
Abstract
Background
In the absence of head-to-head analyses, indirect treatment comparisons (ITCs) can be used for comparative treatment evaluations. A previous ITC of atogepant and rimegepant assessed outcomes from US trials for the preventive treatment of migraine. We expand those initial analyses, and use an ITC to evaluate the efficacy, safety, and tolerability, and estimate the number needed to treat (NNT) per additional ≥50% responder for atogepant and rimegepant in Japanese participants.
Methods
RELEASE (M22-056) and BHV3000-309 were randomized, double-blind, placebo-controlled studies evaluating atogepant compared with placebo and rimegepant compared with placebo for the preventive treatment of episodic migraine (EM) in Japanese participants, respectively. An ITC using a random effects model compared the efficacy, safety, and tolerability of atogepant 60 mg once daily and rimegepant 75 mg once every other day. Estimates of mean differences with 95% confidence intervals (CIs) are presented for monthly migraine days (MMDs), acute medication use days, Migraine-Specific Quality of Life Questionnaire v2.1 (MSQ v2.1) Role Function-Restrictive (RFR) domain score, Migraine Disability Assessment (MIDAS), and European Quality of Life Visual Analog Scale (EQ VAS). Safety and tolerability results are presented as hazard ratios and 95% CIs. The NNT resulting in one additional person achieving a ≥ 50% reduction from baseline in mean MMDs/monthly headache days was analyzed across three responder definitions.
Results
Atogepant demonstrated significantly higher mean monthly acute medication use days reduction (−1.68, 95% CI: −2.72 to −0.64; P < 0.002) at weeks 1 to 12 and significantly greater improvement in MSQ v2.1 RFR domain score (5.13, 95% CI: 1.10 to 9.16; P = 0.01) at week 12. Additionally, atogepant demonstrated numerically higher mean MMD reduction at weeks 1 to 12, numerically greater reduction (improvement) in MIDAS at week 12, and numerically lower improvement in EQ VAS at week 12 relative to rimegepant (all P > 0.05). Atogepant demonstrated numerically lower likelihood of treatment-emergent adverse events (TEAEs) (0.70, 95% CI: 0.45 to 1.09) and adverse events (AEs) leading to discontinuation (0.50, 95% CI: 0.03 to 9.46) compared with rimegepant (both P > 0.05). The median NNT (95% CI) versus placebo for a ≥ 50% reduction from baseline in mean MMDs across weeks 1 to 12 was 2.5 (1.9 to 4.1) for atogepant and 16.6 (6.7 to ∞) for rimegepant. Additional responder definitions were consistent.
Conclusions
Among Japanese participants with EM, atogepant 60 mg demonstrated significantly or numerically greater improvements in four of five efficacy outcomes and numerically lower TEAEs and AEs leading to discontinuation compared with rimegepant 75 mg. Atogepant 60 mg had substantially lower NNTs per additional ≥50% responder versus placebo than rimegepant 75 mg.
Introduction
Current estimates show migraine impacts ∼1.1 billion individuals worldwide and the prevalence of migraine in Japan is estimated at 6.0% to 8.4%.1,2 Episodic migraine (EM) comprises the majority of individuals with migraine (≥90%) and is characterized by <15 headache days per month. 3 Clinical treatment guidelines from the Japanese Society of Neurology state that preventive treatments for migraine should be considered for individuals who experience >2 migraine attacks per month, have significantly impaired quality of life or daily functioning, have an insufficient response or contraindication to acute treatments, or have a risk of medication overuse headache due to frequent use of acute treatments. 4
Preventive treatments for migraine include oral, nonspecific treatments, such as antiseizure medications and beta blockers, and a newer class of treatments targeting calcitonin gene-related peptide (CGRP) or its receptor, a key neuropeptide implicated in migraine pathophysiology.5–7 The CGRP targeted treatments include injectable monoclonal antibodies (mAbs) and oral CGRP receptor antagonists, or gepants.8,9 Atogepant and rimegepant are oral CGRP receptor antagonists approved in the United States and European Union (EU) for the preventive treatment of migraine (rimegepant for EM and atogepant for EM and for chronic migraine [CM]).10,11 The efficacy and safety of atogepant and rimegepant for the preventive treatment of EM have been established in pivotal US trials: atogepant, ADVANCE (NCT03777059) 12 ; rimegepant, BHV3000-305 (NCT03732638). 13 Recently, atogepant and rimegepant have been evaluated for the preventive treatment of EM in Japanese participants: atogepant, RELEASE (M22-056, NCT05861427) 14 ; rimegepant, BHV3000-309 (NCT05399485). 15
Comparative analyses between migraine preventive treatments may assist clinicians in making informed treatment decisions and optimizing the management of migraine.16–19 However, there is a lack of head-to-head trials in migraine including a direct comparison of atogepant and rimegepant for the preventive treatment of EM. A previous indirect treatment comparison (ITC) has been used for comparative evaluations of atogepant and rimegepant for the preventive treatment of migraine in US trial populations. 20 Additionally, a matching-adjusted indirect comparison (MAIC), which allowed for comparisons between atogepant and rimegepant, evaluated comparative efficacy, safety, and tolerability. 21 Expanding on those initial analyses, we utilized an ITC analysis based on registrational trial data from RELEASE and BHV3000-309 to compare the efficacy, safety, and tolerability of atogepant and rimegepant in Japanese participants. The number needed to treat (NNT) is a useful tool for evaluating the potential benefits of treatments and has been used in several recent studies comparing preventive migraine treatments.20,22 NNT also provides important clinical utility by expressing information in patient numbers and supporting clinical decision making about the number of patients needed to treat with a particular treatment to achieve a positive outcome. 23 Therefore, the NNT based on a ≥ 50% reduction from baseline (≥50% responder rate) in mean monthly migraine/headache days (MMDs/MHDs) was also evaluated to compare the efficacy of atogepant and rimegepant.
Methods
Study design
RELEASE was a phase 2/3, multicenter, randomized, double-blind, placebo-controlled study evaluating atogepant 10 mg once daily (QD), 30 mg QD, and 60 mg QD compared with placebo for the preventive treatment of EM in Japanese participants. 14 The atogepant 60 mg dose is reported here and the atogepant 10 and 30 mg doses are reported in the supplemental materials. BHV3000-309 was a phase 3, multicenter, randomized, double-blind, placebo-controlled study evaluating rimegepant 75 mg every other day compared with placebo for the preventive treatment of migraine in Japanese participants. 15
Key study design details for RELEASE and BHV3000-309 are summarized in Supplemental Table 1. RELEASE included a 4-week screening/baseline period, 12-week double-blind treatment period, 12-week active treatment extension period, and 4-week safety follow-up period. BHV3000-309 included a 28-day observation period, 12-week double-blind treatment phase, and a 40-week open-label treatment phase. RELEASE included participants with 4 to 14 MMDs and <15 MHDs in the 3 months before visit 1 and 4 to 14 MMDs and <15 MHDs during the 28-day baseline period. BHV3000-309 included participants with 4 to 18 migraine attacks of moderate or severe intensity per month within the past 3 months prior to the screening visit, and ≥4 MMDs and ≤18 MHDs during the 28-day observation period. Participants in RELEASE were not allowed to take any preventive migraine treatments 30 days before visit 1 and throughout the trial. Participants in BHV3000-309 were allowed to take one preventive migraine treatment, excluding CGRP mAbs or gepants, provided that the dose was stable for ≥3 months before the observation phase and did not change throughout the study.
Outcomes
An ITC based on registrational trial data from RELEASE and BHV3000-309 in Japanese participants was used to compare the efficacy, safety, and tolerability of atogepant 60 mg and rimegepant 75 mg. The outcomes assessed were based on similar primary, secondary, and exploratory outcomes between RELEASE and BHV3000-309. The efficacy outcomes included change from baseline in mean MMDs, change from baseline in mean monthly acute medication use days, change from baseline in Migraine-Specific Quality of Life Questionnaire v2.1 (MSQ v2.1) Role Function-Restrictive (RFR) domain score, change from baseline in Migraine Disability Assessment (MIDAS) total score, and change from baseline in European Quality of Life Visual Analog Scale (EQ VAS) score. MSQ v2.1 is a 14-item questionnaire measuring health-related quality of life impairments associated with migraine in the past 4 weeks. The RFR domain score evaluates the impact of migraine on an individual's daily social and work-related activities. Full methods for MSQ v2.1 have been previously reported. 24 MIDAS is a 7-item questionnaire measuring headache-related disability over a 3-month period. The total score comprises missed work and school days, days at work and school or household work where productivity was reduced by half, missed household workdays, and missed nonwork activity days due to headache. EQ VAS is a generic measure for assessing general health status that records an individual's self-reported health on a scale from 0 (“best imaginable health state”) to 100 (“worst imaginable health state”). Additionally, safety evaluations in both studies included the incidence of adverse events (AEs), serious AEs, and AEs leading to discontinuation. Safety outcomes included treatment-emergent adverse events (TEAEs) and adverse events (AEs) leading to discontinuation.
Due to differences in the time points or definitions between the outcomes in RELEASE and BHV3000-309, some efficacy outcomes were evaluated using multiple definitions. Change from baseline in mean MMDs was evaluated across 3 time points; weeks 1 to 12 (primary endpoint in RELEASE and secondary endpoint in BHV3000-309), weeks 9 to 12 (prespecified additional endpoint in RELEASE and primary endpoint in BHV3000-309), and weeks 1 to 4 (prespecified additional endpoint in RELEASE and secondary endpoint in BHV3000-309). Acute medication use days was evaluated using two definitions; change from baseline in mean monthly acute medication use days at weeks 1 to 12 (secondary endpoint in RELEASE) compared to number of monthly acute medication use days across weeks 9 to 12 (secondary endpoint in BHV3000-309), and change from baseline in mean monthly acute medication use days at weeks 9 to 12 (prespecified additional endpoint in RELEASE) compared to number of monthly acute medication use days across weeks 9 to 12. Change from baseline in MSQ v2.1 RFR domain score was evaluated at week 12 (secondary endpoint in RELEASE and BHV3000-309). Change from baseline in MIDAS total score was evaluated at week 12 (prespecified additional endpoint in RELEASE and secondary endpoint in BHV3000-309). Change from baseline in EQ VAS score was evaluated at week 12 (prespecified additional endpoint in RELEASE and secondary endpoint in BHV3000-309). TEAEs and AEs leading to discontinuation were evaluated across the 12-week double-blind treatment periods.
The NNT to result in one additional person achieving a ≥ 50% reduction from baseline in MMDs/MHDs for atogepant 60 mg and rimegepant 75 mg was calculated using registrational trial data from RELEASE and BHV3000-309. The NNTs for atogepant versus placebo were calculated based on the responder definition of ≥50% reduction from baseline in mean MMDs across weeks 1 to 12 (definition 1) (secondary endpoint in RELEASE). The NNTs for rimegepant versus placebo were calculated based on the responder definition of ≥50% reduction from baseline of mean moderate or severe MMDs during weeks 9 to 12 (secondary endpoint in BHV3000-309). To account for differences in responder definitions in the secondary endpoints between the atogepant and rimegepant trials, the NNT versus placebo was calculated across 2 additional responder definitions for atogepant: definition 2, ≥ 50% reduction from baseline in mean MMDs across weeks 9 to 12; definition 3, ≥ 50% reduction from baseline of mean moderate or severe MHDs during weeks 9 to 12. Definition 2 was a prespecified additional endpoint in RELEASE and definition 3 was a post hoc analysis. The NNTs for each responder definition for atogepant were compared with the NNT for rimegepant.
Statistical analyses
The ITC analyses for efficacy outcomes were based on the modified intent-to-treat (mITT) population from RELEASE (defined as all randomized participants who had an evaluable baseline period, received ≥1 dose of study drug, and had ≥1 evaluable postbaseline 4-week period of eDiary data) and the double-blind treatment migraine analysis set from BHV3000-309 (defined as all randomized participants who received ≥1 dose of study drug, with ≥14 days [not necessarily consecutive] of eDiary efficacy data in both the observation phase and ≥1 month [4-week interval] of the double-blind treatment phase). For the ITC analyses of continuous change from baseline endpoints, the mean differences between treatment arms were estimated by meta-analyses using random effects models. The least squares mean differences (LSMDs) compared with placebo and the standard errors of the LSMDs were used as inputs to the network meta-analyses. Standard errors of the LSMDs were not reported for the rimegepant trial, so they were estimated from the 95% confidence intervals (CIs) assuming the LSMDs were normally distributed. The meta-analyses were performed using the netmeta and pairwise functions of the netmeta package (version 2.9-0) in R version 4.42 (R Foundation for Statistical Computing) within the RStudio version 2024.12.0 environment (RStudio, PBC, Boston, MA, USA). Statistical comparisons are presented as P-values with P < 0.05 defined as a statistically significant outcome.
The ITC analyses for safety and tolerability outcomes were based on the safety population from RELEASE (defined as all participants who received ≥1 dose of study drug during the double-blind treatment period) and the double-blind treatment safety analysis set from BHV3000-309 (defined as all participants who received ≥1 dose of study drug during the double-blind treatment phase). A Bayesian meta-analysis of percent incidence for placebo was conducted to estimate the placebo hazard rate. Hazard ratios (HRs) were calculated using the frequentist approach of the ratio of observed counts over expected counts, as previously detailed. 25 Frequentist methodology using the R package netmeta implements inverse-variance network meta-analyses to compare the HRs of atogepant and rimegepant. Because there are no repeated treatments, the random effects and fixed effects models are equivalent, thus the between trial heterogeneity is estimated at 0.
For the NNT analyses, the log odds of response for placebo and the log odds ratios (ORs) for atogepant and rimegepant versus placebo were estimated by meta-analyses using random effects models. Estimates of the response rates and 95% CIs were derived by converting the log odds estimates and corresponding 95% CIs to probabilities. Statistical analyses of response rates were performed using the MetaProp and metabin functions of the meta package (version 8.0-1) in R version 4.4.2 within the RStudio version 2024.12.0 environment. The NNT was calculated using the following formula: 1 ÷ [(probability of prespecified clinical response at a prespecified time point with treatment) − (probability of same prespecified clinical response at same time point with placebo)], and CIs of the NNTs were estimated by 10,000 iterations using a Monte Carlo simulation.
Results
Participant demographics and trial comparison
The safety population in the double-blind treatment period in RELEASE included 523 participants (atogepant 60 mg, n = 132; placebo, n = 134) and BHV3000-309 included 496 participants (rimegepant 75 mg, n = 247; placebo, n = 249). The mITT population in RELEASE included 521 participants (atogepant 60 mg, n = 131; placebo, n = 133) and the efficacy-evaluable population in BHV3000-309 included 484 participants (rimegepant 75 mg, n = 240; placebo, n = 244). The baseline demographics between the efficacy populations of RELEASE and BHV3000-309 were similar. Mean age was 42.5 to 44.8 years, 83.3% to 91.7% were female, and 100% were Japanese. Participants in the mITT population of RELEASE had baseline mean MMDs of 7.2 (placebo) and 7.1 (atogepant 60 mg) days and participants in the efficacy-evaluable population of BHV3000-309 had baseline mean MMDs of 8.4 (placebo) and 8.3 (rimegepant 75 mg) days (Table 1).
Baseline characteristics.
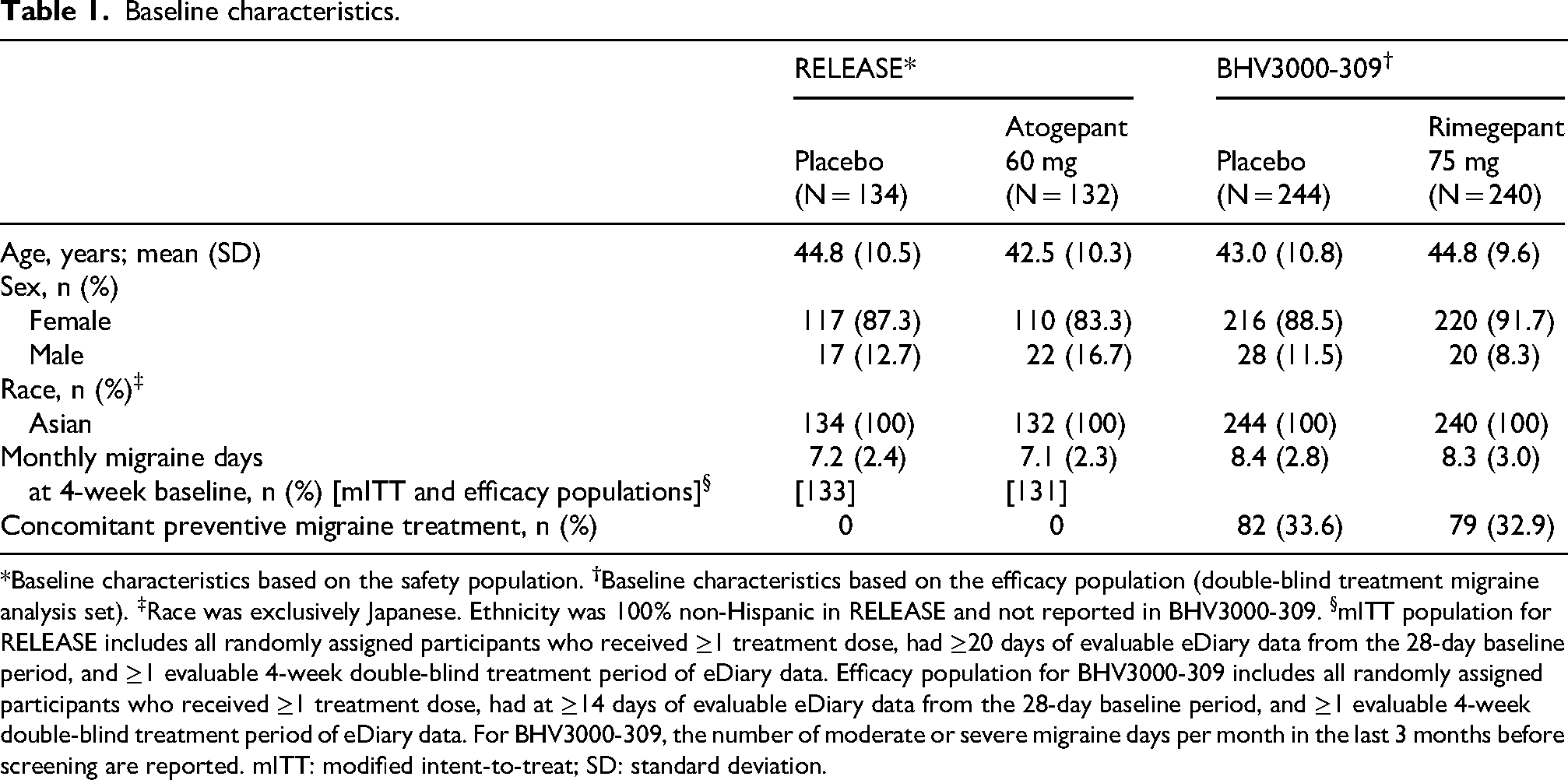
*Baseline characteristics based on the safety population.
Comparative efficacy, safety, and tolerability
Supplemental Table 2 presents the efficacy outcomes (mean MMDs, mean monthly acute medication use days, MSQ v2.1 RFR domain score, MIDAS total score, and EQ VAS score) from RELEASE and BHV3000-309. Baseline MMDs at the 4-week baseline were 7.2 for placebo and 7.1 for atogepant 60 mg in RELEASE, and baseline number of moderate to severe migraine attacks per month were 8.4 for placebo and 8.3 for rimegepant in BHV3000-309. Atogepant 60 mg demonstrated significantly higher reduction from baseline in mean MMDs compared with placebo (mean difference [MD] −2.10, 95% CI: −2.77 to −1.43; P < 0.0001) and numerically higher mean MMD reduction from baseline compared with rimegepant 75 mg (MD: −0.60, 95% CI: −1.47 to 0.27; P = 0.18) across weeks 1 to 12. Mean MMD reduction across weeks 9 to 12 and 1 to 4 was consistent with weeks 1 to 12 (Figure 1). Additionally, atogepant 60 mg demonstrated significantly higher reduction from baseline in mean monthly acute medication use days compared with placebo (MD: −2.48, 95% CI: −3.15 to −1.81; P < 0.0001) and compared with rimegepant 75 mg (MD: −1.68, 95% CI: −2.72 to −0.64; P = 0.002) across weeks 1 to 12. Reduction in mean monthly acute medication use days across weeks 9 to 12 was consistent with weeks 1 to 12 (Figure 2).

Mean difference in change from baseline in mean monthly migraine days for atogepant 60 mg compared with placebo and rimegepant 75 mg at weeks 1 to 4, 9 to 12, and 1 to 12. Atogepant versus rimegepant comparison presented as mean treatment difference (95% confidence interval).

Mean difference in change from baseline in mean monthly acute medication use days for atogepant 60 mg compared with placebo and rimegepant 75 mg at weeks 9 to 12 and 1 to 12. Atogepant versus rimegepant comparison presented as mean treatment difference (95% confidence interval). *P < 0.05.
Atogepant 60 mg demonstrated significantly greater improvement from baseline in MSQ v2.1 RFR domain score compared with placebo (MD: 9.23, 95% CI: 5.87 to 12.59; P < 0.0001) and compared with rimegepant 75 mg (MD: 5.13, 95% CI: 1.10 to 9.16; P = 0.01) at week 12. For MIDAS total score, atogepant 60 mg demonstrated significantly greater reduction (i.e. improvement) from baseline compared with placebo (MD: −4.91, 95% CI: −8.58 to −1.24; P = 0.009) and numerically greater reduction (i.e. improvement) compared with rimegepant 75 mg (MD: −2.51, 95% CI: −6.99 to 1.97; P = 0.27) at week 12. Additionally, there was no difference between atogepant 60 mg and placebo in EQ VAS scores (MD: 0.13, 95% CI: −3.21 to 3.47; P = 0.94) and a numerically lower improvement from baseline compared with rimegepant 75 mg (MD: −2.57, 95% CI: −6.97 to 1.83; P = 0.25) at week 12 (Figure 3).

Mean difference in change from baseline at week 12 in MSQ v2.1 RFR domain score, MIDAS total score, and EQ VAS score for atogepant 60 mg compared with placebo and rimegepant 75 mg. Atogepant versus rimegepant comparison presented as mean treatment difference (95% confidence interval). Greater changes from baseline in MSQ v2.1 RFR domain score and EQ VAS score and reductions from baseline in MIDAS total score signify improvements in these respective outcomes. *P < 0.05. EQ VAS, European Quality of Life Visual Analogue Scale; MIDAS, Migraine Disability Assessment; MSQ v2.1, Migraine-Specific Quality of Life Questionnaire version 2.1; RFR, Role Function-Restrictive.
Supplemental Table 3 presents the TEAEs and AEs leading to discontinuation from RELEASE and BHV3000-309. The full safety analyses have been previously reported.14,15 The HR (95% CI) for atogepant 60 mg compared with placebo was 0.93 (0.65 to 1.34) for TEAEs and 1.02 (0.09 to 11.86) for AEs leading to discontinuation. The HR (95% CI) for rimegepant 75 mg compared with placebo was 1.33 (1.03 to 1.72) for TEAEs and 2.02 (0.41 to 9.99) for AEs leading to discontinuation. Atogepant 60 mg demonstrated a numerically lower likelihood of TEAEs (HR: 0.70, 95% CI: 0.45 to 1.09; P = 0.12) and AEs leading to discontinuation (HR: 0.50, 95% CI: 0.03 to 9.46; P = 0.65) compared with rimegepant 75 mg (Figure 4).

Hazard ratio of treatment-emergent adverse events and adverse events leading to discontinuation for atogepant 60 mg compared with placebo and rimegepant 75 mg. CI, confidence interval.
All outcomes comparing atogepant 10 and 30 mg with rimegepant 75 mg were generally consistent with atogepant 60 mg except atogepant 10 mg EQ VAS score. Atogepant 10 mg demonstrated numerically greater improvement in EQ VAS score at week 12 relative to rimegepant 75 mg (Supplemental Figures 1–3).
Number needed to treat
The adjusted ≥50% responder rates from RELEASE and BHV3000-309 are reported in Supplemental Table 4. NNT was analyzed across three definitions for responder rates. For responder definition 1 (≥50% reduction from baseline in mean MMDs across weeks 1–12), the median NNT (95% CI) versus placebo was 2.5 (1.9 to 4.1) for atogepant 60 mg and 16.6 (6.7 to ∞) for rimegepant 75 mg, with a difference between rimegepant 75 mg and atogepant 60 mg of 14.4. The OR (95% CI) for a response compared with placebo was 5.74 (3.19 to 10.31) for atogepant 60 mg and 1.36 (0.94 to 1.97) for rimegepant 75 mg. The results from responder definition 2 (≥50% reduction from baseline of mean MMDs during weeks 9–12) and responder definition 3 (≥50% reduction from baseline of mean monthly moderate or severe MHDs during weeks 9–12) were consistent with responder definition 1 (Figure 5). The NNTs of atogepant 10 mg and 30 mg versus placebo were consistent with atogepant 60 mg (Supplemental Figures 4 and 5).

Median number needed to treat for one additional person to achieve a ≥ 50% reduction from baseline in responder definitions 1, 2, and 3 for atogepant 60 mg compared with rimegepant 75 mg. CI, confidence interval; OR, odds ratio.
Discussion
We report here an ITC and NNT analysis of atogepant and rimegepant for the preventive treatment of EM in Japanese participants. Atogepant 60 mg demonstrated significantly greater reduction from baseline in mean monthly acute medication use days and a significant improvement from baseline in MSQ v2.1 RFR domain score relative to rimegepant 75 mg. In addition, atogepant 60 mg demonstrated numerically greater reduction from baseline in mean MMDs, numerically greater reduction (i.e. improvement) from baseline in MIDAS total score, and numerically lower improvement from baseline in EQ VAS score compared with rimegepant 75 mg. For safety and tolerability, atogepant 60 mg demonstrated numerically lower TEAEs and AEs leading to discontinuation compared with rimegepant 75 mg (all numerical differences P > 0.05). Atogepant 60 mg had substantially lower NNTs resulting in one additional person achieving a ≥ 50% reduction from baseline in MMDs/MHDs versus placebo than rimegepant 75 mg. An additional 7 to 14 individuals would need to be treated with rimegepant 75 mg to result in a comparable response with atogepant 60 mg. Collectively, atogepant 60 mg demonstrated significantly or numerically greater improvements in four of five efficacy outcomes, a lower likelihood of TEAEs and AEs leading to discontinuation, and lower NNTs versus placebo relative to rimegepant 75 mg. All outcomes comparing atogepant 10 and 30 mg to rimegepant 75 mg were generally consistent with atogepant 60 mg.
Head-to-head trials are the gold standard for comparative analyses; however, currently, there are a limited number of head-to-head trials comparing CGRP preventive treatments. A phase 4, randomized, 3-month, double-blind, double-dummy, parallel-group study evaluating galcanezumab and rimegepant for the preventive treatment of EM found no significant differences in any efficacy or safety outcomes. 26 In the absence of more head-to-head comparisons of CGRP preventive treatments, ITC analyses have been used to compare CGRP mAbs and gepants for the preventive treatment of migraine. A MAIC evaluating erenumab and rimegepant found that erenumab was associated with statistically significant reductions in MMDs at month 3 relative to rimegepant. 27 A second MAIC comparing galcanezumab, erenumab, and rimegepant found no difference in MMD reduction between rimegepant and either CGRP mAb. 28 A third MAIC comparing atogepant and rimegepant using registrational data from the ADVANCE, PROGRESS, and BHV3000-305 trials found that atogepant treatment was associated with a significantly greater reduction in mean MMDs compared with rimegepant. 21 Currently, there are no direct treatment comparisons for migraine preventive treatments in Japanese participants. Here, we report the first comparative analyses between atogepant and rimegepant for the preventive treatment of EM in Japanese participants. The greater improvements in efficacy outcomes and lower likelihood of TEAEs and AEs leading to discontinuation with atogepant 60 mg compared with rimegepant 75 mg may help guide clinical decision making for the preventive treatment of migraine.
NNT can be used as a comparative tool for evaluating the potential benefits of treatments, and an NNT value <10 is generally considered a useful predictor of whether a treatment is likely to have a clinically meaningful benefit to patients.16,29,30 The median NNT for all doses of atogepant was consistently <7, whereas the median NNT for rimegepant was 13.3 to 16.6. Caution is needed when comparing NNT values in these analysis with other studies; however, previous ITCs including preventive treatments for EM have reported NNTs ranging from 4 to 10 across trials for CGRP mAbs.17,18 Additionally, two previous analyses have used NNT as a comparative tool to evaluate atogepant relative to CGRP mAbs and rimegepant. One NNT analysis based on ≥50% responder rates comparing atogepant and the CGRP mAbs found that NNT values were comparable between treatments. 22 A second NNT analysis based on ≥50% responder rates between atogepant and rimegepant from the US trials, ADVANCE and BHV3000-305, found that atogepant 60 mg had substantially lower NNTs versus placebo compared with rimegepant 75 mg for the preventive treatment of EM. 20 Here we report that atogepant 60 mg also had substantially lower NNTs compared with rimegepant 75 mg for the preventive treatment of EM in Japanese participants.
Limitations
Results from comparisons of clinical trials should be interpreted with caution as the results may not be generalizable. The RELEASE and BHV3000-309 trials had differences in study populations and endpoint definitions. The study population in RELEASE only included participants with a diagnosis of EM at baseline. This differed from the BHV3000-309 trial which included participants with 4 to 18 migraine attacks of moderate to severe intensity per month in the past 3 months prior to screening and ≥4 MMDs but ≤18 MHDs at baseline. In BHV3000-309, 30.2% of participants had historical CM. Regardless, the MMDs at baseline were comparable between the trials and treatment groups. In BHV3000-309, a subgroup analysis was performed evaluating the change from the observation period in the number of MMDs between the subgroup with historical CM and the subgroup without historical CM. Their results were similar between these subgroups, suggesting a history of CM would not significantly impact the results presented here. Additionally, RELEASE excluded the concomitant use of a migraine preventive medication during the study, whereas BHV3000-309 allowed the use of one migraine preventive medication, excluding CGRP mAbs and gepants. In BHV3000-309, 33.3% of participants were on a stable preventive migraine medication through randomization. This may suggest a more severe patient population in the BHV3000-309, but baseline clinical characteristics were similar, including MMDs at baseline. In BHV3000-309, a subgroup analysis was performed evaluating the change from the observation period in the number of MMDs between the subgroup with stable preventive migraine medication and the subgroup without stable preventive migraine medication. The subgroup with stable preventive migraine medication had a greater reduction in MMDs compared to those without, which would have a conservative impact on the results presented here.
The assessed time points for the MMD endpoint, and time point and definition of the monthly acute medication use day endpoint differed between the RELEASE and BHV3000-309 trials. The ITC analyses included multiple comparisons across different time points to account for these differences, and results were consistent between all time points. The NNT results are dependent on the ≥50% responder rates in RELEASE and BHV3000-309, which were prespecified secondary endpoints and differed between trials. Three responder definitions were used to compare NNTs for atogepant and rimegepant to address this potential limitation, and results for all responder definitions were consistent. ORs were used to quantify the relative effects of atogepant and rimegepant versus placebo. This approach is consistent with best practices for meta-analyses and assumes the placebo arms between the two trials are comparable. Despite the limitations, these analyses add to the limited literature on comparative analyses between gepants. Future research could explore direct comparative analyses or trials between migraine preventive treatments in the Japanese population.
Conclusions
Among Japanese participants with EM, atogepant 60 mg demonstrated significantly greater reductions in mean monthly acute medication use days and significantly greater improvements in MSQ v2.1 RFR domain score compared with rimegepant 75 mg. Additionally, atogepant demonstrated greater reductions in mean MMDs, greater reductions (i.e. improvements) in MIDAS, lower improvements in EQ VAS score, and a lower likelihood of TEAEs and AEs leading to discontinuation compared with rimegepant 75 mg. Atogepant 60 mg had substantially lower NNTs versus placebo than rimegepant 75 mg. An additional 7 to 14 individuals would need to be treated with rimegepant 75 mg to result in a comparable response with atogepant 60 mg.
Article highlights
Atogepant demonstrated significantly greater reduction in mean monthly acute medication use days and significant improvement in MSQ v2.1 RFR domain score compared with rimegepant in Japanese participants with EM.
Atogepant had a lower likelihood of TEAEs and AEs leading to discontinuation compared with rimegepant.
Atogepant had substantially lower NNTs for one additional ≥50% responder versus placebo compared with rimegepant.
Supplemental Material
sj-docx-1-rep-10.1177_25158163251399924 - Supplemental material for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis
Supplemental material, sj-docx-1-rep-10.1177_25158163251399924 for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis by Takao Takeshima, Yasuhiko Matsumori, Gina Ahmadyar, Pranav Gandhi, Kari Kelton, Toru Yamazaki, Karen Carr, Krisztian Nagy and Jessica Ailani in Cephalalgia Reports
Supplemental Material
sj-docx-2-rep-10.1177_25158163251399924 - Supplemental material for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis
Supplemental material, sj-docx-2-rep-10.1177_25158163251399924 for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis by Takao Takeshima, Yasuhiko Matsumori, Gina Ahmadyar, Pranav Gandhi, Kari Kelton, Toru Yamazaki, Karen Carr, Krisztian Nagy and Jessica Ailani in Cephalalgia Reports
Supplemental Material
sj-docx-3-rep-10.1177_25158163251399924 - Supplemental material for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis
Supplemental material, sj-docx-3-rep-10.1177_25158163251399924 for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis by Takao Takeshima, Yasuhiko Matsumori, Gina Ahmadyar, Pranav Gandhi, Kari Kelton, Toru Yamazaki, Karen Carr, Krisztian Nagy and Jessica Ailani in Cephalalgia Reports
Supplemental Material
sj-docx-4-rep-10.1177_25158163251399924 - Supplemental material for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis
Supplemental material, sj-docx-4-rep-10.1177_25158163251399924 for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis by Takao Takeshima, Yasuhiko Matsumori, Gina Ahmadyar, Pranav Gandhi, Kari Kelton, Toru Yamazaki, Karen Carr, Krisztian Nagy and Jessica Ailani in Cephalalgia Reports
Supplemental Material
sj-docx-5-rep-10.1177_25158163251399924 - Supplemental material for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis
Supplemental material, sj-docx-5-rep-10.1177_25158163251399924 for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis by Takao Takeshima, Yasuhiko Matsumori, Gina Ahmadyar, Pranav Gandhi, Kari Kelton, Toru Yamazaki, Karen Carr, Krisztian Nagy and Jessica Ailani in Cephalalgia Reports
Supplemental Material
sj-docx-6-rep-10.1177_25158163251399924 - Supplemental material for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis
Supplemental material, sj-docx-6-rep-10.1177_25158163251399924 for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis by Takao Takeshima, Yasuhiko Matsumori, Gina Ahmadyar, Pranav Gandhi, Kari Kelton, Toru Yamazaki, Karen Carr, Krisztian Nagy and Jessica Ailani in Cephalalgia Reports
Supplemental Material
sj-docx-7-rep-10.1177_25158163251399924 - Supplemental material for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis
Supplemental material, sj-docx-7-rep-10.1177_25158163251399924 for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis by Takao Takeshima, Yasuhiko Matsumori, Gina Ahmadyar, Pranav Gandhi, Kari Kelton, Toru Yamazaki, Karen Carr, Krisztian Nagy and Jessica Ailani in Cephalalgia Reports
Supplemental Material
sj-docx-8-rep-10.1177_25158163251399924 - Supplemental material for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis
Supplemental material, sj-docx-8-rep-10.1177_25158163251399924 for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis by Takao Takeshima, Yasuhiko Matsumori, Gina Ahmadyar, Pranav Gandhi, Kari Kelton, Toru Yamazaki, Karen Carr, Krisztian Nagy and Jessica Ailani in Cephalalgia Reports
Supplemental Material
sj-docx-9-rep-10.1177_25158163251399924 - Supplemental material for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis
Supplemental material, sj-docx-9-rep-10.1177_25158163251399924 for Comparative efficacy, safety, and number needed to treat analysis of atogepant and rimegepant for the preventive treatment of episodic migraine in Japanese participants: An indirect comparison analysis by Takao Takeshima, Yasuhiko Matsumori, Gina Ahmadyar, Pranav Gandhi, Kari Kelton, Toru Yamazaki, Karen Carr, Krisztian Nagy and Jessica Ailani in Cephalalgia Reports
Footnotes
Acknowledgements
AbbVie and the authors thank all the trial investigators and the patients who participated in these clinical trials. Medical writing assistance was provided to the authors by Brian Neel, PhD, of AbbVie (North Chicago, IL, USA), and editorial assistance was provided to the authors by S. Michael Austin, BA, of AbbVie (North Chicago, IL, USA).
Ethical considerations
The trials were approved by a local or central Institutional Review Board at each participating institution and conducted in accordance with the International Conference for Harmonisation guidelines, applicable regulations, and the Declaration of Helsinki.
Consent to participate
Participants provided written informed consent before screening.
Consent for publishing
Consent for publication was obtained.
Author contributions
All authors had access to relevant data and participated in the drafting, review, and approval of this publication. No honoraria or payments were made for authorship.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AbbVie funded this study and participated in the study design, research, analysis, data collection, interpretation of data, reviewing, and approval of the publication.
Declaration of conflicting interests
The authors declare the following potential conflicts of interest with respect to the research, authorship and/or publication of this article:
Data availability statement
AbbVie is committed to responsible data sharing regarding the clinical trials we sponsor. This includes access to anonymized, individual, and trial-level data (analysis data sets), as well as other information (e.g. protocols, clinical study reports, or analysis plans), as long as the trials are not part of an ongoing or planned regulatory submission. This includes requests for clinical trial data for unlicensed products and indications. These clinical trial data can be requested by qualified researchers who engage in rigorous, independent, scientific research, and will be provided following review and approval of a research proposal, Statistical Analysis Plan, and execution of a Data Sharing Agreement. Data requests can be submitted at any time after approval in the United States and Europe and after acceptance of this manuscript for publication. The data will be accessible for 12 months, with possible extensions considered. For more information on the process or to submit a request, visit the following link: ![]() then select “Home.”
then select “Home.”
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.