
Abstract
This study was an 8-month controlled trial to evaluate the effectiveness of a workplace educational and physical programme in reducing headache and neck and shoulder pain. Central registry office employees (
Introduction
Headache and neck and shoulder pain are both a clinical challenge and a major health problem (1–4). An assessment of the evidence of the worldwide prevalence and burden of headache disorders by Stovner et al. (5) disclosed the following percentages for adults with an active headache disorder: 46% for headache in general, 11% for migraine, 42% for tension-type headache and 3% for chronic daily headache. Application of the World Health Organization's ranking of causes of disability would bring headache disorders into the 10 most disabling conditions for both sexes and into the five most disabling for women (5). Assessment of the combined survey data on visits to doctor's surgeries, hospital out-patient departments and emergency departments, and hospital admission for neck pain in the USA has shown that 10.2 million visits/year occurred in the period 2001–2002 (4).
Non-invasive physical management is often prescribed for neck pain and headache. Systematic reviews, however, have indicated that its effectiveness is limited (6–10). In addition, concentration on either headache or neck pain overlooks the fact that they are frequently associated (11–14).
We have for some time been applying a simple educational and physical programme designed to decrease muscle tension in the head, neck and shoulder area. The simplicity of our programme is such that patients can follow it on their own after a short initial instruction. Its cost is negligible. In our clinical experience, it has reduced the frequency and intensity of headache and neck and shoulder area pain in a considerable number of patients. The purpose of this controlled trial was to evaluate its effectiveness in reducing frequency and intensity of headache and pain in the neck and shoulder area in a large cohort of public servants after 6 and 12 months' follow-up. This study describes our results in terms of its primary objective, i.e. evaluation of the effectiveness of the programme in reducing the frequency of head and neck pain after 6 months. The results of the longer follow-up will be presented in a subsequent paper.
Methods
Study design and participants
This was a controlled, non-randomized trial designed to evaluate the effectiveness of a workplace educational and physical programme in reducing the frequency of head and neck pain.
The eligible participants were 661 employees of the City of Turin's registry and tax offices on 1 January 2005: 330 at the central registry office, 128 at peripheral registry offices and 203 at the tax office. Their work involved contacts with the public and the use of video terminals.
An individual-based, randomized design was not feasible because the subjects were working in the same environment with a high risk of interference and contamination between the study group and controls. A cluster randomized design was barred by the unbalanced distribution of the workers between offices. Two groups were formed: one composed of employees at the central registry office, the other of employees at the peripheral registry offices and the tax office. For feasibility reasons (i.e. the advantage of having all intervention subjects at a single site), the first group was chosen as the study group, the second as the controls. No exclusion criteria were applied.
Assuming 50% participation, a sample size of about 330 subjects provided a power of 0.80 to detect a meaningful difference between groups of at least 10% (α= 0.05, two-tails) in the proportion of symptomatic subjects with a significant reduction of pain frequency.
The study was conducted in accordance with the Declaration of Helsinki and the Guidelines for Good Clinical Practice. The protocol was assessed and approved by the Institutional Review Board of the San Giovanni Battista Hospital of the City of Torino. All eligible subjects were asked to provide their informed consent.
Procedures
All participants were given a diary for the day-by-day recording of severity and duration (hours) in that day of their headache and neck and shoulder pain, intake of analgesics (by type) and menstruation days. Headache severity was coded as follows: score 0, no pain; 1, very mild pain, not perceived if distracted; 2, mild pain, constantly perceived; 3, moderate to severe pain that permits daily activity; 4, severe pain that impedes any activity; 5, excruciating pain.
Diaries were directly filled in by subjects, and were automatically processed by an optic reader via a dedicated computer program.
Some general characteristics and detailed data relative to headache and neck and shoulder pain were collected in a standardized fashion by trained physicians. A psychological assessment according to Axis 1 (Anxiety-, Mood- and Somatoform-Disorders) of the Diagnostic and Statistical Manual of Mental Disorders-IV was then carried out to look for major depression and/or anxiety disorders in a structured interview (15). A clinical examination that included palpation of pericranial and cervical muscles was performed.
The following diagnoses were made according to the guidelines of the International Classification of Headache Disorders (16) and the International Association for the Study of Pain (17): migraine with or without aura (M), tension-type headache (TTH), myogenous neck and shoulder pain (MP). Two or more diagnoses in the same subject were possible.
Following the establishment of a 2-month baseline picture in March and April 2005, the study group was shown how to apply the physical and educational programme. Both groups continued to fill in their diaries until month 8 (Fig. 1).

Flow chart.
Before administering the program an explanation was given of its main purposes, and particular emphasis was placed on the fact that some muscles, especially in the cranio-facial-cervical area, may be unconsciously kept at a too high stage of contracture and that this may facilitate or increase pain in that area. Thus, the aim of the programme was to reduce muscle contraction and to increase the capability of perceiving it when too elevated. The programme consists of brief shoulder and neck exercises to be performed several times a day, a relaxation exercise, and instructions on how to reduce parafunction and hyperfunction of the craniofacial and neck muscles during the day. These instructions are given below.
Relaxation exercise (once or twice a day)
Sit down in a comfortable armchair in a quiet room. Let your lower jaw drop completely for about 10–15 min. Apply warm pads on your cheeks and shoulders.
Posture exercises (8–10 times every 2–3 h): (i) stand upright with your heels, hips and nape of the neck against a wall. Without moving the rest of your body, bring your shoulders into contact with the wall and release, rhythmically; (ii) with your body and head against the wall, make horizontal movements of the head, forwards and backwards; (iii) cup your hands behind your neck. Stretch your head backwards against counterpressure from your hands. Relax after 2–3 s.
Visual feedback
Place red labels in strategic sites to remind you to avoid excessive contraction of your head and neck muscles.
The instructions were given by a clinician in conjunction with other members of the health staff. The programme was explained to groups of 30–40 subjects with the help of a short film followed by a practical demonstration and training. The time employed ranged from 45 to 60 min. Red labels were placed on the workplace. Other labels were provided for use at home. A written form was also provided with illustrations on the exercises (Fig. 2) and the relative instructions. At months 4 and 6 of the study period, the instructions were reiterated by the same clinician at the workplace.

Exercises for neck and shoulder.
Study outcomes
The primary outcome measurement was the change in frequency of headache or neck and shoulder pain (number of days per month with a headache/neck and shoulder pain). Two end-points were used: (i) the between-group difference of pain reduction at months 7–8 compared with baseline; and (ii) the between-group difference in the proportion of subjects with four or more days per month with headache (neck and shoulder pain) during the baseline period who achieved a ≥ 50% reduction in pain frequency by month 7–8 (responder rate).
Secondary outcome measurements were the between-group differences in: (i) headache or neck and shoulder pain index (intensity × frequency), where intensity is the sum of intensity of the daily pain in a month divided by number of days with pain, and frequency is number of days with pain in a month; and (ii) frequency of days with analgesic drug consumption.
Statistical analysis
Baseline differences between the study group and the controls were evaluated with the Mann–Whitney
The data were analysed separately for headache and for neck and shoulder pain. Between-group comparisons are based on changes in the end-points at the end of the study (month 7–8 of follow-up) compared with baseline (months 1–2). Analyses were performed on both the intention-to-treat population and subjects with complete diaries for the entire study period.
The difference in the frequency of symptoms between months 7–8 and the baseline (months 1–2) was calculated for each subject. These differences were compared between the two groups with unpaired Student's
Exploratory subgroup analyses were performed according to protocol by gender, age, diagnosis, psychiatric comorbidities; for each subgroup, adjustment was made for all the variables mentioned above. Interaction was tested by inserting an interaction term between the treatment group and the subgroup covariate of interest. Compliance during the entire period was classed as low (if exercises were performed no more than three/four times a week) and medium to high (if they were performed almost every day or exactly as indicated). The proportion of symptomatic subjects (mean of ≥ 4 days/month of pain during the baseline period) with a ≥ 50% reduction in headache days and in neck and shoulder pain days at months 7–8 was compared between the two groups by using logistic regression models, including the above-mentioned covariates. The proportion of subjects with a ≥ 50% increase in the headache day frequency was also compared between groups.
Reduction of the frequency of pain and drug consumption was also evaluated by applying longitudinal models to the intention-to-treat population. The probability of a daily headache episode during the follow-up was analysed with a logistic regression model, adjusted for clustering due to repeated measures on the same subject with the Huber–White sandwich estimators (18). Relevant covariates were selected by means of a backward procedure and the Akaike Information Criterion; variables included were age, sex, presence of anxiety or mood disorders, baseline symptoms value of each subject, presence of neck and shoulder pain (when the reduction in the frequency of headache and in the use of drug consumption was analysed) and presence of headache (when the reduction in the frequency of neck and shoulder pain and in the use of drug consumption was analysed). Effect of time during the follow-up was modelled using a restricted cubic spline function, with an interaction with the study group to enable the model to allow for non-linear treatment effects over time. The same method was used for the other end-points
Analyses were performed using STATA 8.2 (STATA Corp., College Station, TX, USA), S-Plus 6.2 (Insightful Corp., Seattle, WA, USA) and with Design and Hmisc program libraries (19).
Results
Subjects who did not give informed consent (
Table 1 summarizes the characteristics at baseline for the intention-to-treat population and the subjects with complete diaries (
Characteristics of the study population at baseline (months 1–2)
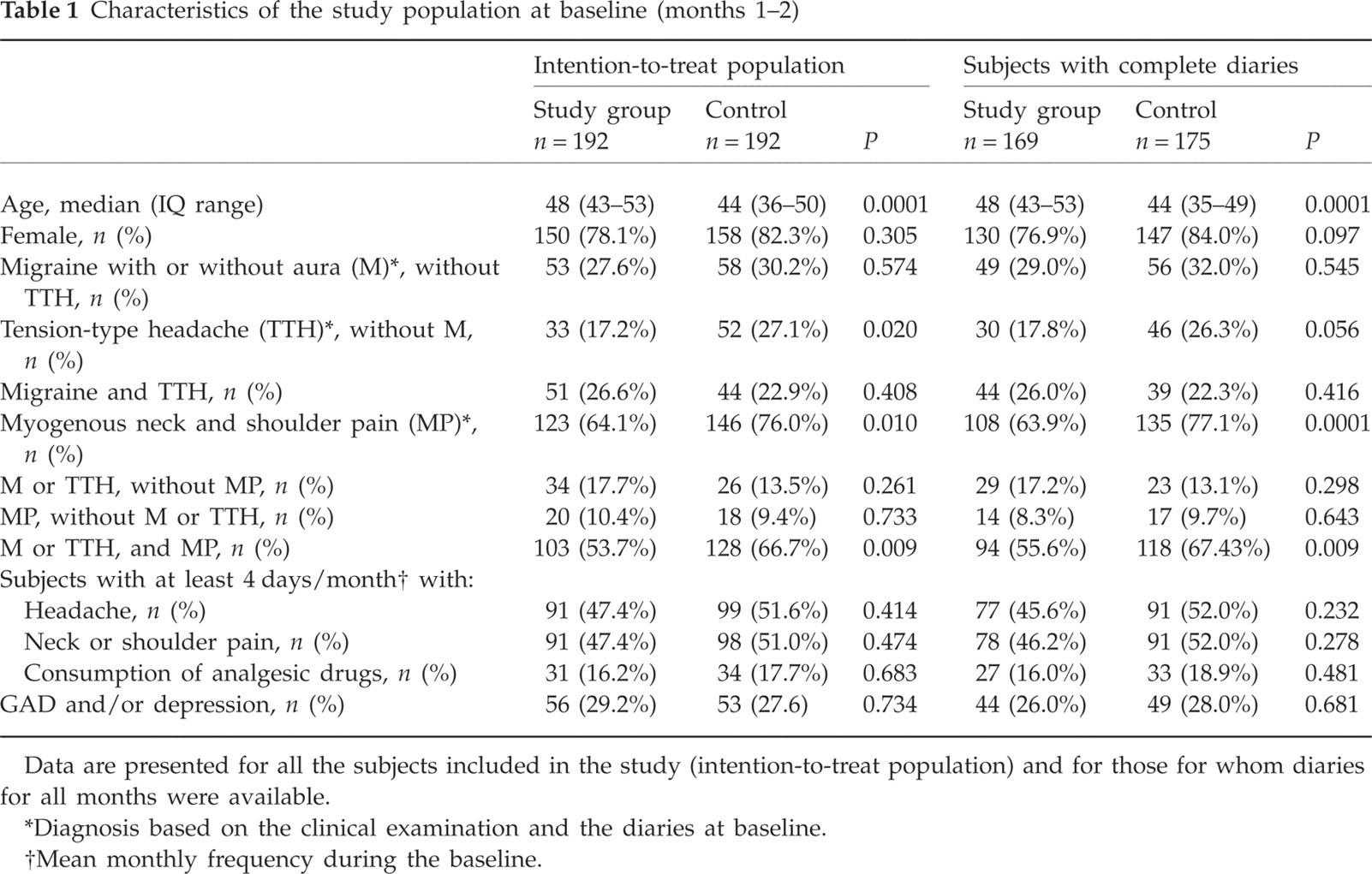
Data are presented for all the subjects included in the study (intention-to-treat population) and for those for whom diaries for all months were available.
Diagnosis based on the clinical examination and the diaries at baseline.
Mean monthly frequency during the baseline.
Due to the non-randomized design of the study, the two groups were not completely balanced at baseline with regard to some characteristics and the distribution of different types of headache and of neck and shoulder pain. Prevalence of M (alone or associated with TTH) in the study group and in the controls was 54.2% and 53.1%, respectively; prevalence of TTH not associated with migraine was 17.2% and 27.1%; prevalence of neck and shoulder pain was 64.1% and 76.0%, respectively. About 80% of subjects enrolled were female. The controls were significantly younger than the subjects in the study group: median (interquartile range) for age was 48 years (43–53) in the study group and 44 years (36–50) in the controls. A diagnosis of anxiety or depressive disorder was made in > 25% of the population. Anxiety disorders were generalized (GAD) in 94% and panic disorders or agoraphobia in 6%. Depressive disorders were dysthymic in 64% and major depressive in 36%. The ratio between these disorders was very similar in subjects with complete diaries and in the intention-to-treat population.
The frequency of the end-points considered at baseline and at months 7–8 in subjects with complete diaries, as well as the mean differences for each group and their absolute between-group differences, both crude and adjusted, are summarized in Table 2. Days per month with headache at baseline were 5.87 for the study group and 6.30 for controls. Days with neck and shoulder pain were 7.12 and 7.79, respectively. Days of analgesic consumption were 2.03 and 2.04.
Effects of the intervention for the different end-point examined
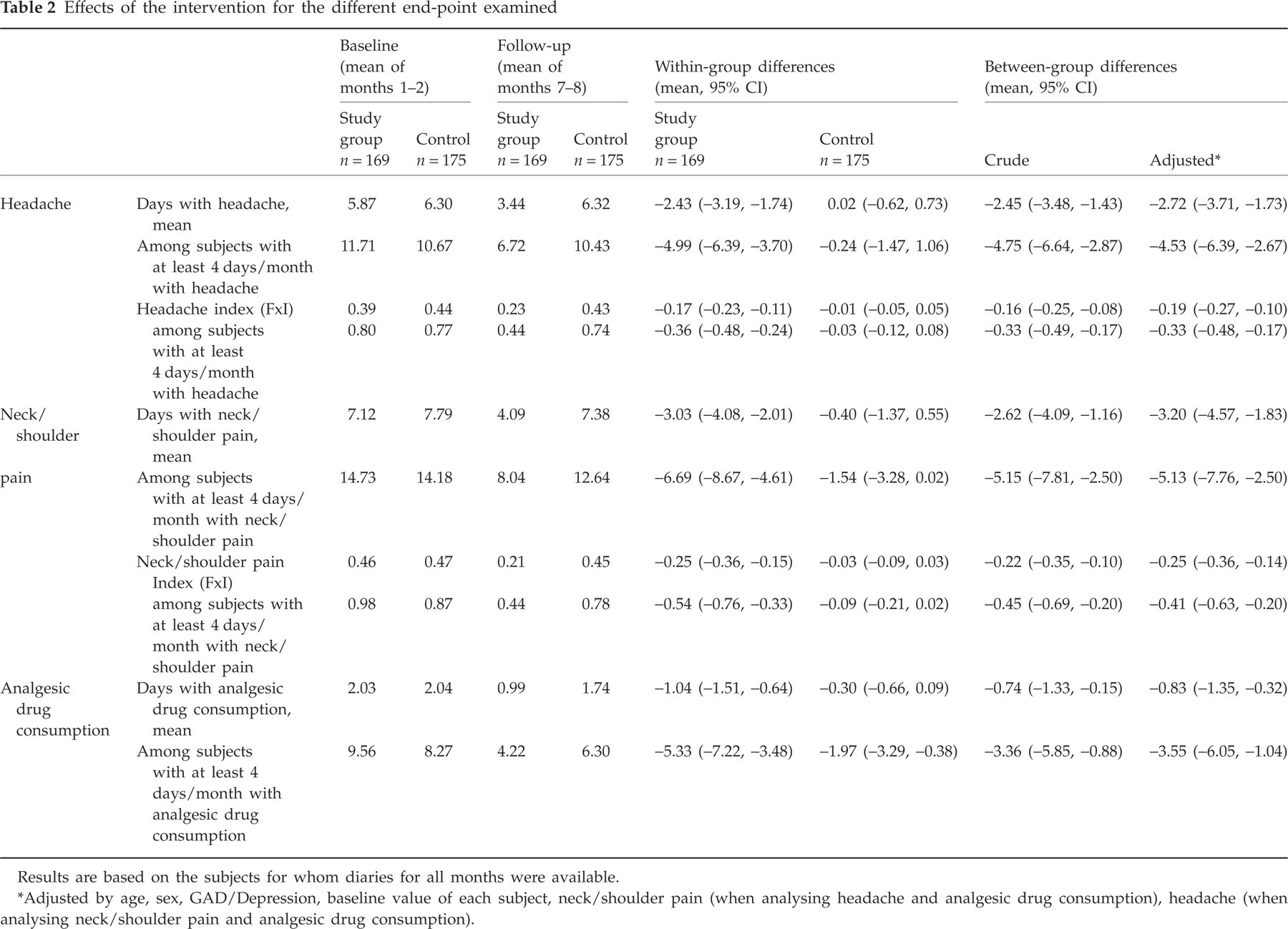
Results are based on the subjects for whom diaries for all months were available.
Adjusted by age, sex, GAD/Depression, baseline value of each subject, neck/shoulder pain (when analysing headache and analgesic drug consumption), headache (when analysing neck/shoulder pain and analgesic drug consumption).
For the primary and secondary end-points, the study group subjects achieved a significant improvement by the end of the follow-up compared with control subjects. The risk reduction for the primary end-points was around 40%. Mean treatment effects [days per month, 95% confidence interval (CI)] on comparing the last 2 months vs. baseline were: headache frequency −2.45 (−3.48, −1.43); frequency of neck pain −2.62 (−4.09, −1.16); days with analgesic consumption −0.74 (−1.33, −0.15). As expected, the effect was more evident in the subgroups of subjects with a higher prevalence of symptoms at baseline. There were no substantial differences between crude and adjusted estimates of treatment effects.
Figure 3 reports the results of the exploratory analysis to examine the effect of treatment by subgroups. The presence of GAD or depression seemed to modify the effect of the programme, for all the end-points examined (for headache,
Proportion of subjects with ≥ 4 days/month with pain (or drug consumption) during the baseline period that had a reduction (improved) or an increase (worsened) in pain frequency or drug consumption of ≥ 50% at the end of follow-up

Adjusted by age, sex, GAD/Depression, neck/shoulder pain (when analysing headache and analgesic drug consumption), headache (when analysing neck/shoulder pain and analgesic drug consumption), baseline value of each subject.

Effects of the programme referred to the end-points by subgroups. Changes from baseline were adjusted for age, sex, presence of anxiety or mood disorders, baseline symptoms value of each subject, presence of neck and shoulder pain (when the reduction in the frequency of headache and in the use of drug consumption were analysed) and presence of headache (when the reduction in the frequency of neck and shoulder pain and in the use of drug consumption were analysed).
In the study group, the probability of achieving a ≥ 50% decrease of pain days was greater among symptomatic subjects with a medium–high level of compliance compared with those with a low level of compliance. However, the results were not statistically significant (for headache: adjusted OR = 1.68, 95% CI 0.63, 4.45; for neck/shoulder pain: adjusted OR = 1.65, 95% CI 0.54, 5.05), and some efficacy was observed also in subjects whose compliance was not optimal.
Figure 4 shows the results observed with the logistic regression model based on the intention-to-treat population (192 in each group). In the baseline period, some improvement of all three end-points considered was observed in both groups. However, the trend became quite different when the programme began. The positive trend continued in the study group, whereas in the control group regression to the original values was observed, somewhat delayed in the case of drug consumption. The difference between the groups became significant after approximately 2 months from the start of the programme for headache and neck and shoulder pain and after 4 months for drug consumption.

Reduction in pain frequency and drug consumption in the intention-to-treat population. Results expressed as adjusted odds ratio (OR) (95% confidence interval). The vertical dashed line indicates the point where the study group began to follow the programme after the 2-month baseline period. The ORs were adjusted for age, sex, presence of anxiety or mood disorders, baseline symptoms value of each subject, presence of neck and shoulder pain (when the reduction in the frequency of headache and in the use of drug consumption were analysed) and presence of headache (when the reduction in the frequency of neck and shoulder pain and in the use of drug consumption were analysed).
Discussion
We observed a significant reduction of about 40% of the monthly frequency of headache and neck and shoulder pain in the study group subjects compared with controls. Moreover, the headache or neck and shoulder pain index and the monthly frequency of drug intake significantly decreased in the study group.
The present study supports the findings of previous studies that workplace-based physical exercise interventions can decrease headache and neck symptoms.
Several studies have assessed the efficacy of non-invasive physical management in reducing the frequency of different types of headache and neck pain. However, the weight of evidence is still limited and the results of recent studies are conflicting (20–24). A Cochrane systematic review of trials (7) comparing non-invasive physical treatments for headache with any type of control found only 10 trials with methodological quality scores of ≥ 50 (using a 100-point scale). The authors could not pool the results because of high study heterogeneity in terms of headache type, patient characteristics, forms of management, comparison therapies, and outcome measurements.
Sjögren et al. (22) have performed a cluster randomized controlled crossover trial on 53 office workers to examine the effects of a workplace physical exercise intervention on the perceived intensity of headache and the intensity of symptoms in the neck and shoulders. The intervention resulted in a slight, but statistically significant, decrease in the intensity of headache and neck symptoms. Nikander et al. (25) in a randomized controlled study examined the dose–response relationship of specific strength-training and endurance-training regimes for the cervical muscles, in 180 female office workers with chronic neck pain. The authors found that both exercise protocols were associated with significant decreases in chronic neck pain and disability.
Our study has some characteristics that differentiate it from previous trials. First, and perhaps most important, its sample size was considerably larger and the follow-up period longer than in other studies. In addition, all the subjects who agreed to participate belonged to an identical working community. The occurrence of pain and its severity was assessed from diaries kept during a 2-month baseline period. Furthermore, this is one of the few studies in which management consisted of a simple, self-administered physical exercise programme performed without leaving the workplace and at home, and without the intervention of paramedical staff. A further strength of the present study is the careful assessment of the symptoms recorded in the diaries throughout the trial, and the relatively small number of drop-outs. Lastly, head, neck and shoulder pain locations were investigated jointly.
The main weakness of the trial design is the lack of a formal randomization. The subjects were assigned to the study group and the control group according to their place of work. Since our programme included exercises and visual feedback measures in the workplace, individual randomization was difficult due to the high level of interference and contamination between subjects working in the same environment. Cluster randomization was equally difficult, since half of the participants worked in a single, central department. The characteristics of our programme were such that a reciprocal reinforcement of its educational aspects may be induced by more enthusiastic and collaborative participating subjects. When the instructions were reiterated at months 4 and 6 of the study period, these subjects were congratulated and encouraged to carry on with their commitment. Indeed, this aspect probably explains the few drop-outs and the better results obtained compared with some other trials (21, 22).
A somewhat unbalanced distribution at baseline of some characteristics between the two groups was expected due to the lack of formal randomization. However, it should be noted that the frequency of headache, neck and shoulder pain and analgesic drug consumption did not differ significantly between the two groups at baseline among ‘symptomatic’ subjects, for whom the highest benefit of the programme was expected.
An appropriate analytical approach was adopted to deal with problems related to the non-randomized design and possible confounding factors. We did not simply compare the mean values of the outcome observed in each group at the end of follow-up; the within-subject difference (Δ) in outcome frequency between baseline and the end of follow-up was calculated, and then the mean Δ for each group was calculated and compared; in this way we excluded that the observed difference between groups could be due to differences in the frequency of the symptoms at baseline; these between-group differences were also adjusted for several potential confounding factors, including the baseline value of each subject.
In addition, an analysis on the intention-to-treat population was also performed using longitudinal models and adjusting for the mentioned confounders, obtaining consistent results.
Another weakness is that neither the subjects nor researchers were ‘blinded’. In physical exercise studies, it is almost impossible to ‘blind’ subjects by including a placebo treatment, because a good and trustworthy placebo cannot be easily developed. These studies may thus contain some non-specific attraction or placebo effects.
Head and neck pain may display seasonal variations in function of temperature and humidity fluctuations (26–28). This may explain the early, albeit not significant, improvement of head and neck pain frequency in both groups during the baseline period (March–April). A second reason may be related to the subjects' expectancy, reinforced by keeping a diary. In our data a seasonal effect was particularly evident in August (Fig. 4), when in Italy the climate is warm and most workers take their holidays. However, the improvement persisted after this period in the study group only, as opposed to what was observed in the control group.
In the study group, 49 of the subjects who agreed to participate had no headache and 60 no neck pain in the baseline period compared with 21 and 40 of controls. The fact that more subjects worsened in the control group suggests that the programme may have a preventive effect. The numbers, however, are too small to allow any definite conclusions to be drawn, and longitudinal studies on more extensive population samples are needed.
In our study the prevalence of subjects suffering from M was slightly higher than of those with TTH. This may reflect selective participation in the trial, since subjects with migraine, albeit episodic, might have been more interested in participating than those with occasional TTH.
Some explanations of the positive effects of the programme may be suggested. First, its substantial educational component (approach to the problem and discussion of its major aspects, periodical instruction reinforcement, reinforcement by the more motivated subjects of the working community, visual feedback, etc.) may be responsible for beneficial effects through mechanisms involving expectation and conscious anticipation (29, 30). Moreover, the expectation of clinical benefit, which is equivalent to the expectation of reward, may be supposed to trigger placebo responses by activating reward mechanisms (31).
A particularly interesting finding of this study is that subjects with anxiety or depression were even better responders. This result is in line with the observation in other studies that the placebo response was stronger in patients with GAD and major depression (32). Moreover, high and moderate levels of psychopathology have been associated with heightened placebo analgesia in chronic low back pain patients (33).
Most of our subjects suffered from concomitant headache, neck and shoulder pain, as in other studies (11, 13, 34). The results suggest that the beneficial effect of the programme on their headache frequency is higher than in those suffering from headache only (Fig. 3). It is generally agreed that neck and shoulder pain is frequently associated with TTH (35, 36) and, to some extent, with M (37). Migraine patients also display a high occurrence of pain and tender points in the upper cervical region (38, 39), and evidence of musculoskeletal dysfunction of the neck (38). In patients suffering from headache and facial pain, muscle tension has been reported to increase further in the concomitant presence of anxiety or depression (40, 41). Reduction of muscle tension may thus be one of the factors through which the programme was consistently able to decrease the prevalence of TTH and M, and of neck and shoulder pain. As expected, medium–high compliance was accompanied by a greater effect. However, the difference was not statistically significant, and considerable efficacy was observed also in subjects whose compliance was not optimal. This is not surprising if one considers that the educational aspects of the programme were the same for all participants (discussion and explanation of the issues, practical demonstrations and training, visual feedback). Indeed, most subjects with a low level of compliance may have acquired the ability to maintain their craniocervical muscles at a lower contraction level during the day.
Prior to this trial, we had built up a long, clinically-based record of the efficacy of our programme in many patients with head and neck pain disorders. The positive results now obtained with this relatively simple form of management suggest its effectiveness and its high acceptability in a large, unselected, working population.
In conclusion, if our results are confirmed by future studies with a randomized design, this programme could be regarded as an effective way of reducing head and neck pain and analgesic drug consumption in extensive working communities, with presumably a very satisfactory cost–benefit ratio.
Footnotes
Acknowledgements
This study was primarily funded by the Compagnia di San Paolo of Torino with additional contributions from the Regione Piemonte. We thank A. Deregibus (University of Turin) for his help in planning the conduct of the study and in the preliminary stage of data collection; D. Gregori (University of Turin) for his excellent comments on the statistical analysis; and J. Iliffe for his invaluable assistance in editing the manuscript.