
Abstract
Elevated IOP in clinical practice is usually seen in glaucoma or ocular hypertension. Glaucoma affects 60 million people worldwide and 8.4 million are bilaterally blind from this chronic disease. 1 Options for reducing IOP rely on pharmacological agents, laser treatments and surgery which may be penetrating or non-penetrating. The last twenty years has seen significant changes in all of these strategies. This review aims to cover these clinical options and introduce some of the new technologies currently in development for the clinical lowering of IOP.
Introduction
In 2002, an international consensus panel published definitions of open-angle glaucoma (OAG) and angle-closure glaucoma (ACG) that are now widely accepted. 2 In OAG the IOP may, but need not necessarily be elevated, the drainage angles are open and there are characteristic structural and functional changes manifest as optic disc damage and visual field loss. 12 IOP lowering may take weeks or months to reach target. ACG, where the drainage angle is occluded, may present acutely with very elevated IOP requiring urgent and immediate lowering or sub-acutely where the management may be similar to OAG. The existence of OAG, ACG and secondary causes of glaucoma reinforces the need for a variety of IOP lowering treatment options with differing mechanisms of action and speed of onset. Although the aetiology of glaucoma is multifactorial the only modifiable risk factor is IOP and numerous studies have shown that reducing IOP prevents glaucoma or delays progression of established disease. 3 12
Physiology of Aqueous Humor (Fig. 1)

Schematic diagram of physiology of aqueous humor.
IOP is determined by the rate of aqueous humor production (inflow) and exit from the eye (outflow). Aqueous humor is produced by the nonpigmented epithelium of the ciliary body and exits the eye through either the trabecular meshwork (conventional pathway) or via the uveoscleral (unconventional pathway). The conventional pathway consists of the sieve like trabecular meshwork, Schlemms’ canal and 360° collector channels for aqueous humor that lead to the episcleral venous system and 80% of flow is via this route. The remaining 20% flows directly through the iris root and interstitial spaces of the ciliary muscle into the suprachoroidal space (uveoscleral pathway). This pathway was discovered later, in the 1960s, but is an important target for newer drug treatments. 13 The relative percentages change with age and presence of disease. 14 17 Episcleral venous pressure has an impact on trabecular outflow so it also influences IOP. The relationship is described as follows:

where F is aqueous humor formation (μL/min), U is uveoscleral outflow (μL/min), C is trabecular meshwork outflow facility (μL/min/mmHg) and Pv is the episcleral venous pressure mmHg. Pharmacological modulation of carbonic anhydrase, adenosine triphosphatases and adrenoreceptors located in the nonpigmented ciliary epithelium can reduce aqueous production and thus lower IOP. Similarly, pharmacological modulation of adrenoreceptors and prostanoid receptors located in the trabecular meshwork or ciliary body can increase aqueous outflow through both pathways and lower IOP.
Pharmacotherapy (Table 1)
Pharmacological IOP lowering agents: efficacy, side effects and mechanism of action.

Topical IOP treatments have been available since the 1870s with Pilocarpine introduced in 1875 and epinephrine drops in 1925. Modern day ocular hypotensives that are still in clinical use arrived in 1978 when timolol maleate was first marketed in the United States. A number of effective topical beta adrenergic blocking agents then followed. They gained widespread acceptance in the 1980s because for the first time topical medications had few visual or ocular side effects. 18 For the next 25 years timolol became the gold standard to which all other topical IOP medications were compared. 18 The 1990s saw the next phase of new and clinically important IOP lowering agents with the selective α2-adrenergic receptor agonist apraclonidine (Iopidine) released in 1988 and the more selective α2-agonist brimonidine tartrate (Alphagan) in 1996. Topical carbonic anhydrase inhibitors became commercially available in 1995 with dorzolamide (Trusopt) and brinzolamide (Azopt) in 1998. Prostaglandin analogues heralded a new era in topical IOP lowering therapy with improved efficacy, tolerability and a once daily dosing regimen. Table 1 demonstrates the main IOP lowering agents in current clinical practice.
Prostaglandin derivatives
Currently the most effective drugs for pressure reduction are Prostaglandin F2alpha analogues. This class now includes latanoprost, bimatoprost, travaprost, tafluprost and unoprostone.
Unoprostone (Rescula; Ciba vision) was the first commercially available prostaglandin analogue and became available in Japan in 1994 and in the United States in 2000. However, it is little used as it has limited efficacy and requires twice daily topical administration. 19 25 There is some newer evidence that it may have a neuroprotective effect and interest in it has been renewed. 20
Latanoprost was introduced to the US market in 1996, travoprost and bimatoprost in 2001. Latanaprost and Travaprost are ester prodrugs of PGF 2 alpha and Bimatoprost is the amide prodrug of 17-phenyl-PGF 2alpha. Bimatoprost, latanoprost and travoprost have received American (FDA) and European (EMEA) approval as first line agents in patients where IOP reduction is desired, specifically OAG and OHT. The decline in the rate of glaucoma surgeries since the 1990s has in part been attributed to these agents. 26 29 They are more effective than beta blockers and have comparable tolerability on a once daily dosing regimen with less systemic side effects. The PG analogues share similar modes of action by potentiating both the trabecular meshwork route and uveoscleral pathway for aqueous drainage. 30 36
Latanoprost,37,54,55 bimatoprost 56 58 and travoprost56,59–61 have been shown to be equal or similar to timolol in lowering pressure in patients with open angle glaucoma or ocular hypertension and typically reduce IOP by 20%–35%.31,37–53 Pooled evidence suggests that latanoprost reduces diurnal variation in IOP significantly more than timolol by an average of 1.2 mmHg (P < 0.001). 62
Beta blockers
Topical Beta blockers reduce aqueous production and have a peak effect in 2 hours. They typically reduce IOP by 20%–27% from baseline. 56
Bronchospasm and bradycardia remain the main concerns with use of topical β blockers. Substantial systemic absorption can occur with all topical ocular hypotensives and one drop of 0.5% timolol may lead to a serum concentration of timolol equal to a 10 mg oral dose. 64 Systemic absorption is thought to be responsible for the nocturnal hypotension seen in some patients and may be a risk factor in progression of glaucomatous optic nerve damage. 65
Carbonic Anhydrase Inhibitors (CAI)
CAIs are available in topical and systemic preparations. Topical carbonic anhydrase inhibitors such as brinzolamide and dorzolamide reduce IOP by reducing aqueous production and are typically instilled 3× daily as monotherapy or twice daily when used in combination, usually with a topical beta blocker. They typically reduce IOP by 17%–20% from baseline. 56 The European Glaucoma Prevention Study (EGPS) 66 was a randomised multicentre double-masked placebo-controlled clinical trial evaluating the efficacy of IOP reduction by dorzolamide in preventing or delaying POAG in patients with ocular hypertension. The mean IOP reduction was 15% after 6 months and 22% after 5 years in the dorzolamide treated group, however there was also a 9% reduction in IOP at 6 months and 19% at 5 years in the placebo group. This may in part be explained by regression to the mean however it also reinforces the belief that there are other factors besides IOP which determine progression in glaucoma.
Oral CAIs such as acetazolamide are used in refractory cases of raised IOP or where topical treatment is not feasible as a temporising measure or while definitive treatment, usually laser or surgical, is being planned.
Adrenergic agonists
In the eye alpha-agonists activate alpha-1 receptors that stimulate contraction of iris dilators and Muller muscles leading to mydriasis and lid retraction. Their effect on IOP is predominantly by inducing vasoconstriction in blood vessels supplying the ciliary body thus decreasing aqueous production. 67 They also stimulate post junctional alpha-2 receptors in the ciliary body and episcleral vessles causing reduced aqueous production and increased uveoscleral outflow.14,65–68
Non-selective α adrenergic agonists such as dipivefrin 0.1% and epinephrine 0.25%–2.0% are no longer used in modern ophthalmic clinical practice as they have significant side effects (Table 1) and there are better α2 selective agonists now available apraclonidine 0.5%–1.0% (Iopidine) and brimonidine (Alphagan). Both decrease aqueous production. Brimonidine also has a secondary action on uveoscleral outflow.14,65,53 The hypotensive effect lasts 12 hours with a peak effect at 2 hours hence it's twice daily dosing. 65 Allergic reactions to brimonidine can occur in up to 25% of patients and usually develops within two weeks of the beginning of treatment. 66 In patients who can tolerate it, it is a useful ocular hypotensive agent but is rarely used first line and is reserved instead for use in combination, usually with timolol, or as monotherapy as a third line agent.
Apraclonidine 0.5% and 1% are equally effective in preventing IOP spikes post YAG iridotomy, 0.5% is more effective than 1% in IOP control post YAG capsulotomy and less effective for post trabeculoplasty IOP control. 240 Apraclonidine can induce a dramatic fall in IOP but there has always been concern about tachyphylaxis and the high rate of follicular conjunctivitis with prolonged use.241,242
In addition to their IOP lowering effects there is some evidence that α agonists may have potential as neuroprotective agents. Animal studies have shown that brimonidine may prevent retinal ganglion cell death independent of its IOP lowering effect. 71 73 Human studies suggest that there may be less retinal nerve fibre layer loss (RNFL) in patients treated with brimonidine compared to timolol over 12 months. 74
Parasympathomimetics
Parasympathomimetics, also known as cholinergics, work by directly stimulating the muscarinic receptors of the ciliary muscle that widen the anterior chamber angle resulting in increased outflow through the trabecular meshwork. They also have a direct action on the longitudinal ciliary muscle.
Pilocarpine is the most commonly prescribed cholinergic. It is short acting and is usually prescribed 4 times daily in drop form or once daily in the 4% gel formulation. It is also used pre laser treatment and in trabeculectomy surgery to constrict the pupil thus stretching the iris facilitating the creation of an iridotomy or iridectomy. It has been shown to decrease uveoscleral outflow and this may be of particular significance in eyes with a compromised trabecular meshwork. 75 Pilocarpine typically reduces the IOP by 20%–30%. 73 Pilocarpine's use is limited by the frequency of its application and by ocular side effects Table 1.
Osmotic agents
Osmotic agents such as mannitol 20% (1.0–1.5 g/Kg intravenously) and glycerol (1.0–1.5 g/Kg orally) are very effective in controlling acutely raised IOP. They must be used with caution as they increase blood volume and therefore increase cardiac preload. Careful assessment of renal and cardiac status is advised. They may also alter blood glucose levels.
Combination therapies
Despite advances in pharmacotherapy for raised IOP monotherapy fails to reduce IOP to a satisfactory level in 40%–75% of patients after more than 2 years of therapy.66,77 Switching within or between IOP lowering drug classes is usually attempted before adding a second agent. Adding a second drop has disadvantages of increased exposure to preservative and the risk of washing the first agent out prematurely when the second drop is instilled.
The introduction of fixed combination therapies brought hope for improved compliance and persistence with treatment as two drugs could be prescribed but in one preparation typically administered once or twice daily.
Use of β blocker preparations with either a prostaglandin analogue/prostamide, a CAI, pilocarpine or brimonidine have been shown to be more effective at lowering IOP than their use singly. 75 90 As previously mentioned topical β blockers and specifically timolol were the gold standard treatment for many years but with increasing popularity of PGA as first line agents the use of both these classes in fixed combination therapy has been popular. Webers et al published a systematic review of combination therapies in 2010. 91 They make the point that there are many possible combinations to assess with use of timolol 0.25% and 0.5% alongside bimatoprost, travaprost and latanoprost and using these combinations either in the morning or the evening making assessment of combination therapies not quite as straight forward as one might expect. Most of the eligible studies used timolol 0.5% and latanoprost in fixed combination. Diurnal variation is also important in fixed combination therapies with Weber et al reporting that the mean additional decrease in IOP when using latanoprost 0.005%/timolol 0.5% fixed combination in the morning was less (3.8 mmHg) than when used in the evening (6.3 mmHg). 91 It is important to note that the reported additional IOP lowering of latanoprost when added to timolol is higher when used concomitantly rather than when used as a fixed combination. 91 This may be partly explained by the fact that the combination therapy uses timolol 0.5% only once daily.
The CAI/β blocker fixed combination, Cosopt (trusopt and timolol 0.5%) has been shown to be equally effective at reducing IOP as its components used separately. 92 and as brimonidine and timolol 0.5% used separately 93 thus offering equivalent clinical effect on a simpler regime with its associated advantages.
Pharmacological treatments to lower IOP have improved dramatically. The newer topical ocular hypotensives have changed the paradigm by which clinically raised IOP is treated. The improved efficacy and tolerability of these drugs is in part responsible for the reduction in the number of glaucoma operations carried out since the 1990s. 26 29
Laser
An alternative or additive treatment to the use of pharmacotherapy is laser treatment. Laser may be applied to the trabecular meshwork (trabeculoplasty) or the ciliary body (Table 2).
Laser treatments to lower IOP.
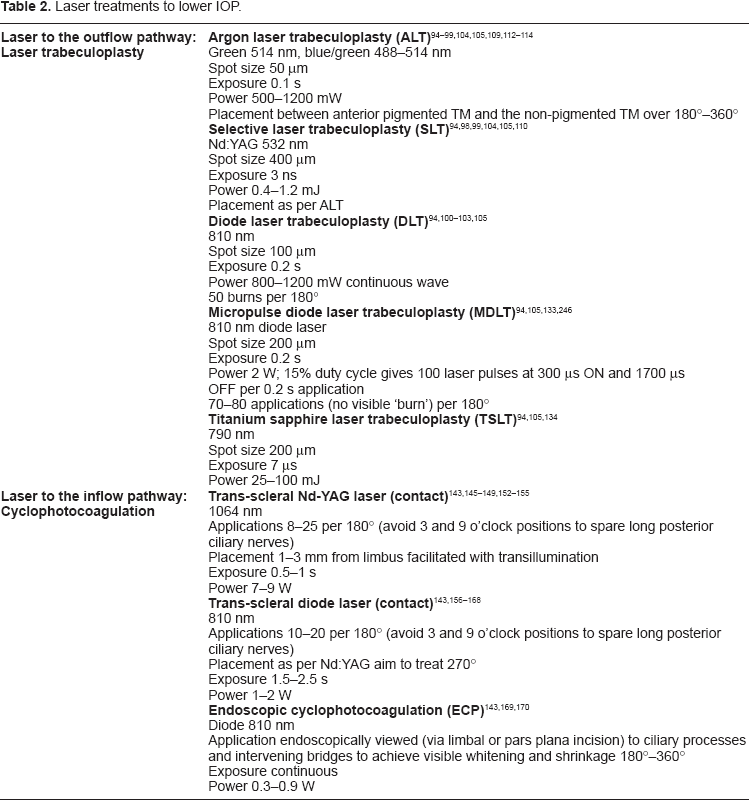
Laser trabeculoplasty
Argon Laser Trabeculoplasty (ALT)
Trabeculoplasty describes multiple laser burns applied to the trabecular meshwork. 94 Krasnov first reported on this technique using a ruby laser in 1972. 95 Following Hager's report of using argon laser to create what he thought was trabeculopuncture, 96 Wise and Witter 97 conducted a pilot study on the use of argon laser trabeculoplasty (ALT) reporting in 1979 that it lowered IOP. Subsequent studies have demonstrated ALT to be a safe and effective method of lowering IOP.
Selective Laser Trabeculoplasty (SLT)
In 1995, Latina and Park described SLT as an alternative laser modality applied to the trabecular meshwork to lower IOP. 98 This is an Nd:YAG laser that selectively targets the pigmented trabecular meshwork cells and uses several thousand times less energy than a standard ALT treatment. Histological studies have shown that is induces less structural damage change in the meshwork. 99
Diode Laser Trabeculoplasty (DLT)
The diode laser is a solid state laser and more compact and portable than an argon laser. It is traditionally used trans-sclerally to treat the ciliary body as will be discussed, however studies have reported its use in trabeculoplasty. 100 103
Micropulse-Diode Laser Trabeculoplasty (MDLT)
MDLT is a large spot, low irradiance treatment that uses an 810 nm diode laser to emit repetitive short near infrared laser pulses to confine the laser induced thermal effect spatially. 94 Theoretically each micropulse induces less thermal damage than ALT without compromising clinical effect.
Titanium-Sapphire Laser Trabeculoplasty (TSLT)
The titanium-sapphire laser has a longer wavelength than that used in ALT and SLT at 790 nm. It is thought that this near infrared wavelength may allow deeper penetration to the juxta canalicular meshwork which is thought to be the primary site of outflow resistance of aqueous humor. 94
Three recent reviews have been published on this technology.94,104,105
Mechanism of action of laser trabeculoplasty
The exact mechanism by which trabeculoplasty works is unknown but there are three main theories that are not necessarily mutually exclusive.
Mechanical theory
The mechanical theory suggests that electromagnetic energy produced by the argon laser is converted to heat energy when applied to the trabecular meshwork causing a burn which contracts trabecular meshwork tissue thus stretching adjacent portions of tissue. This is then purported to reduce resistance to flow in the trabecular meshwork and Schlemm's canal thus potentiating the conventional outflow pathway and reducing IOP. 104 Histopathological evidence and tracer studies supporting this theory have been provided in monkey eyes,106,107 however controversy still exists as Van Buskirk et al 108 failed to demonstrate a change in the cross sectional area of Schlemm's canal in enucleated human eyes after ALT. SLT does not induce contraction or scarring of the trabecular meshwork and yet still lowers IOP and therefore the mechanical theory applies more to ALT than SLT.
Biologic theory
This theory is based on the evidence that thermal energy stimulates cellular activity in the trabecular meshwork increasing the number and recruitment of macrophages thus allegedly remodelling the meshwork and increasing aqueous outflow. 107 Both ALT and SLT have been shown to release chemotactic and vasoactive agents such as interleukin-1 (IL-1), tumour necrosis factor (TNF-α). These molecules up regulate matrix metalloproteinase (MMP) expression triggering remodelling of the meshwork presumably decreasing resistance and potentiating outflow. 107 As SLT causes very little mechanical damage to the trabecular meshwork tissue, 99 unlike ALT, the favoured theory for SLT's mode of action is biological rather than mechanical.
Repopulation theory
Bylsma et al 111 suggested that laser energy stimulates increased cell division and trabecular meshwork repopulation. They demonstrated an increase in DNA replication 2 days after ALT treatment with increased cell division initially in the non- filtering portion of the meshwork migrating out to the trabecular beams where filtration does occur.
It appears that the trabecular meshwork has a multitude of responses to injury that are not necessarily stimulus specific.
Effectiveness of ALT
Evidence suggests laser trabeculoplasty provides clinically significant IOP reduction in more than 75% of initial treatments of previously unoperated eyes.11,112–118 When reviewing the literature, besides differences in methodology, follow up times and use of adjunctive treatments one must remember that many of the studies were conducted in the time when PG analogues were not available and thus the medical treatment arms of these studies usually rely on topical β blocker therapy. The Glaucoma Laser Trial compared the IOP lowering effects of 360 degree ALT vs. Timolol 0.5% as primary therapy for patients with open angle glaucoma. 113 The major findings were that ALT effectively lowered the IOP by 9 mmHg vs. 7 mmHg in the Timolol group. After 2 years 44% of the ALT group did not require additional interventions for glaucoma compared with 30% in the Timolol only group. After 7 years of follow up, the ALT treated eyes continued to demonstrate lower IOP and less subjective visual field loss progression compared with the eyes receiving timolol leading the authors to conclude that ALT was at least as effective as timolol in this scenario.
Effectiveness of SLT
Several studies have verified the IOP lowering effect of SLT 119 131 the magnitude of which has been reported as 11%–40% from baseline. A study by McIlraith et al 132 compared SLT to latanoprost and demonstrated an average IOP reduction of 8.3 mmHg in the SLT group vs. 7.7 mmHg in the latanoprost group. Overall, SLT's effectiveness is thought to be comparable to a single potent topical anti-glaucoma medication with the added benefit of easier compliance.104,126
The Cochrane systematic review of laser trabeculoplasty concluded that there was some evidence demonstrating similar effects in IOP control for diode and SLT compared with ALT at 6 months and one year follow up. 105 Detry-Morel et al 133 reported 3 months data on MDLT vs. ALT and found that the mean IOP decrease was 2.5 ± 2.6 mmHg in the MDLT group and 4.9 ± 3.4 mmHg in the ALT group (P = 0.04) Goldenfeld et al 134 reported mean follow up data at 15 months on titanium-sapphire laser trabeculoplasty vs. ALT and found similar reduction in IOP in both groups. The literature supports similar complication rates across all modalities of laser with transient IOP rise the most common.101,113 Iritis, corneal burns and reflux bleeding from the meshwork have also been noted. 94
Repeat treatments
Repeat ALT beyond 360 degrees is generally not recommended as it has relatively low efficacy but has increased risk of IOP spikes. 135 139 Evidence also suggests that eyes that receive repeat ALT within 12 months of the initial treatment will require further intervention more quickly than eyes with an initial success of more than 12 months. 135 Conversely, there is some evidence for repeat SLT therapy with Shah et al 140 reporting 70% success rate of repeat SLT at one year and 53% at 2 years.
A major advantage of laser is that it does not rely on adherence and persistence with topical medical treatment longterm and studies suggest that laser trabeculoplasty is less costly when compared with medical and filtering-surgery groups.141,142
Laser ciliary body ablation
Cyclodestructive procedures are traditionally reserved for cases of raised IOP that are refractory to pharmacotherapy and outflow surgery and in eyes that have little or no visual potential. Cyclodestruction has been achieved by various methods including surgical excision, diathermy, ultrasound, cryotherapy and laser. 143 Laser to the ciliary body may be employed via a contact or non-contact approach through the sclera using the Nd:YAG laser(Surgical Laser Technologies Inc., Malvern, PA) or the more portable semi- conductor diode laser (IRIS Oculight SLx, Iris Medical Inc., Mountain View, CA). An endoscopic approach where the ciliary processes are lasered under direct vision (ECP) has gained in popularity particularly in eyes where there is good visual potential. 143
Trans-scleral Cyclophotocoagulation (TCP)
TCP administered with a Diode or Nd:YAG laser is usually carried out with a contact approach under regional anaesthesia (peri bulbar or retro bulbar technique) as the procedure is painful. Both diode and Nd:YAG offer comparable IOP lowering and safety profiles but the diode laser is more portable. Both contact and non-contact TCP have been shown to be effective therapies for reducing IOP in which medications and/or other surgeries have failed with success rates of 34%–94% at mean follow up 5.85 years. 144 168 Traditionally, concerns over side effects such as pain, hyphaema, uveitis, cataract progression, hypotony, phthisis and severe visual loss have meant that TCP has not been used earlier in the treatment schedule of raised IOP. Reported visual loss and adverse events are partially due to the underlying disease and not just due to laser cyclodestruction. The Diode Laser Ciliary Ablation Study Group 157 reported vision loss of 2 or more lines in 30% of treated eyes. In more recent studies where TCP has been used as primary surgery the rates of serious complications are less and may be due to lower energy settings and less severe forms of glaucoma than in previous studies. 163 168
Endoscopic Cyclophotocoagulation (ECP)
ECP causes localised shrinkage of the ciliary processes and this can be visualised as the treatment is applied. This is thought to cause an initial reduction in blood flow and aqueous producing capacity in the ciliary body with partial reperfusion at 1 month hence the lower associated rates of hypotony and phthisis. 143 ECP can be undertaken in conjunction with cataract surgery or in pseudophakic or aphakic eyes. As it is an intraocular procedure there is the associated risk of endophthalmitis not applicable to the trans-scleral approach. The largest series on ECP by Chen et al 1997 169 reports a mean IOP reduction of 34% from baseline at 12.9 months. Glaucoma medication usage was reduced from an average of 3 agents preoperatively to 2 postoperatively indicating that ECP is frequently an adjunctive treatment to medical therapy. As there is relative sparing of the adjacent tissues when compared to TCP, namely the iris root, pars plicata, pars plana and sclera there is a relatively lower incidence of vision threatening complications. Complications reported in the largest series included fibrin exudate in 24%, hyphaema 12%, cystoid macular oedema 10% and vision loss of 2 lines or greater in 6%.169,170
Surgery
When pharmacological and laser treatments have been unsuccessful in reducing IOP adequately surgery is usually indicated.
Surgery for raised IOP is divided into penetrating and non-penetrating groups. Surgical techniques have evolved over the last 40 years from the traditionally less predictable full thickness procedures to safer guarded antiproliferative enhanced trabeculectomy, implantation of glaucoma drainage devices and a variety of non-penetrating techniques such as viscocanalostomy and deep sclerectomy. For lowering IOP and preventing visual field loss, a recent Cochrane review 171 comparing the effectiveness of surgery vs. medical IOP lowering treatments found there was evidence of slightly better IOP control with surgery though no current evidence to support any difference in visual field progression.
Trabeculectomy
Trabeculectomy is the still the most widely used surgical procedure for glaucoma and is more effective in lowering IOP than medical or laser treatment. 114 A trabeculectomy creates a fistula between the anterior chamber of the eye and the subconjunctival space to allow controlled release of aqueous. The conjunctiva is reflected in either a fornix based or limbus based approach and a full thickness sclerostomy is made under a pre-fashioned partial thickness scleral flap. The conjunctiva is then resutured above the scleral flap. Aqueous flows through the sclerostomy and under the scleral flap. This fluid forms a conjunctival bleb and is thought to be carried away by vessels within the conjunctiva and also by evaporating across the conjunctival surface. The final IOP lowering effect is determined by the size of the bleb, downstream drainage from the conjunctival vessels and the scarring response around the bleb. Since its original description by Cairns in 1968 172 advances in operating microscopes, instruments, suture material and the introduction of antimetabolites have improved the success rates of trabeculectomy alongside a marked reduction in complications.5,171,173,174
The Collaborative Initial Glaucoma Treatment Study (CIGTS) 5 was a randomised controlled trial involving 607 patients with newly diagnosed open-angle glaucoma randomised to medication or trabeculectomy with or without 5- fluorouracil (5FU). The IOP was lower in the surgical group (mean 14–15 mmHg) than in the medical treatment group (17–18 mmHg) however as is common with most penetrating surgery the rate of cataract progression and incidence of cataract surgery was increased (6% medication group vs. 17% trabeculectomy group). In the hands of experienced surgeons the success rate of filtering surgery (alone, or with adjunctive medical therapy) in a previously un operated eye is reported to be up to 90% at 2 years, however as with any meta-analysis there are large differences in the criteria used to define success.77,171,175 Optimum success rates are achieved when the eye has not been exposed to previous interventions either surgical or medical. 176 Risk factors for failure of trabeculectomy to control IOP include previous exposure to topical medication (especially sympathomimetics), previous surgical manipulation of the conjunctiva or other injury. Age is inversely related to risk. 177 The success rate is lower in black Africans, people with previous ocular inflammation or vascularisation and children. 174 The commonest cause for failure of trabeculectomy is subconjunctival fibrosis 178 resulting in occlusion of the fistula with an encapsulated bleb, commonly known as the ‘ring of steel’. Various agents have been used to minimise scarring with mitomycin C (MMC) the most commonly used intra-operative agent. 5FU is commonly used to influence bleb morphology post operatively. Beta irradiation has also been used as an anti-scarring agent. 174 It may be particularly useful in developing countries due to the technical simplicity of application of the probe and lower cost.
MMC was first introduced in 1983 although its widespread use did not come until the 1990's. MMC's alkylating properties inhibit DNA replication and inhibit or kill fibroblasts in in-vitro and in-vivo models of trabeculectomy thus increasing the success rates of filtration surgery.175,179–181 MMC is typically administered intraoperatively in concentrations of 0.1–0.5 mg/mL for 1–5 minutes depending on personal surgical preference. The main concerns about MMC use revolve around the thinning of the conjunctiva overlying the guarded sclerostomy which may cause late bleb leaks, hypotony, bleb related infection and endophthalmitis. The Cochrane review of MMC use in filtering surgery 181 found the risk of cataract to be the only side effect significantly increased and failed to confirm many ophthalmologists’ anecdotal view of increased complications of hypotony and endophthalmitis. This may, in part, be due to low event rates and increasing success in preventing these complications being mindful of the potential risks inducing ever more meticulous care and attention when handling the conjunctiva and sclera.
Aqueous shunts
Aqueous shunts, also known as glaucoma drainage devices, tube implants and setons are alternatives to trabeculectomy surgery. Aqueous shunts have evolved over more than one hundred years and 4 main shunts are used in clinical practice today; Ahmed (New World Medical Inc., Rancho Cucamonga, CA), Baerveldt (Advanced Medical Optics, Inc Santa Ana, CA 250 mm2 and 3500 mm2 devices), Krupin (Eagle Vision Inc., Memphis TN) and Molteno (Molteno Ophthalmic Ltd., Dunedin, New Zealand, single and double plated devices).182,190
They follow the same biological principles using an explant plate sutured to the sclera, typically in the superotemporal part of the globe that when encapsulated provides a potential space into which aqueous can drain via a connecting silicone-rubber tube which is placed into the anterior chamber taking care not to abut the corneal endothelium or phakic lens. The devices differ in explant surface areas, shape, plate thickness, presence or absence of a valve and the absolute details of surgical implantation. 182 Aqueous flows from the eye through the tube to the encapsulated plate and then diffuses into the surrounding tissues by passive diffusion. 183
These shunts were traditionally thought not to be as effective as standard and augmented trabeculectomy 182 with typical IOPs of 18 mmHg vs. 14–16 mmHg and 8–10 mmHg respectively, however the recent Tube vs. Trabeculectomy study 184 challenges this with a mean IOP of 13 mmHg and IOP of 14 mmHg or less in 62% of patients at 3 years. They used a 350-mm2 Baerveldt shunt. It also reported fewer complications in the tube group compared with the MMC trabeculectomy group (39% vs. 60% respectively during the first 3 years of follow up P = 0.004) but more adjunctive medications at 1 year in the tube group however this had ceased to be statistically significant at 3 years. Cataract progression was similar in both groups at 3 years (58% Tube group vs. 57% Trabeculectomy group) Recently published expert opinion make the point that the complication rates of augmented trabeculectomy in the study were higher than other published data and the debate regarding superiority is ongoing. 244 Studies published before 2005 were included in the Cochrane review of aqueous shunts. 185 Comparative outcomes of current shunts remain insufficient to conclude that one device is more effective than another, but several studies indicate that devices with larger equatorial plates control IOP better than smaller plates.185,186 There is no definitive evidence to support the use of antifibrotic agents as adjuncts to aqueous shunt surgery.187,188
Aqueous shunts tend to be reserved for complicated cases of raised IOP, after pharmacotherapy, laser and filtering surgery has failed and in eyes with traumatic, inflammatory and neovascular glaucoma.182,185 Medicare data between 1995 and 2004 189 suggests a trend towards earlier and increased usage of aqueous shunts. This may in part be explained by increasing surgical familiarity and confidence in these devices to deliver lower IOP with fewer side effects.
The principal concept of non-penetrating glaucoma surgery (NPGS) is to create filtration through a naturally occurring membrane that acts as an outflow resistance site, allowing a progressive IOP drop and avoiding postoperative ocular hypotony. 191 The rate of aqueous drainage is controlled at the level of the trabecular meshwork and Descemet's membrane rather than a guarded sclerostomy. The proposed advantage of NPGS is that uncomplicated surgery is virtually an extraocular procedure 192 and some believe it to be safer than trabeculectomy with quicker visual recovery, less intraocular inflammation and is astigmatically neutral. 193 195 The basic premise underlying NPGS is that the greatest resistance to aqueous flow is at the juxtacanalicular trabecular meshwork and Schlemm's canal. The first published report was in 1964 when Krasnov196,197 described a procedure, (sinusostomy) which involved removing a lamellar band of the sclera thus opening up Schlemm's canal over 120 degrees. Various modifications then ensued until Fydorov stressed the importance of removing the corneal stroma behind the anterior trabeculum and Descemet's membrane calling it deep sclerectomy. 198
The two main NPGS procedures in current clinical use are Deep Sclerectomy (DS) and Viscocanalostomy.
Deep sclerectomy
DS involves making a 5 × 5 mm superficial scleral flap of approximately one third scleral thickness. A second scleral flap 4 × 4 mm beneath the original is then fashioned and removed to leave a residual scleral bed of 50–100 microns. Schlemm's canal is de-roofed in the most challenging part of the surgery due to the risk of inadvertent perforation of the anterior chamber or removing insufficient tissue in efforts to avoid perforation. Some surgeons then peel the Schlemm's canal endothelium and juxtacanalicular trabeculum membrane and this additional step corresponds to abexterno trabeculectomy. 198 The superficial scleral flap is then repositioned and sutured with or without an implant to help keep the scleral space open. After aqueous passage through the residual trabeculo-Descemet's membrane there are four hypothetical mechanisms for resorption; a subconjunctival filtering bleb, an intrascleral filtering bleb, a suprachoroidal filtering bleb and an episcleral vein outflow via Schlemm's canal. 198 200
Efficacy of deep sclerectomy
Clinical IOP lowering with deep sclerectomy without the adjunctive use of antimetabolite or implant has been reported as a mean drop of 50% at 46 months in a retrospective study on eyes newly diagnosed with POAG and no prior treatment to success rates of 61.4%, 36.6% and 18.9% at 21, 24 and 30 months respectively in a prospective study of 43 eyes where surgical success was deemed to be IOP of less than 22 mmHg and 20% reduction from baseline without the use of medication. 201
Recent evidence suggests that success rates are improved with antimetabolites and implants.192,198 Using an implant is thought to help maintan a low pressure intrascleral lake between the external scleral flap and trabecular meshwork acting as a spacer in the time of maximal healing and hence scar formation. In one RCT deep sclerectomy with implant (DSCI) achieved IOP of <21 mmHg without adjunctive medical treatment in 69.2% at 48 months vs. deep sclerectomy without implant (DS) 38.5%. The IOP at 48 months was 10 (±4 mmHg DSCI) compared with 16 ± 3.0 mmHg (DS) (P = 0.005). 201 Various authors report prospective and retrospective case series demonstrating enhanced success with the use of implants.198,202–204 however there are some comparative studies where implants have not improved success rates.192,205,206 Some discrepancy may be due to the confounding influence of using 5FU in the control group but not the DSCI group. Several commercially available implants have been developed (Aqua-flow collagen drainage device, T flux, SKGEL and PMMA implant) Interestingly, Ultrasound Biomicroscopy (UBM) performed 1 year after deep sclerectomy without implant demonstrates the presence of an intrascleral space in over 90% of cases 207 and the presence and volume of the intrascleral space correlates poorly with level of IOP.
Antiproliferatives and deep sclerectomy
Both 5FU and MMC have been used to try to augment the success rate of DS and both appear to increase success rates.205,206,208 An RCT of DS with and without MMC (0.2 mg/mL for 2.5 minutes) demonstrated a greater IOP reduction in the MMC group at 36 months (11.7 mmHg or 42.3% vs. 7.1 mmHg or 27.6% P = 0.05). 209 Neudorfer et al also reported an increased success rate210,211 however, Anand et al 212 report a RCT studying the effect of DS with low dose MMC in a Nigerian population and MMC did not deliver better IOP lowering and success rates were low in both groups (13% MMC DS vs. 24% DS at 18 months P = 0.5).
Comparing DS with trabeculectomy 213 217 is important as many specialist surgeons use one or other technique predominantly. Randomised controlled trials comparing NPGS to trabeculectomy213,218–222 suggest an improved safety profile of NPSG but are not in agreement when it comes to efficacy even in RCTs on paired eyes. El Sayyad et al 213 randomly assigned 39 patients to DS or trabeculectomy in the first eye followed by the opposite procedure in the fellow eye reporting mean postoperative IOP of 15.6 mmHg ± 4.2 DS group vs. 14.1 mmHg ± 4.6 in the trabeculectomy group; an IOP reduction of 44% and 50% respectively from baseline. Chiselita 214 in a similar study of 34 eyes in 17 patients found a statistically significant lower IOP in the trabeculectomy group throughout the 18 month follow up period (17.3 ± 1.2 mmHg vs. 20.9 ± 4.0 mmHg DS group) but with significantly fewer complications in the DS group. This reduced complication rate was echoed by Ambresin et al 216 who also reported similar success rates between DS and trabeculectomy. Cilino et al 215 found no significant difference in outcome between DS and trabeculectomy although the trend was towards lower IOP in the trabeculectomy group.
Viscocanalostomy
Stegmann et al described a variant of NPGS and termed it viscocanalostomy to emphasise the importance of injecting high viscosity sodium hyaluronate (Healon GV) into Schlemm's canal as a means of improving aqueous drainage. 223 In viscocanalostomy the superficial scleral flap is tightly sutured so that only aqueous regressing through trabeculo-Descemet's membrane can reach the two surgically created ostia of Schlemm's canal, travel circumferentially within the canal and enter the collector channel s and then the aqueous veins. In a post mortem eye model, injecting viscoelastic into Schlemm's canal enlarged its area adjacent to and 6 mm from the flap significantly more than if it was not injected. 224 In vivo primate 225 and human eye 223 studies show that not only is Schlemm's canal dilated but so too are the collector channels and there is disruption of the inner wall endothelium of the canal with disorganisation of the juxtacanalicular zone resulting in direct communication of the juxtacanalicular space with the lumen of Schlemm's canal. This may enhance conventional aqueous outflow. 223 Disruption of the posterior wall of Schlemm's canal may also allow direct communication between the lumen and the ciliary body thus potentiating uveoscleral outflow. The viscoelastic material is also postulated to have an anti- inflammatory effect and may inhibit cellular migration, phagocytosis and cytokine production thus interfering with wound healing. 198
Stegmann reported the results of viscocanalastomy in 214 eyes from 157 black African patients with average follow up time of 35 months. 223 82.7% of eyes achieved an IOP of 22 mmHg or less without medical therapy and an average IOP reduction of 64% with few complications. In the mainly caucasian series of Sunaric-Megevand and Leuenberger the mean IOP reduction was 38.3% with complete success in 68% at 1 year, 60% at 2 years and 59% at 3 years. 226 Yarangameli et al 227 compared a prospective group undergoing viscocanalostomy with MMC with a retrospective viscocanalostomy alone group and reported no statistically significant difference in IOP although they observed a trend towards more IOP reduction and higher success rate in the MMC group. A prospective RCT of viscocanalostomy with and without the SKGEL implant found 40% success rate at 1 year in both groups (IOP < 22 mmHg and no medication) with equally low complication rates. 228
Viscocanalostomy compared with trabeculectomy
O'Brart et al conducted 2 RCTs one comparing MMC trabeculectomy with standard viscocanalostomy and the other comparing augmented trabeculectomy with augmented viscocanalostomy.220,221 In the RCT of 50 eyes from 48 POAG patients randomised to MMC augmented trabeculectomy or standard viscocanalostomy 100% of eyes in the trabeculectomy group achieved IOP < 21 mmHg at one year compared with 64% in the viscocanalostomy group (P < 0.001) The trabeculectomy group however had significantly more postoperative interventions (64% vs. 23% in the viscocanalostomy group) When both procedures were augmented success rates were 68% in the MMC trabeculectomy group vs. 34% in the MMC viscocanalostomy group after mean follow up 1 year. Most of the evidence suggests that augmented viscocanalostomy tends not to achieve the same IOP reduction as MMC augmented trabeculectomy but does result in fewer complications.218–222,227,228 However, Mendrinos et al in their review on NPGS make the point that there is a significant learning curve to NPGS and one cannot compare one's first few cases of NPGS to their last few cases of trabeculectomy. 198
There are some studies using laser assisted ablation of deep scleral tissues and this step is generally felt to be the most difficult to do successfully. An erbium-YAG laser has a wavelength near the maximum absorption of water hence the ablation depth is self-limited by the percolation of aqueous and may reduce the risk of inadvertent anterior chamber perforation. 229 Excimer and CO2 lasers have also been tested experimentally and may be viable. 198
NPGS continues to evolve and IOP lowering appears to have improved with modifications in technique just as trabeculectomy and aqueous shunt surgery have however the degree and longevity of IOP lowering between augmented trabeculectomy and NPGS are still uncertain.
Novel Glaucoma Procedures
The American Academy of Ophthalmology recently issued a report summarising the exciting new developments in surgical procedures for IOP lowering. 230 These have FDA approval or are currently in phase III clinical trials in the USA. The majority of novel procedures seek to avoid bleb formation and its associated disadvantages and instead rely on augmentation of the physiological outflow pathways. There are three main categories of new devices; (1) increasing outflow by creating a new outflow channel) Ex-PRESS glaucoma implant (Alcon, Inc., Hunenberg, Switzerland) 247 251 and Fugo blade transciliary filtration (Medisurg Ltd., Norristown, PA);252,253 (2) augment the conventional (trabecular meshwork) pathway, trabecular bypass stent (iStent, Glaukos Corporation, Laguna Hills, CA), 254 256 trabeculectomy by internal approach with the Trabectome (NeoMedix, Inc., Tustin, CA) 257 259 Fugo blade goniotomy, 260 excimer laser trabeculoplasty (AIDA, Glautec AG Nurnberg, Germany)261,262 and canaloplasty (iScience Interventional Corp., Menlo Park, CA) 263 265 and (3)enhancing uveoscleral flow, the SOLX Gold Shunt (SOLX Ltd., Boston, MA). 266 268
Conclusions
The ideal scenario in clinical IOP lowering would be a cost effective procedure or pharmacological agent which lowered IOP significantly and predictably with minimum side effects or complications and minimal reliance on adherence and persistence with treatment regimes. This review comments on current clinical options for IOP lowering and there is no doubt that refinement and modifications of existing medical and surgical options have provided better IOP lowering for patients but continued innovation and pursuit of the perfect ocular hypotensive are to be encouraged.
Author Contributions
Wrote the first draft of the manuscript: LC. Contributed to the writing of the manuscript: SZ, MC, LG. Agree with manuscript results and conclusions: MC, LG. Jointly developed the structure and arguments for the paper: LC, MC, LG. Made critical revisions and approved final version: MC, LG. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.