
Abstract
The prevalence of dementia is increasing in our aging population at an alarming rate. Because of the heterogeneity of clinical presentation and complexity of disease neuropathology, dementia classifications remain controversial. Recently, the National Plan to address Alzheimer’s Disease prioritized Alzheimer’s disease-related dementias to include: Alzheimer’s disease, dementia with Lewy bodies, frontotemporal dementia, vascular dementia, and mixed dementias. While each of these dementing conditions has their unique pathologic signature, one common etiology shared among all these conditions is cerebrovascular dysfunction at some point during the disease process. The goal of this comprehensive review is to summarize the current findings in the field and address the important contributions of cerebrovascular, physiologic, and cellular alterations to cognitive impairment in these human dementias. Specifically, evidence will be presented in support of small-vessel disease as an underlying neuropathologic hallmark of various dementias, while controversial findings will also be highlighted. Finally, the molecular mechanisms shared among all dementia types including hypoxia, oxidative stress, mitochondrial bioenergetics, neuroinflammation, neurodegeneration, and blood–brain barrier permeability responsible for disease etiology and progression will be discussed.
Introduction
In recent years, dementia due to various causes is becoming common in the elderly. Notably, abnormal protein deposition has been shown to co-exist with damaged neurovasculature in dementias at various disease stages. The relationship between vascular dysfunction and dementia has been described several decades ago. During the nineteenth century, pathologists have noted small blood vessel narrowing in the brain and described its association with hypoperfusion leading to brain damage. This became known as arteriosclerotic dementia—the hardening of arteries.1,2 In 1907, Alois Alzheimer reported senile plaques in the brain of patients, which have become the neuropathologic hallmark of Alzheimer’s disease (AD). Further, Alois Alzheimer posited that circulatory system impairment might serve as the trigger for AD pathology. Yet most pathologists at that time classified AD as purely degenerative, with uncertain etiology. In the mid-twentieth century, experts began to challenge the dichotomy between arteriosclerotic and degenerative dementia, questioning the etiology of AD. From that point on, the concept of vascular dementia (VaD) has evolved and transformed (for additional information, refer to ‘Classifications of dementias’ section). In 1974, Hachinski et al. 3 defined arteriosclerotic dementia to include multiple small-vessel infarcts, offering a new perspective on the cerebrovascular causes of dementia. With the advent of noninvasive computed tomography of the brain and, later, magnetic resonance imaging (MRI) technology, the clinical understanding of vascular disease was improved. This led to mounting evidence on a wide spectrum of ischemic changes and abnormal findings in apparent cognitively normal elders, which further perplexed investigators and clinicians alike. 4 Since the emergence of MRI as a unique tool coupled with advances in related diagnostic technologies, the diagnosis of dementia today is integrative and uses a variety of diagnostic tools to merge neuroimaging and immunohistopathologic analysis to assess the contributions of various neuropathologic mechanisms, including vascular factors, in dementia. 5
Cerebrovascular changes are common neuropathologic findings in aged subjects with dementia. 6 Vascular remodeling and pathologic changes to the macro- and microvasculature may disrupt blood vessel integrity. Notably, such remodeling leads to vascular disease and cerebral hypoperfusion associated with neuronal injury, structural and functional brain damage. 7 More specifically, neuroimaging findings indicate white matter hyperintensities, cerebrovascular lesions, and cerebral amyloid angiopathy (CAA). 8 Other ultrastructural abnormalities to the microvasculature associated with small-vessel disease, and exacerbated by aging, include capillary wall deterioration and the accumulation of erythrocytes, 9 basement membrane thickening, and pericyte degeneration, 10 resulting in blood–brain barrier (BBB) permeability 11 and vascular cognitive impairment (VCI). Vascular cognitive impairment is a broad term that encompasses cognitive deficits associated with vascular disease, ranging from mild-to-severe cognitive impairment including VaD. 12 A new and all-inclusive term was recently coined referred to as VCID (vascular contributions to cognitive impairment and dementia). It is now often used by many groups, including NIH, since it is not restrictive to a particular diagnosis but rather highlights the contributions of many dementias. Moreover, hemodynamic impairment of mean blood flow velocity, pulsatility index, and cerebrovascular reactivity were found in AD patients as compared with controls using transcranial Doppler to monitor the middle cerebral artery. 13 These results suggest hemodynamic impairment as a critical marker of cognitive decline and confirm its role as an early predictor of vascular damage in AD. Similarly, previous studies have observed cerebrovascular changes in DLB, partially (in 30% of the cases) characterized by cortical microbleeds and CAA. 14 Some cases of FTD associated with white matter alterations and small-vessel disease. 15 Interestingly, VaD incorporates certain key neurovascular features of AD-related dementias (i.e., cerebral microbleeds, infarcts, CAA), which significantly correlates with vascular risk factors in clinical studies. 16 However, it is unclear whether this relationship is purely coincidental and cumulative or, alternatively, casual and synergistic. Treatments aimed at reducing vascular risk factors, such as better blood pressure control, improved diet, and exercise have been shown to improve disease incidence and progression. 17
The brain histopathology and pathophysiology may not necessarily reflect clinical symptoms. The disease(s) may take years to manifest their cognitive, behavioral, and functional impairments. Several autopsy studies of nondemented, aged individuals confirm mixed cerebrovascular pathologies and neuropathologic findings, suggesting a complex and silent form of subclinical disease.18,19 Additional support for this claim is derived from the seminal nun studies. Autopsies of nearly 500 human brains found that the prevalence of dementia in persons beyond the age of 75 is very high. Moreover, only 10% of the nuns in this group exhibited ‘brain reserves’, or the ability to tolerate high-stage AD-related neuropathologic alterations without developing clinical symptoms of dementia. 20 In another related study, nuns diagnosed with dementia often showed signs of underlying cerebrovascular dysfunction as defined by the presence of lacunar infarcts and these participants tended to have less severe AD-related changes than participants with similar cognition but without overlapping vascular disease pathology. 21
With the wide spectrum of available literature on cerebrovascular alterations in different dementias, in the following sections, we will first provide current evidence linking cerebrovascular abnormalities to AD-related dementia. Next, a discussion of vascular impairments in various other forms of dementia will follow, along with controversial hypotheses regarding vascular contributions to cognitive impairment. Finally, we will highlight emerging vascular risks and molecular mechanisms predisposing individuals to dementia.
Classifications of dementias
The incidence of dementia is exponentially increasing and has become one of the major public health concerns in recent years. According to the World Health Organization census in 2010, there were approximately 35.6 million people worldwide living with dementia, a number that is expected to triple by 2050.
22
With the yearly diagnosis of 7.7 million new cases of dementia worldwide, the medical cost burden surpasses that of cancer and heart disease combined.
23
Furthermore, dementias may be difficult to clinically diagnose because of their multifactorial causes, overlapping symptoms, and variety of degenerative pathologies, resulting in inconsistent clinical presentation and diagnostic challenges.
24
For example, a retrospective study using the National Alzheimer’s Coordinating Center database was recently conducted on the accuracy of AD diagnosis. Autopsies of 533 AD patients demonstrated that 119 subjects did not meet the criteria for definite AD diagnosis. Among other neuropathologic findings, researchers found DLB ( Classifications of dementia subtypes and associated neuropathologic features. A hierarchy listing the four major categories of dementia with corresponding neuropathologic findings. A mixed phenotype represented by double-sided arrows indicates a shared disease neuropathology between two dementia types. A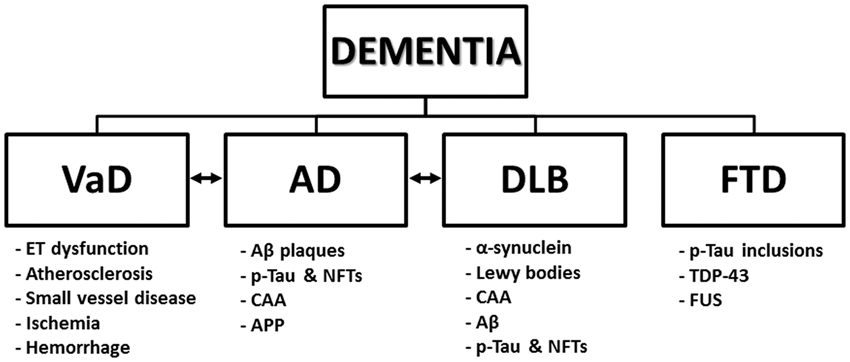
Alzheimer’s Disease
Alzheimer’s disease is the most common form of dementia, which often occurs with VCI.
26
The neuropathologic hallmarks of AD are the extracellular accumulation of senile plaques composed of A
Cerebrovascular effects of amyloid
Recent findings indicate that vascular changes often coexist with changes linked to AD, suggesting a synergistic effect on cognitive decline. Pathologic studies of the Alzheimer’s brain microcirculation have shown alterations of blood vessel morphology and decreased vascular density, combined with increased vessel tortuosity.
33
One significant contributor to AD-mediated cerebrovascular injury is A
Additional data indicates A
Although the majority of AD is sporadic, there is a strong genetic component to the disease. Apolipoprotein E-ɛ4 allele has been classified as one of the important genetic risk factors for late-onset AD and drives the accumulation of parenchymal A
Dementia with Lewy Bodies
Dementia with Lewy bodies is the second most common cause of neurodegenerative dementia in the elderly.
42
It shares clinical and pathologic characteristics of other dementias that may occur during the course of Parkinson's disease and other neurologic conditions.43,44 Pathologically, DLB is characterized by abnormal aggregation of the synaptic protein
Cerebrovascular dysfunction and neuroinflammation in dementia with Lewy bodies
Emerging evidence supports the contributions of hypoxia and vascular hemodynamic alterations in DLB.
46
Reductions in cerebral blood flow and decreased microvessel density associated with vascular endothelial growth factor deficiency, secondary to the accumulation of
Controversies of dementia with Lewy bodies as a cerebrovascular disease
Data regarding the prevalence of cerebrovascular pathologies in DLB patients remain scarce and contradictory. An interesting study by Ghebremedhin et al. 51 found that patients with co-existing vascular disease were likely to have less Lewy body pathology than patients with only Lewy body disease in autopsy samples of DLB brains, consistent with a cumulative pathology hypothesis. The extent of Lewy body pathology inversely and significantly correlated with the severity of vascular pathologies, such as atherosclerosis, infarcts, and small-vessel disease. In contrast, CAA and NFTs were positively and significantly correlated with DLB pathology. Consequently, the authors concluded that patients with advanced Lewy body pathology were less likely to present with vascular dysfunction and/or stroke.
Although the complexities of AD-related dementias and their clinical diagnosis remain a challenge, there is a clear gap in knowledge regarding vascular contributions in pure DLBs. 52
Frontotemporal Dementia and Related Tauopathies
Frontotemporal dementia is a heterogeneous neurodegenerative group of non-AD dementias with a variant clinical and pathological profile. Several genes have been identified that cause the autosomal dominant familial forms of FTD. However, our focus will be on sporadic FTD, which represents 60% of cases. 53 The sporadic form of the disease typically develops in the elderly during the sixth decade of their life. 54 The term frontotemporal lobar degeneration (FTLD) refers to the neuropathology of the FTDs. Pathologically, the FTLDs are characterized by atrophy of the frontal and temporal lobes (lobar atrophy), which contrasts the diffuse atrophy of AD, and by some or all of the following microscopic findings: neuronal loss and gliosis, vacuolization of the superficial cortex (spongiosis), and ballooned neurons. 55 Frontotemporal dementia can be further subdivided into three different categories: (1) FTD-tauopathies (examples: progressive supranuclear palsy, Pick’s disease, corticobasal degeneration, Argyrophilic grain disease, etc.); (2) FTD-ubiquitin with ubiquitin-positive tau-negative neuronal inclusions (examples: motor neuron disease and sporadic amyotrophic lateral sclerosis), and (3) FTD-without tau- or ubiquitin-positive inclusion (examples: amyotrophic lateral sclerosis, and in some cases of AD, Pick’s disease, and DLB). 56 These variants differ in terms of clinical presentation, cognitive impairment, and affected brain regions. 57 This categorization is reasonably well accepted.
Pathologic markers of frontotemporal dementia
The neuropathologic hallmarks of these diseases include gliosis, neuronal loss, superficial spongiform degeneration, and atrophy of the frontal and temporal lobes, often culminating with progressive aphasia, disintegration of personality and behavior, severe memory loss, and language impairments. 58 Neuroimaging modalities such as MRI are necessary to provide an accurate diagnosis. Distinctive MRI features often include frontal and anterior temporal lobe atrophy, altered white matter signals reflecting gliosis, and frontotemporal brain hypometabolism. Another common histopathologic finding associated with the FTD group of diseases is tissue deposition of abnormally aggregated proteins. Three major pathogenic proteins have been implicated in the autopsy studies of sporadic FTD: (1) FTD-Tau: cellular p-tau inclusions (in both sporadic tauopathies and familial FTD linked to parkinsonism on chromosome 17, FTDP-17T) 59 and (2) FTD-transactive response DNA-binding protein-43 (TDP-43): the main ubiquinated peptide in tau-negative FTD, 60 representing the majority of cases, 61 while (3) inclusions of fused in sarcoma (FUS) proteinopathy are a seldom occurrence associated with a clinical diagnosis of behavioral variant FTD. 55 The tau-protein is typically involved in the regulation of microtubule assembly and disassembly, and has been shown to have an important role in FTD cases of tau- or ubiquitin-positive inclusions. 62 These tau abnormalities may also lead to tau aggregation or microtubule dysfunction, which in turn, may affect axonal transport.
Vascular risk factors associated with frontotemporal dementia
Only a few risk factors have been recognized to contribute to FTD etiology and only a few studies have investigated the relationship between vascular impairment and FTD. One of these risk factors is family history of FTD. Recent autopsy data of FTLD brains with tau inclusions supports the role of small-vessel dysfunction in FTD disease progression.
15
Investigators reported the prevalence of white matter arterial changes within frontal and temporal lobe regions associated with demyelination. These effects correlated with older age and suggest the presence of vascular co-morbidity in FTD. However, there is evidence arguing against the role of cerebrovascular dysfunction in FTD, including a negative effect or no correlation altogether, consistent with a cumulative pathology hypothesis. One reason that conclusions may be particularly difficult to reach regarding the role of vascular disease in FTD is the diverse etiologies associated with each of the FTDs, including both genetic and environmental influences (i.e., FTD because of trauma manifests differently than FTD associated with TDP-43). A case–control study containing 80 cases of veterans with sporadic FTD found a significant association between FTD and head injury. In fact, the prevalence of traumatic brain injury was significantly greater in veterans with FTD versus those with non-FTD dementias. Surprisingly, the FTD group also experienced a lower prevalence of heart and cerebrovascular disease, although vascular risk factors such as hypertension were similar between both the studied groups.
63
Additional evidence demonstrating an inverse relationship between FTD and cerebrovascular dysfunction is present in autopsy studies of FTLD brains. Young patients with
Vascular Dementia
The term VCI comprises the heterogeneous group of cognitive disorders that share a presumed vascular cause and includes both dementia and cognitive impairment without dementia. 66 Vascular dysfunctions, including large vessel disease, cardioembolic disease, and small-vessel disease are considered causal in patients with VaD compared with its additive or synergistic effects in association with the other dementias explained above. On the basis of the vascular hypothesis, VaD is caused by diminished cerebral blood flow, leading to hypoxia and BBB permeability from prolonged vasculotoxic and neurotoxic effects promoting neurodegeneration and amyloid deposition. 67 Vascular dementia has been classified into the following six dementia subcategories: (1) multi-infarction dementia, (2) strategic infarction dementia, (3) hemorrhagic dementia, (4) mixed dementia, (5) subcortical ischemic vascular dementia (SIVD), and (6) other forms of VaD. 68 The sudden occurrence of infarction and hemorrhagic stroke dementia subtypes associated with acute cerebrovascular diseases may parallel specific cortical or subcortical symptoms related to stroke-affected brain regions. Beyond the major categories of large vessel disease, cardioembolic and small-vessel disease, the remaining VaD subtypes, represent heterogeneous etiologies, including vasculitis, CAA, and inherited disease such as CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy). 69
The following section will address an emergently important VaD subtype, which is known to be caused by small-vessel disease in the brain and has been implicated in VaD.
Subcortical ischemic vascular dementia
SIVD is characterized by small-vessel vascular disease and is classified as a VCI subtype.
70
Hypertension represents a primary risk factor in sporadic SIVD (refer to ‘Cerebrovascular risk factors and neuropathological correlates of dementia’ section). The neuropathology is driven by severe stenosis and microvessel occlusion, culminating as white matter ischemia and multiple lacunar infarctions in subcortical structures.
71
Clinical studies of SIVD patients using dynamic contrast-enhanced MRI show significantly elevated albumin index and increased BBB leakiness, indicating abnormal white matter damage in the SIVD group as compared with controls.
72
Moreover, SIVD may be further divided into several clinical subtypes. The first presents with arteriosclerotic leukoencephalopathy in the white matter and is known as Binswanger's disease. This type of ischemic change in the brain is formed by widespread incomplete infarctions or white matter hypoperfusion.
73
The second is a rare hereditary disease referred to as CADASIL. Case reports of CADASIL patients have noted elevated A
Mixed Dementia
A mixed etiology of AD and VaD is thought to become more common with increasing age, particularly in individuals older than 85.
75
Data from epidemiologic studies indicate that approximately one-third of patients with AD present with vascular pathology,
76
suggesting that there is a strong vascular component promoting brain injury.
77
Clinicopathologic studies report a heterogeneous phenotype comprising AD (A
Cerebrovascular risk factors and neuropathologic correlates of dementia
Diabetes, hypertension, hypercholesterolemia, smoking, and old age are some of the vascular risk factors known to increase the risk for AD-related dementias.
82
Among these, hypertension has emerged as the strongest predictor of cognitive impairment, serving as a common denominator for a variety of neurodegenerative conditions. The following sections will focus on the role of hypertension in dementia, a novel research area that is only now beginning to emerge and describe known mechanisms of neuroinflammation and neurodegeneration leading to BBB permeability and manifesting dementia subtypes. We will also review neuropathologic findings associated with dementia, which are known to contribute to cerebrovascular risk (Figure 2).
Neurovascular factors driving neuropathology and dementia. A schematic representing the mechanisms of cerebrovascular injury because of hypoxia/hypoperfusion, metabolic dysfunction, and altered cerebrovascular hemodynamics with corresponding neuropathologic hallmarks leading to dementia. Additional pathologic markers of dementias include amyloid-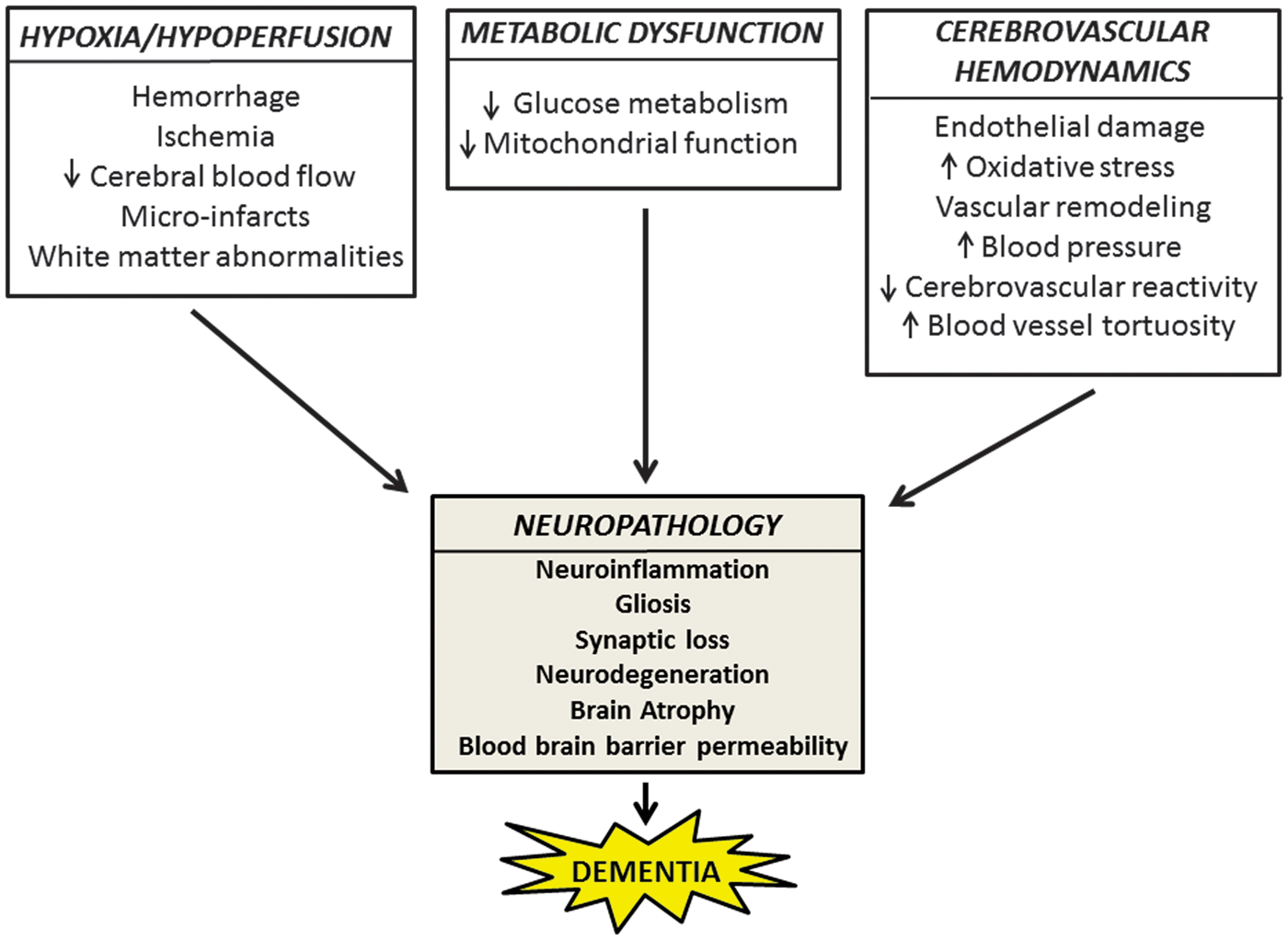
Hypertension
Hypertension is a shared risk factor of AD and VaD associated with significant memory impairments in late life. 83 Chronically elevated blood pressure promotes cerebrovascular remodeling, leading to a reduction in the lumen diameter by an increase in the wall-to-lumen ratio. 84 Additional consequences of prolonged systemic blood pressure include altered morphology of small cerebral arterioles that supply vulnerable brain regions necessary for cognitive function. 84
Epidemiologic and preclinical studies have recently begun to address the complex interactions between aging, hypertension, and AD pathology. The direct effects of hypertension on A
Efforts to determine the mechanisms of A
Only a few studies, thus far, have addressed the relationship between hypertension and other dementia types. Neuroimaging MRI studies quantified white matter lesions and brain atrophy in late-life dementia. Earlier studies suggested that deep white matter hyperintensities did not correlate with measures of brain atrophy, ventricular dilatation, or age, but were associated with a history of hypertension, thus supporting an association of deep white matter hyperintensities with ischemic and vascular risk factors.
97
In contrast, no correlation was found between cardiovascular risk factors and FTD. Clinical evaluation of 100 FTD elderly patients (mean age > 70) as compared with 200 age-matched controls found no differences with rate of hypertension, dyslipidemia, and obesity.
98
However, further studies are needed to confirm these results. A previous study from our group has investigated the mechanisms of VCI in a hypertensive model of small-vessel disease (spontaneously hypertensive stroke-prone rats with carotid occlusion and a high-salt diet), using EPR (electron paramagnetic resonance) technology.
99
An EPR lithium crystal was implanted
Neuroinflammation
Neuroinflammation is prevalent in AD and related dementias. A growing body of literature links active inflammatory responses to AD neuropathology.
101
Epidemiologic data suggest that neuroinflammation serves as an independent predictor of early death in AD.
102
Microglia, the resident macrophage of the brain, have been shown to associate with A
Mechanisms of hypoperfusion-induced neuroinflammation in Alzheimer’s disease
Recent evidence suggests that hypoxia and pro-inflammatory mediators of neuroinflammation may precede A
The role of neurovascular inflammation in dementia subtypes
The effects of neurovascular inflammation injury to the blood vessel wall because of adhesion of inflammatory markers are currently being investigated using novel AD animal models and innovative techniques. These studies have led to the observation that such ‘neurovascular inflammation’ is mediated by the peripheral systemic immune response, and that the two immune systems may work synergistically, thus influencing AD neuropathology and cognition. 101 Although significant neurovascular inflammation has been reported, its role and contributions to the AD brain remains unclear.
Reports of neuroinflammation in other AD-related dementias further support its critical contributions to disease pathophysiology. For instance, in the early phases of DLB, patients showed extensive microglia activation in several associative cortices, as measured by the binding potential of [(11)C]-PK11195 with positron emission tomography.
119
On further examination, it was discovered that extracellular
Neurodegeneration
One timely question in the field is whether neurodegeneration precedes A
Several potential cerebrovascular risk factors have been implicated in neurodegeneration. The first is fibrinogen, known to induce clot formation. The deposition of fibrinogen in the AD brain promotes neuronal cell death and correlates with disease pathology. Moreover, small decrease in fibrinogen levels were shown to promote neuronal health and reduce A
Finally, previous studies report an association between loss of function in
Blood–Brain Barrier Dysfunction
The neurovascular unit, composed of neurons, astrocytes, myocytes, pericytes, extracellular matrix components, and endothelial cells forming the tight junctions of the BBB, is known to create a protective biochemical barrier between the brain microenvironment and the peripheral circulation. 135 Pathophysiologic changes occurring throughout the aging process, and exacerbated by cerebrovascular and neurodegenerative disease, may result in blood vessel tortuosity and vessel-wall thickening, causing reduced vascular reactivity. Vascular risk factors such as hypertension and diabetes associated with small-vessel disease may lead to BBB abnormalities, 136 reflected in increased albumin levels in the CSF and matrix metalloproteinase upregulation, known to disrupt tight junction proteins and promote cerebral edema. 137
In the AD brain, neurovascular unit pathology has been described as a consequence of A
Furthermore, BBB damage has also been noted in the other dementias. Observations of significant white matter abnormalities and demyelination because of underlying microvascular dysfunction in FTD were reported. 15 A separate study describes the rare occurrence of cerebrovascular lesions, 142 whereas microbleeds were more prevalent in the cerebral cortex of DLB brains. 142 Additional analyses by the same group revealed the prevalence and severity of cerebrovascular lesions in post-mortem brains of patients with DLB as compared with age-matched controls. 14 The authors concluded that these histopathologic changes reflect the neurodegenerative process, which is associated with BBB injury. 14 Increased BBB permeability reported in VaD patients corresponds to a higher mean albumin ratio (CSF/serum) as compared with healthy controls. 143 As there was no correlation between the albumin ratio and clinical vascular risk factors, the authors concluded that the observed BBB disruption is most likely because of small-vessel disease rather than cerebral infarcts. These findings were also confirmed among elderly individuals diagnosed with VaD, thus providing evidence for BBB leakiness as an early marker of cerebrovascular change in the disease process before the onset of clinical dementia. 144 A possible cause for the observed BBB damage in VaD may be attributed to the presence of matrix metalloproteinases in the white matter of patients as a result of underlying microvascular disease. 145
Conclusions and future directions
In conclusion, this review highlights several important key points. First, the possible multifactorial nature of sporadic AD and related dementias is associated with vascular etiologies as a part of the disease process. Second, the review focuses on the molecular cascades and associated cerebrovascular factors contributing pathologically to different dementias. Third, although the timing of disease symptoms and progression is important, often patients present with significant tau and A
A recent report released by the Alzheimer’s Association, in collaboration with NINDS, argues for the need to create basic science animal models to address the neurobiologic mechanisms underlying sporadic AD and related dementias and to develop novel biomarkers for clinical trials.
146
More specifically, several top priority objectives were recognized in the field: (1) animal models to understand the mechanistic link between cerebrovascular dysfunction and cognitive decline and to investigate the neuropathologic time course of neuronal and white matter injury. Small-vessel disease models mimicking human AD-related and mixed dementias are particularly needed; (2) biomarkers capable of detecting preclinical dementia are necessary, as early detection is the key to future therapeutic interventions. If it fails, neurodegeneration will be impossible to reverse once pathologic cascades are initiated; (3) reducing A
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by NIH, RO1 grant, R01NS083704 (PI: KB) and NIH/NINDS, RO1 NS045847-07A1 (PI: Gary Rosenberg).
Acknowledgement
The authors would like to thank our collaborators, Drs Karen Santa Cruz and Gary Rosenberg for their guidance and support throughout the review drafting and revisions process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
All the authors contributed equally to the conceptualization, design, and outline of this manuscript. LR collected the literature, created the figures, and provided the initial draft of the review. JK offered valuable clinical insight to answer the reviewers’ comments and ensure clinical accuracy of the manuscript during the revisions process. KB provided feedback throughout the entire writing process and was instrumental during the editing process.