
Abstract
Background
Migraine is a prevalent neurological disorder in sub-Saharan Africa (SSA). Despite its significant burden, migraine care in SSA faces numerous challenges. Healthcare services are limited, with primary care providers often lacking specialized knowledge in headache disorders. The scarcity of neurologists exacerbates the issue, leading to inadequate diagnosis and treatment. Public awareness about migraine is low, and social stigmatization further hinders effective care. Essential medications for migraine are often unavailable or unaffordable, and traditional medicine is frequently used as an alternative.
Objectives
This narrative review highlights the barriers to migraine care in SSA, including limited access to specialists, inadequate training of primary care providers, and the high cost of treatment. It also discusses the availability and use of evidence-based treatments, the role of traditional medicine, and the importance of public awareness and education.
Methods
A literature search was conducted on PubMed, Google Scholar, and Web of Science to identify papers on migraine epidemiology in SSA, access to care and treatment.
Conclusion
The article proposes strategic interventions to improve migraine care, such as enhancing education and training for healthcare providers, developing Africa-specific clinical guidelines, integrating traditional medicine with conventional care, and leveraging digital health solutions. By addressing these challenges, SSA can improve migraine care and reduce the associated disability.
This is a visual representation of the abstract.
Introduction
Migraine is a neurological disorder characterized by recurrent pulsating headaches, typically unilateral, with moderate to severe intensity, and is accompanied by symptoms such as nausea and vomiting.1,2 It is the third most burdensome neurological condition worldwide. Data from the Global Burden of Disease survey revealed that between 1990 and 2021 the global prevalence of migraine increased by only 1.6%, however, the absolute burden is substantial, particularly in certain regions, with highest rates of age-standardized DALYs (Disability-Adjusted Life Years) reported in eastern and central sub-Saharan Africa (SSA).3,4 Migraine affects approximately 10–15% of African populations, with higher rates among women.5,6

National/community-based health insurance scheme availability across sub-Saharan Africa (SSA).
Migraine medication availability in Essential Medicines Lists across SSA countries.

EML: Essential Medicines List; SSA: sub-Saharan Africa.
Availability of acute and preventive medications on the EML of select countries in SSA and their reimbursement status by the NHI schemes.
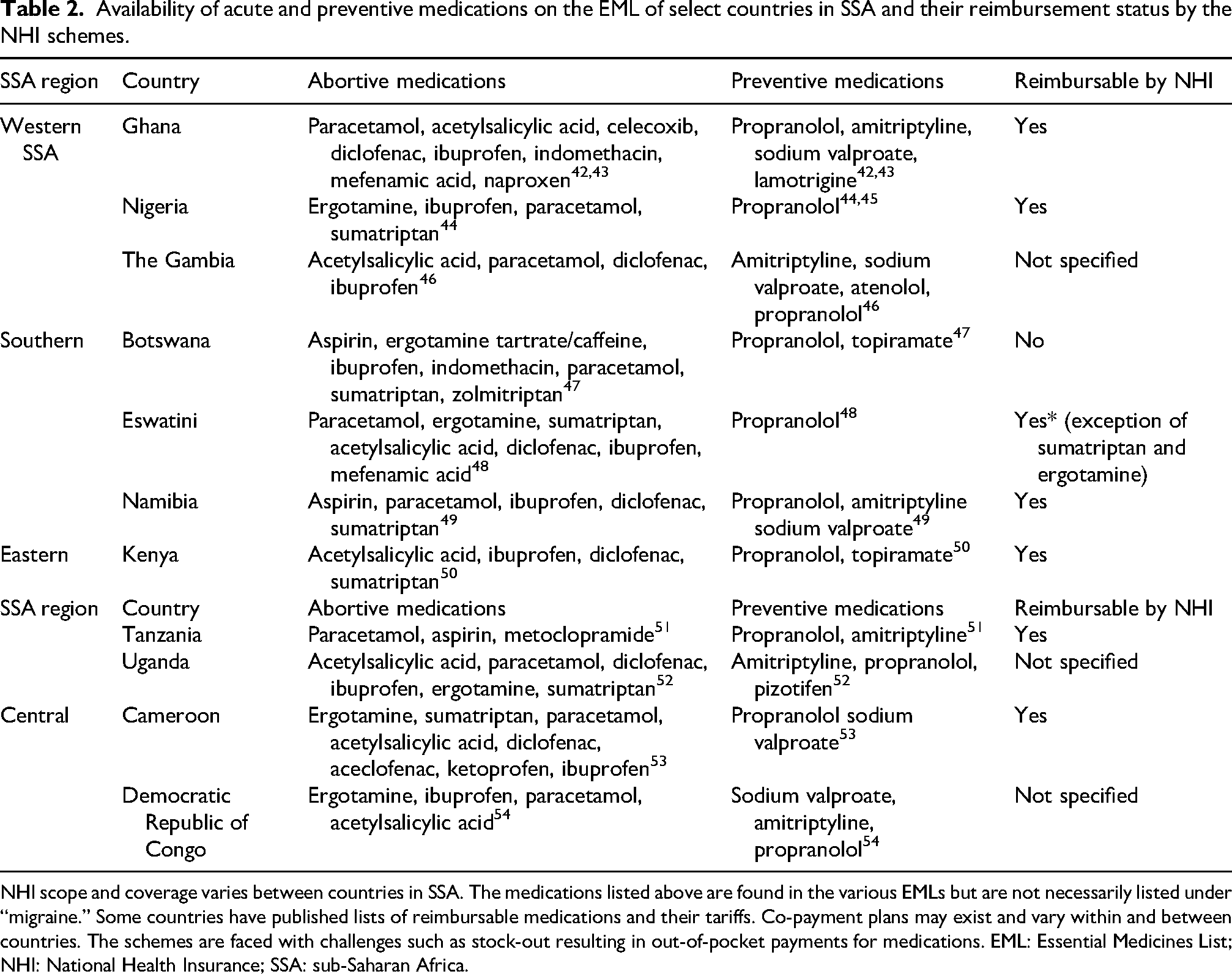
NHI scope and coverage varies between countries in SSA. The medications listed above are found in the various EMLs but are not necessarily listed under “migraine.” Some countries have published lists of reimbursable medications and their tariffs. Co-payment plans may exist and vary within and between countries. The schemes are faced with challenges such as stock-out resulting in out-of-pocket payments for medications. EML: Essential Medicines List; NHI: National Health Insurance; SSA: sub-Saharan Africa.
Organization of services
Healthcare services for migraine in SSA are limited. The setup of the healthcare system in SSA is a combination of public health services, private services and informal/traditional services. Care is primarily provided by nonspecialized medical doctors or clinical officers/physician assistants nurses, pharmacists, and traditional healers with limited access to specialists like neurologists. 7 In some countries traditional medicine services (mostly herbal medicine) are incorporated into primary healthcare. Despite the access to some level of care, there is a significant gap between the prevalence of migraine and the availability of specialized care. 8 Healthcare financing varies across the region. Some countries provide some level of free basic healthcare to all citizens de novo or through a Community-based Health Insurance (CBHI) or a National Health Insurance (NHI) service requiring payment of premiums (Figure 1). These schemes may be free to enroll on for some category of the population, for example, pregnant women, children under 5 years and the elderly.
Barriers to care
There are inadequate numbers of neurologists in SSA. The World Health Organization (WHO) recommends a ratio of 1 neurologist per 100,000 people, however, in many SSA countries, this ratio is far lower.9–11 On average there are 0.3 neurologists per million people. In the 2017 Global Health Observatory by the WHO, Togo was reported to have 0.14 neurologist per 100,000 population while Switzerland had as high as 13 per 100,000. 11 Some countries have no neurologists. 12
Even more dire is the scarcity of pediatric neurologists. According to a survey by Wilmshurst et al., 13 for the population of 1.37 billion in the continent of Africa, their survey revealed 324 child neurologists, equating to a median of 0.01 per 100,000 population in comparison with a median of 0.59 child neurologists per 100,000 across high-income countries.
Worldwide, neurology is considered a challenging discipline by a significant number of medical students, internal medicine residents, and specialists in other disciplines.12,14 SSA is no different. This perception has contributed to few neurologists being trained in the region. Skilled migration further drains locally trained specialists. 13 The workload of the few neurologists available impacts their ability to teach and supervise nonspecialists. It also impacts on their time for research and publications. This may account for the scarcity of data on migraine from the region. 15 Many of these neurologists are based in urban regions depriving rural folk of access to specialists. 16 With the increasing burden of neurological disorders on the African continent, strokes, epilepsy and infectious diseases with related CNS manifestations make up majority of cases seen in the neurology outpatient departments, often with long waiting periods at these centers to see neurologists.17–20 There are often no dedicated headache clinics in these settings. This may be a driving force for patients seeking alternative relief for their headaches.
Community health workers, general practitioners, and physician assistants/clinical officers often provide primary care for neurological conditions, including headaches. 21 There is often limited knowledge of the different headache disorders among primary care providers. A study conducted in Burkina Faso found that general practitioners in the hospital districts of Ouagadougou had varying levels of knowledge, attitudes, and practices regarding migraine management. 22 This lack of adequate knowledge can be a significant barrier to proper diagnosis and treatment. 23 Patients may be referred to regional, district, or tertiary facilities if they are not lost to follow up at these peripheral centers. 24 Access to neuroimaging (computed tomography (CT) and magnetic resonance imaging (MRI)) is restricted to major urban centers in most African countries, hampering the differential diagnosis of headache disorders. 23 On the contrary, where available, unnecessary head imaging tests for “misdiagnosed” primary headache disorders may be a deterrent to health-seeking behavior. 25
Public Awareness about headache disorders remains limited. Many people with migraine are unaware effective treatments exist. 26 Headache disorders are often seen as minor because they are episodic, nonfatal, and noncontagious. They are frequently dismissed as “normal” or trivial. These social perceptions result in stigmatization and prevent many from seeking medical help, despite experiencing significant pain and disability.7,27 People with migraine may face stigmatization when disabling headaches keep them away from work or social events. Presenteeism may be a consequence to stay employed or avoid being “labeled.” Over-the-counter medications are easy to obtain in most SSA countries. 28 There are usually no measures in place to prevent abuse, contributing to Medication Overuse Headaches (MOH). 23 Some people with migraine may prepare concoctions using herbal medications and over-the-counter analgesics. These concoctions may be applied topically, snorted, or drank. Alternatively, they may visit traditional healers, herbalists, or spiritualists.5,12 Additionally, public transport may provide opportunities for individuals to purchase medications from vendors, often lacking pharmacological expertise, who sell both conventional and “miracle cure” concoctions.29–31
Studies on headaches in SSA often focus on the prevalence and demographic associations of headache disorders, assessing their overall burden. These studies often overlook access to appropriate headache services, as well as the availability, affordability, and effectiveness of treatment options. 32 Essential headache medications, including triptans and preventive therapies, are often unavailable or unaffordable for many patients. 33 The cost of treatment can be a barrier to accessing healthcare in several SSA countries. The cost of consultations, investigations, and medications for headache disorders could prevent patients from seeking or continuing care.8,34,35 Access to neuroimaging (CT and MRI) is restricted to major urban centers in most African countries, hampering the differential diagnosis of headache disorders.23,36,37
Availability and use of evidence-based treatments
Medications listed in the Essential Medicines Lists (EMLs) across SSA for migraine treatment are varied and often arbitrary. The WHO 23rd list of Essential Medicines has only acetylsalicylic acid, ibuprofen, paracetamol/acetaminophen, and sumatriptan listed under migraine for acute therapy. 38 Metoclopramide and ondansetron are listed for indications other than migraine. Propranolol is the only medication listed under migraine for preventive therapy while bisoprolol, lamotrigine, amitriptyline, lidocaine, bupivacaine, dexamethasone, and methylprednisolone are listed under other indications. Ditans, gepants, Calcitonin Gene Related Peptide (CGRP) monoclonal antibodies and small molecules are not currently on the WHO EML. While they may be available in some countries, they are cost prohibitive.35,39 The International Headache Society (IHS) recently published global practice recommendations for acute and preventive treatment of migraine with “essential” considerations for resource-limited settings.40,41 The nuances in EMLs and medication reimbursements, where available, across SSA are summarized below (Tables 1 and 2).
Medications listed on the EMLs are usually reimbursed on the various health insurance schemes, either fully or partially, however one must be enrolled on a scheme to benefit. 55
Education/advocacy and initiative in migraine in SSA
Headaches in general, and migraine especially, are taught as part of the training required to obtain a doctorate in medicine at universities in SSA, although it is not possible to objectively quantify the volume of hours devoted to them due to the diversity of university curricula. Medical training differs between English and French-speaking countries in SSA. Since 2003, the West African Health Organization (WAHO), a specialized agency of Economic Community of West African States (ECOWAS), in collaboration with the African and Malagasy Council for Higher Education (CAMES) and the WHO, has planned and conducted programs aimed at providing solutions to the problems of health system management in this geographical area. One of the steps was the harmonization of training curricula for health professionals in the ECOWAS region. Thus, for the Diploma of Specialized Studies in Neurology, the pain module (Neu 13) with the study of headaches and facial pain is included in semester 1 of the Diploma for an hourly volume of 40 hours/600 and a credit of 2/30 compared to the other modules of this semester, namely the fundamental basics of neurology, semiology 1, and internships, which have a total hourly volume of 260, 200, and 100 hours respectively and 13, 10, and 5 credits. 56 The literature does not present training programs exclusively devoted to migraine in Africa, and even less so in SSA. Migraine education is part of headaches training in African countries in general, or in low- and middle-income countries worldwide. The IHS-GPAC (International Headache Society – Global Patient Advocacy Coalition), the African Academy of Neurology (AFAN), the World Federation of Neurology (WFN), and the IHS joined efforts to present an education program entitled “Education in Headache to Healthcare Providers in Africa (EHHPA)” since 2021. 57 The first program was held on August and September 2021 to initially introduce headache disorders with a focus on migraine. A post event certificate of attendance was awarded. The event registered 551 registrants from 71 countries of Africa beyond sub-Saharan. As a result of attending this program, a postevaluation survey found that 55% of attendees could distinguish migraine from other headache disorders, 48% had confidence to make a correct diagnosis of migraine and other types of headache disorders, 37% had their understanding of the underlying biology and pathophysiology of migraine and other headache disorders improved, 28% found their confidence in treating and managing migraine and other headache disorders increased. 58 Some specific teaching programs by headaches specialists like “headache education and management in Cameroon” have also helped to improve knowledges of health care providers in the country. 59
The DREAM (Disease Relief through Excellent and Advanced) program, initially created to treat HIV/AIDS in SSA countries, offer a model for providing headache services in the region as well. 34 Collaborations between the IHS and DREAM through the Regional Outreach Programme (IHS-ROPE) have provided headache education to primary health care providers/clinical officers in Malawi, building capacity by training trainers to ensure local sustainability for headache education. 60
Mortel et al. highlighted the fact that improving education of primary care providers in headaches in low- and middle-income countries is a critical step to improving the global burden of headaches and proposed a strategy called the “three-tiered system” advocated by “Lifting the Burden: the global Campaign against Headache,” in collaboration with the European Headache Federation.24,32 In South Africa, for example, they agree that much of the headache education effort should be focused on educating primary care providers who need to be better supported to recognize migraine and adopt appropriate approaches to treatment, including referral to specialist care if necessary. 61
Future directions
The challenges of migraine care in SSA abound, however, strategic interventions can help change the narrative. The following outlines our proposals toward achieving this goal.
Education and training
Enhancing knowledge and skills among healthcare providers represents a critical step toward improving headache care in Africa. Integration of headache medicine into medical curricula, strengthening headache education in undergraduate medical, nursing, and pharmacy programs will ensure graduates possess basic competencies in headache diagnosis and management. Developing specialized training programs, fellowships, and continuing medical education courses focused on headache medicine for practicing clinicians and establishing partnerships between African medical institutions and international headache centers will facilitate knowledge exchange and build capacity among headache care providers. Implementing headache awareness programs and partnering with government-led programs in schools can address adolescent-onset migraine and reduce stigma and absenteeism from migraine-associated disability.
Task-shifting can be achieved by training community health workers and nonspecialist providers to recognize common headache patterns and implement basic management in areas with limited specialist access. By increasing public knowledge about headache disorders through community-based education campaigns using culturally appropriate educational materials about headache disorders (their impact and treatment options) health-seeking behavior may improve. Taking into cognizance cultural beliefs and practices and adopting inclusive management approaches will improve acceptability and adherence to treatment while reducing stigma. Supporting the establishment of “headache-patient organizations” and providing resource persons to address their concerns across African countries will empower their members, create awareness and encourage advocacy for improved services.
Development of Africa-specific clinical guidelines
While international headache guidelines provide valuable frameworks, Africa-specific guidelines are needed to address unique contextual factors. Developing diagnostic approaches that account for limited access to neuroimaging and laboratory testing and creating tiered guidelines that provide management options based on available resources, from minimal to optimal care settings is essential. Given the disparities in medication availability in the essential drug lists across SSA, establishing country-specific recommendations for essential headache medications considering availability, cost, and local regulatory frameworks are important. The African Academy of Neurology, in collaboration with the International Headache Society, other headache societies and patient-advocacy groups can spearhead the development of such guidelines, ensuring they address regional variations across the continent.
Integration of traditional medicine
Integrating evidence-based traditional approaches with conventional care is essential to expanding the reach and acceptability of treatment options to patients. Conducting scientific evaluations of traditional remedies commonly used for headache relief as well as investigating African medicinal plants used for headache treatment may discover potentially effective treatments providing cheaper alternatives to orthodox medications.
Some SSA countries have healthcare facilities that offer both conventional and traditional approaches to headache management in culturally acceptable ways. These services should be evaluated to ensure well-trained and certified providers as well as evaluate efficacy of treatments. Collaborative relationships between traditional healers and conventional healthcare providers will improve prompt referrals of complex cases.
Telemedicine and digital health solutions
Digital health technologies—including tele-neurology consultations, headache tracking applications, and text-message-based educational interventions—have the potential to transform headache care, especially in underserved regions where access to specialist care is limited.
Tele-neurology consultations allow patients in remote or rural areas to connect with neurologists and headache specialists via video or phone calls reducing the need for long-distance travel. Through telemedicine, primary care providers can also consult with specialists for guidance on complex cases, improving diagnostic accuracy, and treatment decisions.
Headache tracking apps empower patients to monitor their symptoms, medication use, and potential triggers daily. These digital tools can generate detailed headache diaries, which help both patients and healthcare providers identify patterns, assess treatment effectiveness, and make informed adjustments to care plans. By facilitating self-management, these apps encourage patients to take an active role in their health, which can lead to better adherence to treatment and improved outcomes.
Text-message education programs deliver tailored health information, reminders, and motivational messages directly to patients’ mobile phones. In regions where smartphone penetration is low, basic short messaging service (SMS) can still be a powerful tool for raising awareness about migraine, educating patients on lifestyle modifications, and reminding them to take medications or attend follow-up appointments.
By integrating these digital solutions, healthcare systems can bridge critical gaps in headache care. These technologies can reduce disparities in headache diagnosis and management, leading to better health outcomes for populations that have historically been underserved.
Innovative service delivery models
Developing mobile/traveling clinics that visit underserved areas on a regular schedule to provide specialist assessments and follow-up care can improve the reach of migraine-specialist services. Shared medical appointments can be arranged for headache patients to maximize specialist time while providing peer support.
Collaborations between headache specialists and private sector healthcare providers can expand access to diagnostic facilities and specialized care. Establishing occupational health initiatives that address headache disorders may improve early diagnosis and reduce productivity losses.
Research and surveillance
While the majority of the literature on headaches in SSA have focused on migraine prevalence in special groups and populations, they are not comprehensive. Several countries lack published data. Conducting comprehensive standardized surveys across SSA to determine the prevalence and burden of migraine and other headache disorders is important. Investigating unique genetic and environmental factors affecting headache presentation and treatment response in African populations as well as quantifying the economic impact of headache disorders and cost-effectiveness of interventions will provide more reliable and comparable data to inform policy changes. Strategies to evaluate the implementation of evidence-based headache care in resource-limited settings are required.
African headache registries
The establishment of multicenter patient registries to track disease characteristics, treatment patterns, and outcomes can serve as a means of evaluating collaborative efforts. This can help focus collaborative efforts where care and outcomes are not optimal.
Medication access and affordability
Improving access to effective headache medications requires systemic approaches.
Supporting the production of generic headache medications within Africa can reduce costs and improve supply reliability. Establishing regional medication-purchasing collaboratives as a pooled procurement effort will leverage economies of scale and reduce prices. With newer headache medications like the anti-CGRP monoclonal antibodies which are currently recommended as first line preventive medication rather than a last resort negotiating with pharmaceutical companies for differential/tiered pricing favoring African markets will be advantageous. 62 Streamlining regulatory processes across African regions are necessary to facilitate medication registration and availability.
Advocating for the inclusion of headache medications within national essential drug lists and in national health insurance schemes are necessary to ensure medication access and affordability.
Implementation considerations
Implementing the proposals above will require coordinated efforts across multiple stakeholders. The following elaborate strategies to achieve this:
Policy level:
Development of national headache strategies within noncommunicable disease frameworks. Inclusion of headache disorders in national health insurance coverage. Investment in neurological training programs and retention of specialists. Regulatory frameworks that support telemedicine and task-shifting approaches.
Institutional level:
Establishment of headache centers of excellence in major teaching hospitals. Integration of headache assessment into primary healthcare protocols. Development of referral pathways between primary, secondary, and tertiary care. Implementation of quality measurement metrics for headache care.
Individual provider level:
Commitment to continuing education in headache medicine. Adoption of evidence-based practice guidelines. Engagement with patient education and advocacy efforts. Participation in research and quality improvement initiatives.
Conclusion
In conclusion, migraine is associated with high levels of disability across SSA. Despite few neurologists and headache specialists, the existing cadre of primary and secondary healthcare providers can be equipped to provide appropriate diagnoses, treatment, and referral of complex cases when needed. Educational campaigns like the IHS-ROPE and the EHHPA have successfully improved headache knowledge among primary care providers and should be encouraged.
The majority of SSA countries, despite having some measures in place for the very poor, do not have NHI/CBHI policies. National EMLs do not contain a wide variety of options for migraine care. Where they are listed, they may fall under other diagnoses instead of. These EMLs are not necessarily in sync with the medications reimbursed by the NHI/CBHI schemes. We have proposed various measures to improve migraine (and headache in the broader context) care across Africa. Africa must unite to improve migraine care and reduce disability.
Public health relevance
Migraine is managed mainly at the primary care level by nurses, clinical officers/physician assistants, and general physicians.
Improving diagnosis and management of migraine requires regular programs educating and empowering the primary care level while encouraging referral of complicated cases to specialists.
The IHS-ROPE, EHHPA, and Migraine Outreach programs have been successful platforms for education and should be sustained.
Footnotes
Ethical considerations
Institutional Review Board approval was deferred for this narrative review paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used for this article may be obtained from the authors with a reasonable request.