
Abstract
Purpose:
To investigate in vitro the accuracy of dynamic contour tonometry, Goldmann applanation tonometry, and Tono-Pen XL in edematous corneas.
Methods:
Experimental study included 20 freshly enucleated porcine eyes. Epithelium was debrided, and eyes were divided in four groups. Groups were immersed in 35%, 40%, 50%, and 60% glycerin solutions for 3 hours. Subsequently, globes were mounted in a special holder, and their intraocular pressure was hydrostatically adjusted. Intraocular pressure was measured by means of dynamic contour tonometry, Goldmann applanation tonometry, and Tono-Pen XL while adjusting true intraocular pressure to 17, 33, and 50 mm Hg. Ultrasound pachymetry was performed.
Results:
Mean corneal thickness was 914.5 ± 33.3 μm (730–1015 μm). In true intraocular pressure of 33 mm Hg, Goldmann applanation tonometry and dynamic contour tonometry significantly underestimated true intraocular pressure (mean Goldmann applanation tonometry: 14.7 ± 4.8 mm Hg, p < 0.001, mean dynamic contour tonometry: 21.6 ± 6.8, p < 0.001). Tono-Pen XL also underestimated, but difference was not statistically significant (Tono-Pen XL: 27.9 ± 9.7, p = 0.064). In true intraocular pressure of 50 mm Hg, all three methods significantly underestimated (Goldmann applanation tonometry: 17.6 ± 5.3 mm Hg, p < 0.001, dynamic contour tonometry: 26.8 ± 6.3 mm Hg, p < 0.001, Tono-Pen XL: 35.6 ± 8.4 mm Hg, p < 0.001). The error in measured intraocular pressure for each method (true minus measured intraocular pressure) was significantly correlated to true intraocular pressure (p < 0.001). The intraocular pressure measurements of each eye taken under true intraocular pressure of 17 and 33 mm Hg with the three methods were correlated to each other. Measurements taken under intraocular pressure of 50 mmHg were not correlated to each other. Corneal thickness was not correlated to intraocular pressure measurement.
Conclusion:
Goldmann applanation tonometry, dynamic contour tonometry, and Tono-Pen XL underestimate intraocular pressure when measured under edematous conditions. Tono-Pen XL showed better accuracy, especially in lower true intraocular pressure. The measurement error increases when true intraocular pressure increases in all three methods.
Introduction
Measurement of intraocular pressure (IOP) is a fundamental part of the ophthalmologic examination for the assessment and management of glaucoma progression. Goldmann applanation tonometry (GAT) has been established as the gold standard for routine measurement in everyday clinical practice. Accuracy of GAT measurements depends on several parameters, including corneal thickness, corneal curvature, and biomechanics.1–3 Corneal thickness is considered to have a significant influence on the measurement of GAT; thus, it is now recommended to be taken under consideration for the assessment of risk for glaucoma progression in addition to GAT. 4
Corneal edema, as it directly affects corneal thickness and biomechanical properties,5,6 is also a factor that modifies the measured IOP. Several studies have assessed the effect of edema on GAT with variable results.6–10
Currently, there are other methods except from GAT for the measurement of IOP. Dynamic contour tonometry (DCT) is a nonapplanation contact tonometry method which is considered to be largely independent from corneal thickness and curvature. The Tono-Pen XL (TXL) is also an automated method with wide clinical use over the past decades. Tono-Pen is based on the same principle with the Mackay-Marg tonometer,
11
which was considered to measure IOP less affected
The purpose of our study is to investigate in vitro the accuracy of DCT, GAT, and TXL in edematous corneas.
Methods
Experimental procedure
Thirty enucleated porcine eyes were obtained from a local abattoir within 24 hours after slaughtering. Eyes were conserved in −4°C until the experimental procedure. Each eye was carefully observed under a surgical microscope to identify any corneal scars, epithelium defects, or corneal edema. Nine eyes were excluded from the study because of detection of a corneal abnormality. Careful corneal epithelium debridement was performed with a rotating brush in 20 eyeballs. After debridement, total globes were divided into four groups. Groups were immersed in glycerin solutions of 35%, 40%, 50%, and 60% concentration for 3 hours in order for the corneal hydrations to reach equilibrium in a variable range of edema. Using a surgical microscope, a 27-g needle was inserted at the limbus, through the pupil, and into the posterior chamber. The lens was not disrupted. Subsequently, each globe was mounted in a custom-made eye holder, and IOP was regulated hydrostatically through anterior chamber cannulation.
The IOP of each globe was measured by means of DCT, GAT, and TXL while adjusting true IOP to 17, 33, and 50 mmHg by the height of the saline column. The three levels of IOP were selected to perform the experiment under true IOP in the normal range, moderately increased, and significantly increased. Corneal ultrasound pachymetry was performed.
Our study did not require an ethical board approval by the University of Crete because it was an experimental procedure on postmortem porcine eyes provided by an abattoir.
Statistical analysis
Mean value of each instrument’s IOP measurements was compared with the corresponding true IOP with paired samples t test. Linear correlation between pairs of quantitative variables was assessed using Pearson correlation coefficient. Correlations were assessed among IOP measurements with all instruments to each other, among measured corneal thickness of each button and glycerin concentration of the corresponding solution and among corneal thickness of each experimental eye and IOP measurement with each devise. We calculated the error in measured IOP of each method (true minus measured IOP) and assessed its correlation with the true IOP. The level of p < 0.05 was accepted as statistically significant. The statistical package PASW Statistics 18.0 was used (SPSS Inc., Chicago, IL, USA).
Results
Results are presented as mean value ± standard deviation (SD). Mean corneal thickness of all corneas was 914.5 ± 33.3 μm (range 730–1015 μm). All corneas were in edematous condition, and thickness was significantly correlated with glycerin concentration (r = −0.82, p < 0.001). We found no statistically significant correlation of corneal thickness with tonometry with any of the three devices used. When true IOP was adjusted at 17 mm Hg, GAT and DCT significantly underestimated true IOP (mean GAT: 7.7 ± 5.9 mm Hg, p < 0.001, mean DCT: 10.6 ± 7.5, p < 0.001). Tono-Pen XL slightly underestimated, and difference was not statistically significant (TXL: 16.6 ± 7.5, p = 0.83). At true IOP of 33 mm Hg, GAT and DCT significantly underestimated true IOP (mean GAT: 14.6 ± 6.8 mm Hg, p < 0.001, mean DCT: 21.6 ± 67.7, p < 0.001). Tono-Pen XL also underestimated, but difference was not statistically significant (TXL: 27.9 ± 8.8, p = 0.064). At true IOP of 50 mm Hg, all three methods significantly underestimated true IOP (GAT: 17.4 ± 5.3 mm Hg, p < 0.001, DCT: 26.8 ± 7.3 mm Hg, p < 0.001, TXL: 35.6 ± 8.4 mm Hg, p < 0.001) (Table 1). The error in measured IOP of each method for all eyes (true minus measured IOP) was significantly correlated to true IOP (GAT error versus true r = 0.88, p < 0.001, DCT error versus true: r = 0.728, p < 0.001 TXL error versus true: r = 0.583, p < 0.001). Intraocular pressure measurements of each experimental eye taken with all three methods had a statistically significant positive correlation to each other when true IOP was adjusted at 17 mm Hg and also at 33 mm Hg. The measurements of IOP taken under true IOP of 50 mm Hg were not significantly correlated to each other (Table 2).
Mean results and comparisons of each tonometry result with the corresponding true IOP.
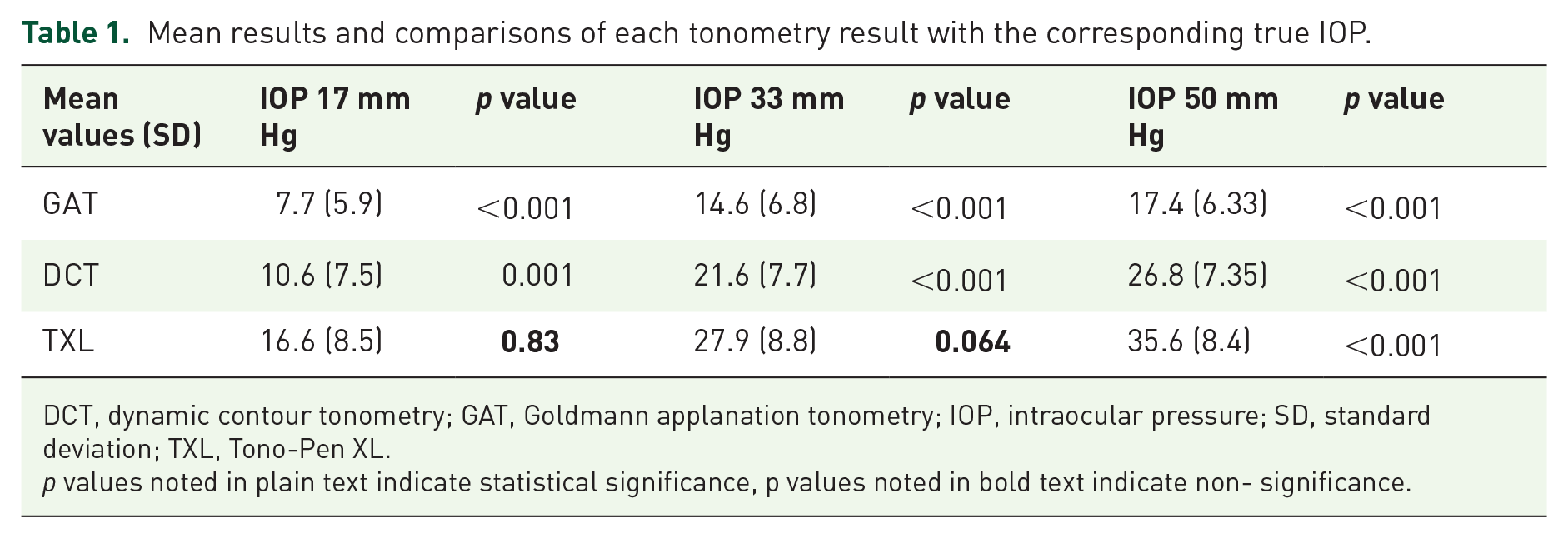
DCT, dynamic contour tonometry; GAT, Goldmann applanation tonometry; IOP, intraocular pressure; SD, standard deviation; TXL, Tono-Pen XL.
p values noted in plain text indicate statistical significance, p values noted in bold text indicate non- significance.
Results of correlations among measurements of each experimental eye with the three different methods.

DCT, dynamic contour tonometry; GAT, Goldmann applanation tonometry; IOP, intraocular pressure; TXL, Tono-Pen XL.
Discussion
The results of our in vitro study suggest that IOP measurement with GAT, DCT, or TXL through edematous corneas could lead to significant underestimation of true IOP. Corneal edema is a common condition associated with several corneal disorders or even postoperative course of several ophthalmic surgical procedures. Consequently, measurement of IOP through edematous cornea is a common condition in clinical practice. Underestimation of true IOP in such cases should be taken under consideration in patients’ management.
Our results suggest that among the three tested tonometers, GAT is the most affected by corneal edema and significantly underestimates IOP. This is expected because corneal edema, as it directly affects corneal thickness and biomechanical properties, is also a factor that modifies GAT.5,6 The Goldmann tonometer is based on the Imbert-Fick principle to estimate the IOP by recording the force required to applanate an area of the cornea that is 3.06 mm in diameter. This principle is applied with the assumption that true IOP can be measured if there is equilibrium of the four main forces involved: IOP, corneal rigidity, adhesion force of the tear film, and appositional force of the tonometer. The calibration of the Goldmann tonometer is based on the average population values of corneal thickness shape and rigidity. As a result, the measurements taken in corneas that are highly differentiated from the usual as in the case of edema are not expected to be reliable.
With regard to the effect of corneal edema on GAT, there are clinical studies with somewhat contradictory results. According to Lau and Pye 6 and Hamilton and colleagues 8 contact lens–induced edema causes a small increase in the measured GAT. On the contrary, Oh and colleagues 9 found underestimation of IOP by GAT in individuals with contact lens induced edema. Simon and colleagues 7 carried out GAT measurements on cadaver eyes undergoing osmotically controlled hydration measured by pachymetry. They found that GAT readings were inversely correlated with change in corneal thickness, with a decrease of 9.2 mm Hg being observed between minimum and maximum hydration. Huang and colleagues 10 found that postoperative edema causes a significant underestimation of IOP from the Goldmann applanation tonometer. The authors of this study also state that the underestimation is associated with the amount of edema in lower than medium edema, and not associated in increased edema. In our results, GAT significantly underestimated true IOP in all tested levels of IOP. It is possible that greater amounts of edema as in our study cause underestimation, whereas small amounts of edema as in contact lens wear do not have always this result.
With regard to DCT, our study indicates that it also underestimates IOP in corneal edema. This is in agreement with other previous clinical studies. Hamilton and colleagues 8 found that it underestimates IOP in patients with contact lens–induced edema. Oh and colleagues 9 have shown similar results and, additionally, stated that it is more affected than GAT. In our study, the DCT significantly underestimated IOP in all measurements, but underestimation was less than with GAT. It seems that though less affected by thickness and corneal contour than GAT, DCT still remains affected by corneal edema.
The Tono-Pen tonometer is an automated method with wide clinical use since the last decades. It has similar principle of function as the MacKay-Marg tonometer 11 which has been demonstrated to be accurate in edematous corneas, more than the Goldmann tonometer. 12 In a clinical study by Chang and colleagues, 13 it was demonstrated that Tono-Pen measurements in corneas thickened by edema secondary to endothelial dysfunction or Descemet Stripping Automated Endothelial Keratoplasty (DSAEK) do not need to be corrected for the amount of edema. According to our results, the Tono-Pen has increased accuracy in comparison with the other two tested tonometers in eyes with corneal edema. It is possible that because it employs a small contact area surrounded by an external sleeve that absorbs the force required to bend the cornea, the Tono-Pen is less affected by thickness and edema.
Another in vitro study by Neuburger and colleagues 14 demonstrated the increased accuracy of Tono-pen in measuring IOP through edematous corneas. This study also measured in vitro the manometrically adjusted pressure. Major difference with our study is that we used whole globes of porcine corneas, thus including the effect of the whole globe and scleral rigidity, instead of donor corneas on artificial chamber.
In our study, underestimation was increased in higher level of true IOP in all tested methods. Regarding GAT, this finding is in accordance to the results by Kniestedt and colleagues, 15 who tested GAT and DCT in human cadaver eyes under edematous and dehydrated conditions in a range of manometricaly calibrated IOP from 5 to 60 mm Hg. The authors also found significant underestimation of IOP from GAT in edematous condition, but not by DCT. They also state that the measurement error increased with increasing true IOP. In the study by Neuburger and colleagues, 14 authors also report analogous findings regarding underestimation in edema by GAT, although they used a Perkins tonometer rather than a Goldmann tonometer. Furthermore, likewise that study, we did not find a correlation of corneal thickness with measured IOP, indicating that existence rather than severity of edema affects the result. In our study we had similar findings in GAT as well as DCT, but more significant error in GAT. This parameter should be taken under consideration when high IOP is measured in eyes with edematous corneas.
A significant limitation of our study is that it was conducted on porcine corneas in vitro. Differences between clinical and laboratory setting may have a significant impact on tonometry results, as in the study by Eisenberg and colleagues. 16 The authors found an increased accuracy of tonopen in laboratory measurements, in contrast to decreased accuracy in vivo. On the other hand, in vivo comparisons can be made only between clinically used tonometry methods, and not with manometricaly defined IOP. Another significant limitation of this study is the absence of a control group of nonedematous corneas because all our experimental corneas had various degrees of edema.
In conclusion, our study provides evidence that IOP measurements obtained through significantly edematous corneas underestimate true IOP. Underestimation is more significant in higher levels of IOP than lower levels. The TXL shows increased accuracy in comparison with GAT and DCT, especially in lower true IOP levels, when measuring through edematous corneas.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr George A. Kontadakis was supported by a grant from the ‘Hellenic Society of Intraocular Implant and Refractive Surgery’.