
Abstract
Background
Post-traumatic neuropathic pain is a therapeutic challenge in everyday practice. The craniofacial region is no stranger to this reality and can present complex symptoms in areas of trigeminal sensitivity with a significant impact on quality of life.
Case
We present the first report of perineural botulinum toxin injection with ultrasound guidance in the trigeminal innervation for the management of post-traumatic pain.
Conclusion
The patient experienced an objective improvement in symptoms, an improvement in quality of life, and a return to work without any secondary events resulting from the intervention.
This is a visual representation of the abstract.
Introduction
Post-traumatic neuropathy occurs as a result of disruption of the peripheral nervous system caused by a mechanical, chemical, or thermal injury. Resulting in signs and symptoms of neuropathic pain such as allodynia, hyperalgesia, and hyperpathia, which will occur in the area innervated by the affected nerve. 1 In the trigeminal nerve (cranial nerve V), traumatic trigeminal neuropathy (TTN) occurs in 1,5–13% of patients, 2 with trigeminal neuralgia due to non-traumatic causes (tumor compression, vascular compression, or post-herpetic infection) being more common.3,4 Traumatic trigeminal nerve injuries have been described mainly in the iatrogenic context of dental surgery or procedures and maxillofacial fractures.3,4
Regardless of the cause of trigeminal neuropathic pain, one treatment that promises to be effective, safe, and therapeutic in the medium term is the application of botulinum toxin. Although there have been no extensive studies, reports indicate positive outcomes.2,4 This drug, purified from Clostridium botulinum neurotoxin, has been used in neurological conditions such as spasticity, dystonia, and abnormal movements, among others, thanks to its effect of inhibiting the release of acetylcholine at the neuromuscular junction. 4 It also has an analgesic effect, inhibiting presynaptic release in the sensory fibers of pain mediators such as CGRP, substance P, and glutamate.4,5 Its use in neuropathic pain has increased, still being an off-label indication, but with growing evidence.
The most widely described and used technique for trigeminal neuropathic pain is subcutaneous application, after creating a grid with 1 cm2 squares, applying 5 to 10 units of toxin in each square according to anatomical landmarks, with a total dose of between 100 and 200 units. In addition to these approaches, other techniques have been described that have shown good results, such as intraoral, intramuscular, and even sphenopalatine ganglion application. 6
Due to the diversity of the approaches described and the lack of standardization of a specific approach, there has been growing interest in applying botulinum toxin for neuropathic pain using an ultrasound-guided perineural approach. This technique has proven to be effective and safe in cases of post-traumatic headache and peripheral and post-traumatic neuropathies.5,7,8 Although previous reports suggest the use of anatomical landmarks to locate the infraorbital nerve, there is a risk of puncturing the infraorbital artery or facial artery, as well as the possibility of intramuscular injection. Therefore, the use of ultrasound guidance not only allows for precision in the injection but also reduces the risk of potential adverse events. There are no reports of perineural application of botulinum toxin for the management of neuropathic pain due to TTN, this is the first case with a successful outcome using this technique.
Clinical case
We present the case of a 34-year-old patient who suffered facial trauma, predominantly to the left side of his face, while performing his work duties. He was initially referred to the emergency department, where a CT scan revealed an aligned fracture of the left frontal bone compromising the anterior wall of the left frontal sinus, as well as a displaced fracture of the medial wall of the left orbital cavity and the walls of the ethmoid cells.
He was evaluated by the ophthalmology department, which ruled out any involvement of the eye or optic nerve. After that, plastic surgery and maxillofacial surgery performed an initial surgical intervention to repair the skin and soft tissues, but without the use of osteosynthesis material. He was discharged with COX 2-based anti-inflammatory treatment for two weeks. Follow-up by maxillofacial surgery revealed adequate healing of his fractures; however, the patient presented with neuropathic pain in the facial area, described as paroxysmal electric shocks with distension predominantly in the lower region of the eye socket towards the nose and in the zygomatic region. He was initially treated with pregabalin 50 mg twice daily and acetaminophen, with only a 10% improvement in symptoms, in addition to reporting limitations in his daily activities and difficulty sleeping due to pain.
The patient is referred to our pain medicine service for complementary treatment. Neuropathic pain was found in the left trigeminal region, predominantly in the sensitive area of the infraorbital nerve. Analgesic management was initiated with pregabalin 150 mg daily, acetaminophen with caffeine 500/65 mg, and topical 5% lidocaine patches in the infraorbital area. With this treatment, the patient experienced a 20% improvement in symptoms, with increased pain during daily activities and no resolution of pain at night. An ultrasound-guided infraorbital nerve block was considered. For the intervention, a Vscan Air GE linear transducer of 3–12 MHz was used, and a plane approach was performed at the level of the left infraorbital nerve emergence, applying 1 ml of 0.25% bupivacaine + 1 mg of betamethasone. With this intervention, the patient reported a 90% improvement in symptoms for 60 days. There was a significant improvement in nighttime pain and pain during activities, in addition to resolving the dysesthesia.
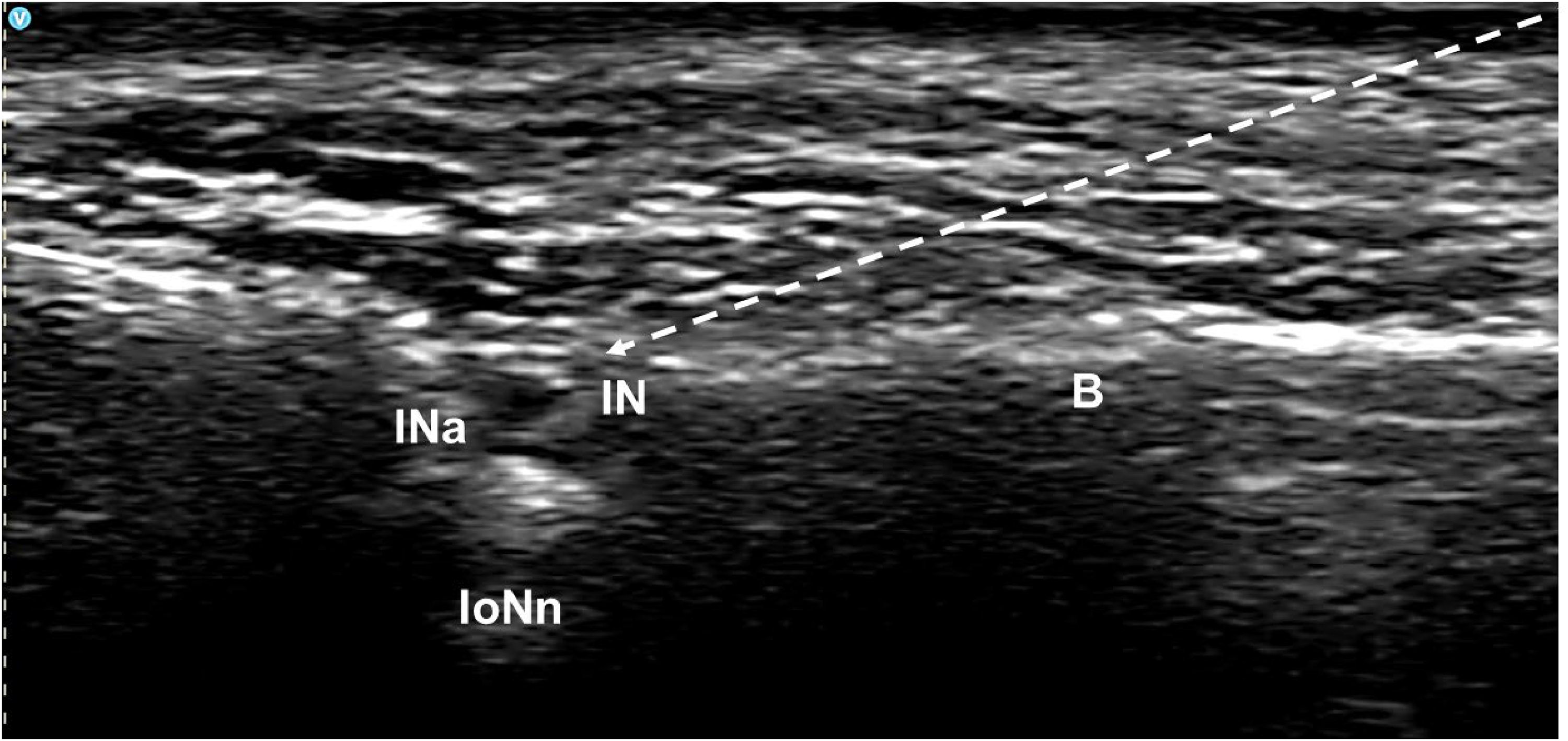
At the 90-day follow-up, the patient continued to use pregabalin and acetaminophen with caffeine but reported a recurrence of pain at approximately 70% of the initial intensity. Radiofrequency intervention was discussed with his maxillofacial surgeon, but due to the type of trauma and surgical approach, they considered that this type of treatment would not be appropriate. A second infraorbital nerve block was performed following the same guidelines as the first, with only a 40% improvement in symptoms for 30 days and a recurrence of pain. At the follow-up appointment after 4 weeks, based on the persistence of pain, it was decided to perform a perineural application of botulinum toxin (Onabotulinumtoxin A). Using the same approach as for the block (Figure 1), 10 IU of botulinum toxin was applied to the infraorbital nerve emergence, in a dilution of 10 U/ml, for a total volume of 1 ml. With this intervention, the patient reported an 80% improvement in symptoms with complete resolution of dysesthesia.
We performed follow-up visits on 30, 60, 90, 120 and 180 days, where sustained improvement in pain was reported. The patient continued his pharmacological management and was able to return to work. No additional surgical interventions or pain management were necessary. A significant improvement was found in the patient's sleep pattern and daily activities, with no episodes of pain and the ability to wash his face daily, apply sunscreen, and touch his skin without pain.
Discussion
TTN represents a clinical and therapeutic challenge due to the limited efficacy of currently available pharmacological treatments.1,3,4 In the reported case, maxillofacial trauma caused the patient neuropathic pain that was difficult to manage, as first-line pharmacological treatment failed to control the symptoms, requiring ultrasound-guided infraorbital nerve block. The satisfactory response to the block confirmed the neuropathic component, although pain relief was short-lived (60 days) and recurred. In cases such as this, it is necessary to evaluate alternatives that allow for longer analgesic duration, especially if radiofrequency is not a viable option. For these cases, botulinum toxin type A emerges as an effective and safe treatment. 1 3–5
This therapeutic option, although not first-line and with a poorly evaluated indication for neuropathic pain management, has shown benefit in trigeminal neuropathic pain. Hu et al. (2024) conducted a meta-analysis that included 23 studies, four of which were randomized clinical trials, to evaluate the response to the use of botulinum toxin for the management of trigeminal neuralgia, finding an average reduction of 4 points on the visual analog scale of pain and a favorable response rate in 70% of the patients evaluated, with a therapeutic effect lasting up to 6 months. 4 In the case of the reported patient, follow-up was performed for up to 4 months, and the analgesic effect was sustained until this time, which is consistent with the results of this study.
Another meta-analysis published in 2019 by Wei et al., which included 10 randomized clinical trials comparing the efficacy of botulinum toxin with placebo in a total of 391 participants with trigeminal neuralgia and peripheral neuropathy, found that to achieve a 50% improvement in neuropathic pain, the number needed to treat TTN was 1.9 to 3.3, with an excellent safety profile and a minimal rate of adverse effects. 7 In this case, there were no adverse effects, which corroborates the safety of the treatment demonstrated in the studies.
Unlike most approaches described in the literature for the management of neuropathic pain (subcutaneous or intradermal distribution in a grid pattern), perineural application under ultrasound guidance allows for more precise placement of the toxin around the affected nerve, optimizing its local concentration and reducing diffusion to adjacent tissues.5–8 This approach has been described to date in case reports and case series for other painful conditions, such as post-traumatic headaches and peripheral neuropathies, this being the first case reported for the management of TTN. In the case presented, a single application of 10 IU of perineural Onabotulinumtoxin A produced a sustained improvement of more than 80% for more than 180 days, with complete resolution of positive neuropathic symptoms and allowing the patient to return to work.
Although evidence has shown a lasting analgesic effect of up to 6 months, studies such as that by Tan et al. found an average analgesic effect of 3 months using subcutaneous grid application, which is the most commonly used method. 1 The ultrasound-guided perineural approach described in this case is novel and suggests a prolonged duration of the analgesic effect, possibly because botulinum toxin acts directly on the peripheral nerve. Additionally, we believe that a more localized application avoids multiple subcutaneous injections, improving patient tolerance and satisfaction with the procedure. However, as this is a case report, there is insufficient certainty to issue a specific recommendation, and a more extensive evaluation is required for its implementation in daily practice.
The long-term effect is considered secondary to the application of botulinum toxin. When applied to the muscle, an effect lasting at least 12 weeks can be expected, but in perineural application for neuropathic pain, not only is the typical action on the SNARE complex generated, but transient potential receptors are also modified, in addition to generating an antidromic effect on sensory perception, which may explain the patient's clinical evolution.9,10
In conclusion, to our knowledge, this case constitutes the first report of ultrasound-guided perineural application of botulinum toxin type A in post-traumatic trigeminal neuropathy, with successful and sustained clinical results. Although evidence shows that the use of this medication is effective under the currently described methods of application, it is necessary to evaluate the perineural technique mentioned in this case report with controlled studies to define the optimal dosage, technique, and frequency. Additionally, this case supports its consideration as an intermediate therapeutic option before ablative or neurosurgical procedures, within a multimodal and personalized approach to craniofacial neuropathic pain.
Key findings
The use of perineural botulinum toxin may be useful in the management of neuropathic pain.
Traumatic craniofacial pain of trigeminal origin may improve with the application of botulinum toxin.
Footnotes
Acknowledgments
This article is based on the CARE checklist for clinical cases.
Ethical considerations
This study was granted approval by the ethics committee at IPS Fundalivio.
Consent to participate
The patient consented to the performance of the procedures described and to the use of his or her clinical information in this article. Informed consent was obtained.
Consent for publishing
Yes, the authors agree to publish with Cephalalgia Reports
Author contributions
LAG wrote the article and performed the clinical intervention.
JMM wrote the article and did the research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All available information is included in the article.