin, Edmund Arthur, Wen-Chih Wu and Jessica Alber in Therapeutic Advances in Ophthalmology
Supplemental Material
sj-docx-2-oed-10.1177_25158414251340541 – Supplemental material for Pilot study examining the relationship between retinal vasculature and cognition in older adults recently discharged from a 12-week cardiac rehabilitation program
Supplemental material, sj-docx-2-oed-10.1177_25158414251340541 for Pilot study examining the relationship between retinal vasculature and cognition in older adults recently discharged from a 12-week cardiac rehabilitation program by Jordan Sergio, Emma Gosselin, Edmund Arthur, Wen-Chih Wu and Jessica Alber in Therapeutic Advances in Ophthalmology
Footnotes
Acknowledgements
The authors would like to acknowledge the staff at the Cardiac Rehabilitation Program at the Miriam Hospital for their collaboration on this study, the Lifespan Clinical Research Center for operational support, and the volunteers who participated in this study for their time and effort.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.