
Abstract
Purpose:
The aim of this study was to compare the intraocular pressure measurements obtained from healthy subjects with the rebound tonometry, non-contact airpuff tonometry, and Goldmann applanation tonometry in different age groups.
Methods:
A total of 180 eyes of 90 healthy subjects were included in the study. According to the subjects’ ages, the eyes were categorized into three groups: group 1 (age: 7–17 years), group 2 (age: 18–40 years), and group 3 (age: 41–75 years). Intraocular pressure was measured on each subject always in the same order: rebound tonometry, non-contact airpuff tonometry, and Goldmann applanation tonometry. Central corneal thickness values were obtained using ultrasonic pachymetry. One-way repeated-measures analysis of variance, Pearson’s correlation coefficient, and Bland–Altman analysis were used for the statistical assessment.
Results:
The mean corneal thickness was found to be 604 ± 13 µm, 546 ± 15 µm, and 547 ± 15 µm in group 1, group 2, and group 3, respectively. Non-contact airpuff tonometry was significantly higher than both Goldmann applanation tonometry and rebound tonometry measurements in all groups (p < 0.001, for all). No statistical difference between Goldmann applanation tonometry and rebound tonometry measurements was found in group 1 (p = 0.248), group 2 (p = 0.63), and group 3 (p = 0.126). There was a significant positive correlation in the meaning of intraocular pressure measurements between rebound tonometry and non-contact airpuff tonometry; non-contact airpuff tonometry and Goldmann applanation tonometry; and Goldmann applanation tonometry and rebound tonometry in all groups.
Conclusion:
As a result, without need for topical anesthesia, fast measurement and ease-of-use rebound tonometry is a reliable alternative to Goldmann applanation tonometry in different age groups.
Introduction
Glaucoma is the most common cause of irreversible blindness worldwide. In 2020, more than 11 million individuals are expected to have bilateral blindness. 1 Glaucoma is diagnosed by evaluating all factors such as intraocular pressure (IOP), cupping of the optic nerve head, corneal thickness, thinning of the retinal nerve fiber layer (RNFL), and changes in the visual field. 2 Although IOP is not included in the definition of glaucoma, increased IOP is the most important and the only risk factor that can be changed and slowed or stopped the progress of the disease when it is lowered. 3
Therefore, one of the most important steps of the routine examination for early diagnosis is to measure the IOP correctly in order to detect glaucoma patients, most of whom are asymptomatic. Since the invention of the first tonometry according to the Goldmann Imbert-Fick principles, Goldmann applanation tonometry (GAT) has been accepted as the international gold standard measurement method. 4 Non-contact airpuff tonometer (NCT) is used in the routine patient examination, even though GAT is accepted as the gold standard. NCT was first designed by Zeiss and developed by Grolman in 1972. It measures the IOP without touching the corneal surface and therefore does not increase risk of infection and does not require anesthesia or fluorescein drop.5,6 The rebound tonometer (RT; I-Care; Tiolat Oy, Helsinki, Finland) is a new player in the field of IOP measurement instruments. There is a magnetized probe that moves quickly toward the eye. A solenoid detects the acceleration and deceleration of the probe. Topical anesthesia is not required for measurements with RT, such as NCT, and the risk of spreading infection is considered negligible due to the use of disposable probes. 7
The purpose of this study is to compare RT and NCT measurements with the reference method GAT in the eyes of different age groups including healthy subjects.
Methods
This protocol was carried out at Medipol University’s Vatan Health Practice Center following the 1964 Helsinki Declaration, following approval from the ethics committee of the Istanbul Medipol University (10840098-604.01.01-E.12581) and the approval of research participation from eligible healthy subjects.
A total of 180 eyes of 90 healthy subjects were included in the study. Subjects with any history of ocular disease affecting IOP, astigmatism greater than 2 diopters, contact lens use (within the 2-week period prior to IOP measurement), previous ocular surgery or trauma, ocular inflammation, family history of glaucoma, classical glaucomatous optic disk changes as focal or diffuse thinning of the RNFL with consistent glaucomatous visual field defects were excluded from the study. Glaucomatous visual field defects were confirmed if two of the following three conditions were met: presence of a cluster of three points on a pattern deviation probability plot with p < 5%, one of which had p < 1%; a pattern standard deviation with p < 5%; or a glaucoma hemifield test result outside normal limits. To avoid the double-organ bias, the mean measurements of two eyes of one subject were used for statistical analysis. According to the subjects’ ages, the eyes were categorized into three groups: group 1 (age: 7–17 years), group 2 (age: 18–40 years), and group 3 (age: 41–75 years). Subjects below 18 years were accepted as pediatric group. From literature, we know that subjects older than 40 years are at risk of glaucoma that is why those were arranged as a separate group. The subjects aged between 18 and 39 years formed the other group.
Central corneal thickness measurements
Central corneal thickness (CCT) values were obtained by ultrasonic pachymeter (AccuPach VI; Keeler, Malvern, PA, USA) before IOP measurements. After one drop of 0.5% proparacaine hydrochloride eye drops (Alcaine®; Alcon Laboratories Inc., Fort Worth, TX, USA), the pachymeter probe was placed on the center of the cornea, and the mean of three readings was calculated for each eye.
IOP measurements
The IOP values were obtained by RT, NCT, and GAT, respectively. Each of the tonometers was calibrated according to the manufacturer’s guidelines prior to its use. There was a 15-minute interval between measurements. IOP measurements were made by the same doctor (G.D). The RT (I-Care 100; Tiolat Oy) was positioned near the subject’s eye with the forehead being used as a base support. IOP measurements were taken with the tip of the probe maintained at a distance of approximately 3 to 7 mm from the center of the cornea, according to the manufacturer’s instructions. The mean of six consecutive sets of acceptable final measurements was used for subsequent analyses. The measurements with RT were made first in sitting position and after 15 minutes in dorsal decubitus. The NCT (Topcon CT-80; Topcon Corporation, Tokyo, Japan) automatically recorded three IOP readings, with their average per eye being recorded for the study. The GAT (Haag-Streit, Koeniz, Switzerland) values were recorded after three consecutive readings and a mean value was calculated for each eye observed. Before acquisition, one drop of 0.5% proparacaine hydrochloride eye drops (Alcaine®; Alcon Laboratories Inc.) was instilled and a fluorescein strip (Fluorescein Sodium Ophthalmic Strip; Optitech Eyecare, Allahabad, India) was applied to the inferior conjunctival fornix. The last IOP measurement was obtained using GAT to avoid a corneal-compression-induced aqueous outflow increase that would have affected subsequent IOP readings.
Statistical method
Statistical analysis was performed with Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, USA). The normality of the continuous variables was evaluated with the Shapiro–Wilk test. Intraclass correlation coefficient (ICC) test was done before taking average measurements of two eyes. Because ICC was close to 1, the average of measurements from two eyes of a subject was used. The differences between IOP readings were compared with the one-way repeated-measures analysis of variance (ANOVA). The relationship among three devices in the meanings of IOP readings was evaluated by Pearson’s correlation coefficient. Bland–Altman analysis was used to assess the clinical agreement of IOP measurements between the tonometers. Values of p lower than 0.05 were considered as statistically significant.
Results
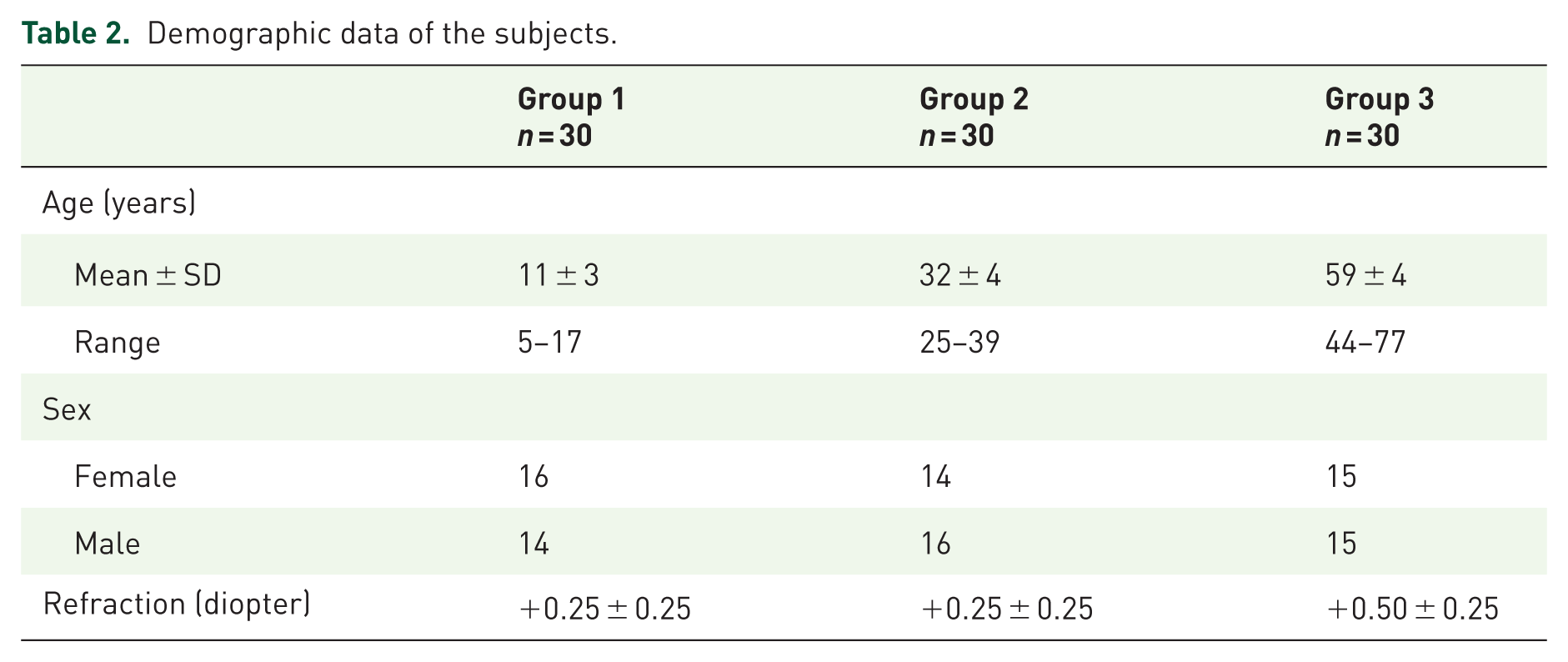
The normality of the continuous variables was evaluated with the Shapiro–Wilk test (Table 1). Demographic data of the all subjects are given in Table 2. When study groups were analyzed, the mean corneal thickness was found to be 604 ± 13 µm, 546 ± 15 µm, and 547 ± 15 µm in group 1, group 2, and group 3, respectively. The mean corneal thickness was significantly higher in group 1 compared with groups 2 and 3 (p < 0.001 for both). There was no significant difference in corneal thickness between groups 2 and 3 (p = 1.000). The NCT measurements were significantly higher than both GAT and RT measurements in all groups (p < 0.001, for all). No statistical difference between GAT and RT measurements was found in group 1 (p = 0.248), group 2 (p = 0.63), and group 3 (p = 0.126). Comparison of IOP measurements obtained by RT, NCT, and GAT among three groups is shown in Table 3. There was a significant positive correlation in the meaning of IOP measurements between RT and NCT; NCT and GAT; and GAT and RT in all groups (Table 4). The mean ± SD differences and 95% limits of agreement between RT, NCT, and GAT are shown in Table 5.
Shapiro–Wilk test normality results of the continuous variables.

IOP: intraocular pressure; RT: rebound tonometry; NCT: non-contact tonometry; GAT: Goldmann applanation tonometry.
Demographic data of the subjects.
Comparison of intraocular pressure measurements obtained by RT, NCT, and GAT among three groups.

RT: rebound tonometry; NCT: non-contact tonometry; GAT: Goldmann applanation tonometry.
One-way ANOVA post hoc Bonferroni test.
Correlation analysis of three devices in all groups.

RT: rebound tonometry; NCT: non-contact tonometry; GAT: Goldmann applanation tonometry.
Pearson’s correlation coefficient.
Results of Bland–Altman analyses of the agreement between RT, NCT, and GAT.

RT: rebound tonometry; NCT: non-contact tonometry; GAT: Goldmann applanation tonometry; LoA: limits of agreement.
Discussion
Glaucoma is the most common cause of blindness after cataract in the world. 8 Glaucoma treatment is aimed at slowing or stopping the disease. Today, glaucoma drugs do this by lowering IOP. Therefore, the correct IOP measurement is one of the most important parameters of the eye examination. The most precise measurement is to measure with a manometer by placing a cannula in the anterior chamber, although not in clinical practice. 9 For this reason, GAT is accepted as the international gold standard today. 4 However, the GAT is also affected by the examiner experience, CCT, corneal slope, and axial length.10,11 It is also important to keep in mind the risk of spreading infection and using smooth and not cracked prism.12,13 In this study, GAT was used as reference measurement method.
The RT was discovered by Obbink 60 years ago. 14 In principle, IOP was found by measuring impact time of the probe that strikes the cornea. The higher the IOP, the shorter the probe’s stroke time. There are various studies showing that they are affected or not affected according to CCT.15,16 The exact advantages are cheapness, easiness, convenience, portability, and fastness. The exact advantages to GAT are that it does not require an experienced ophthalmologist, painless, no anesthesia, and no risk of infection. 17 Abraham and colleagues 7 showed that there is no difference between the experienced and inexperienced technicians of I-Care measurements. No side-effects were observed in any study. Some investigators have shown that the I-Care tonometry results in high CCT cases had high IOP readings.15,18,19 Fernandes and colleagues 20 have shown that I-Care tonometry in the normal population produces an average of 1.34 mmHg higher results than GAT. I-Care measurements were found to be higher in the studies in which the results of the measurements taken from pediatric cases were compared with those in the GAT.21,22 In another similar study, I-Care had a significantly lower measurements. 23 Brusini and colleagues 24 have shown that the I-Care tonometry is a suitable measurement method for screening healthy individuals. Kim and colleagues 25 have shown that I-Care measurements are independent of age, axial length, and CCT parameters. Khanal and colleagues 26 found very similar results with I-Care tonometry in different quadrants of cornea in their study. Thus, they explained that measurements of I-Care tonometry were not affected by corneal thickness.
However, Feng and colleagues 27 showed that there were significantly different results taken between NCT, RT, and GAT in a large series of pediatric patients. They observed the highest values with NCT and the lowest values with GAT. They also found that all types of tonometry measurements correlated with CCT. They showed that the CCT affected all types of tonometer measurements. When the whole pediatric group was examined, 93% of cases with NCT, 85% of patients with RT, and 77% of patients with GAT could be measured. This study emphasized the necessity of NCT and RT to measure IOP due to compliance in the pediatric group. We found the highest values with NCT similar to this study but we found similar values in RT and GAT measurements.
Some studies have investigated the effects of topical anesthetic drugs on corneal thickness and IOP measurements.28,29 Rosa and colleagues 28 showed that oxybuprocaine eye drops had no significant effect on corneal volume and CCT measurements. Lam and Chen 29 also observed that there was no significant effect on CCT measurements with proparacaine eye drops. For these reasons, we did not take into account the effect of local anesthetic drops on CCT in our study.
NCTs provide air application without touching the eye. After the beginning, air force increases until the cornea is flattened. Then, the tonometer transforms the power of applanation to IOP. There are measurement problems compared to similar corneal pathologies such as GAT. 30 Ogbuehi 31 showed that NCT performed reliable and similar measurements with GAT. Tonnu and colleagues 30 have shown that NCT, Tono-Pen XL, and GAT measurements were influenced by CCT. Shields 32 have shown that the reliability of NCT in high IOP cases is reduced. A study, comparing RT and GAT, found mean IOP measurements 14.3 ± 3.9 mmHg and 11.7 ± 4.7 mm Hg using GAT and RT, respectively. 33 Similar to our study, RT measurements were lower than GAT measurements.
Limitations of this study are small sample size and lack of glaucomatous subjects.
Conclusion
The measurements from the three different age groups with RT were found to be consistent with GAT measurements. The NCT measurements were significantly higher than those obtained by GAT. It can be concluded that RT is a reliable alternative for screening healthy subjects for whom GAT is difficult to implement. However, it is necessary to take into consideration that RT measurements are slightly lower than GAT measurements.