
Abstract
Objective:
This randomized, partially-blinded, placebo-controlled study evaluated hemodynamic effects, pharmacokinetic interactions, and safety of concomitant administration of oral rimegepant and subcutaneous sumatriptan.
Methods:
Healthy non-smokers aged ≥18 and ≤40 years (men) or ≥18 and ≤50 years (women) were enrolled. On Day 1, subjects received 12 mg of sumatriptan as 2 subcutaneous 6 mg injections separated by 1 hour. From Days 2 to 4, subjects received rimegepant or placebo once daily (randomized 6 to 1, rimegepant to placebo). On Day 5, subjects received rimegepant or placebo, followed 2 hours later by 2 subcutaneous 6 mg injections of sumatriptan, separated by 1 hour. Sumatriptan was administered at the same times as on Day 1.
Results:
All 42 dosed subjects were analyzed. There were no significant differences in the time-weighted average of mean arterial pressure, diastolic blood pressure, or systolic blood pressure between treatment with rimegepant + sumatriptan and sumatriptan alone. Co-administration of rimegepant and sumatriptan had no effect on the pharmacokinetics of either drug. Overall, 93% (39/42) of subjects experienced ≥1 adverse event; injection site reaction was most common (60% [29/42]).
Conclusions:
Concomitant administration of oral rimegepant and subcutaneous sumatriptan to healthy adults was without hemodynamic or pharmacokinetic interaction and was safe and well tolerated.
Introduction
Rimegepant (Nurtec ODT, Biohaven Pharmaceuticals, New Haven, CT, USA) is an orally-administered small molecule calcitonin gene-related peptide receptor (CGRP) antagonist with demonstrated efficacy and safety in the acute treatment of migraine in 3 Phase 3 clinical trials. 1 –3 It was approved by the US Food and Drug Administration for the acute treatment of migraine in adults in February 2020. 4 In previous research, including a long-term safety study with 1800 patients with migraine taking rimegepant 75 mg for up to 1 year, 5 no clinically significant effects on blood pressure were observed. Rimegepant has also demonstrated efficacy and safety as a preventive treatment for migraine when dosed every other day in a 12-week randomized, double-blind, placebo-controlled Phase 2/3 trial; during this trial, triptans were permitted to be taken as acute treatment for migraine if needed. 6
Rimegepant has rapid absorption (Tmax of 1.5 hours with the orally disintegrating tablet) followed by a rapid distribution phase with an approximately 11-hour terminal elimination half-life. 4 The compound is primarily metabolized by cytochrome P450 (CYP) 3A4 and eliminated predominantly in unchanged form with no major circulating metabolites in plasma. Rimegepant undergoes no significant accumulation and is neither an inducer nor a clinically significant inhibitor of metabolism. Clinically significant pharmacokinetic (PK) interactions with sumatriptan are unlikely based on the properties of the 2 drugs.
While rimegepant monotherapy is expected to meet the needs of patients with migraine, the acute treatment of a migraine attack may involve exposure to rimegepant and sumatriptan due to sequential or concomitant use of both drugs. The possibility of concomitant use also heightens the importance of understanding the potential for PK or pharmacodynamic interactions, especially cardiodynamic interactions based on the known risk of triptans to increase blood pressure. Sumatriptan was selected as a representative triptan for this interaction study with rimegepant based on sumatriptan’s widespread use and well defined hemodynamic properties. 7
The primary objective of this study was to evaluate the effect of rimegepant on resting blood pressure when administered concomitantly with sumatriptan in healthy volunteers. Secondary objectives included assessing the presence of any PK interactions between sumatriptan and rimegepant; evaluating the effects of rimegepant on resting blood pressure compared with placebo; and assessing the safety and tolerability of co-administered rimegepant and sumatriptan.
Methods
Oversight
This study complied with Good Clinical Practices and Good Laboratory Practices referenced in the International Council for Harmonization guidelines, all applicable federal and local regulations, and any independent ethics committee requirements relative to clinical studies. Subjects provided written informed consent before any study-related procedures were undertaken. The protocol was approved by a central Institutional Review Board (Pro00030237, Advarra IRB, Columbia, MD, USA).
Study conduct
This single-center, Phase 1, randomized, partially-blinded, placebo-controlled study in healthy fasted adults had 3 phases: a 28-day screening phase, 5-day treatment phase, and a 1-day end of study/early termination phase (Figure 1). Screening procedures included collection of demographic data; medical and medication histories; complete physical examination; injection site evaluation; Sheehan Suicidality Tracking Scale (S-STS); 8 body measurements; 12-lead electrocardiogram (ECG); vital signs (blood pressure, heart rate, and respiratory rate); oral temperature; hematology; biochemistry; tests for human immunodeficiency virus, hepatitis B surface antigen, and hepatitis C virus; urinalysis; urine cotinine test; alcohol breath test; urine pregnancy test; and urine drug screen. After the screening phase, upon arrival at the study site for confinement (Day −1), subjects meeting eligibility criteria were randomly assigned (6:1) to rimegepant or placebo. On Day 1, sumatriptan succinate (Taro Pharmaceuticals Inc., ON, Canada) was administered as 2 subcutaneous (SC) injections of 6 mg/0.5 mL separated by approximately 1 hour, for a total dose of 12 mg. On Days 2, 3, and 4, rimegepant 75 mg or placebo were administered once daily. On Day 5, rimegepant 75 mg or placebo tablets were administered; approximately 2 and 3 hours later (i.e. separated by approximately 1 hour), 2 SC sumatriptan injections of 6 mg/0.5 mL were administered corresponding to the same times as Day 1 sumatriptan administration.

Study Design. SC, subcutaneous. †After a manual pre-dose recording, collected with an automated blood pressure monitoring system every 10 minutes for the first 4 hours post-dose, every 30 minutes for the next 2 hours post-dose, and every 60 minutes for the last 9 hours post-dose. An additional blood pressure recording was made at 24 hours post-dose on Days 2, 5, and 6. ‡Of sumatriptan.
Each subject participated for approximately 5 weeks, including the screening period. Subjects were confined to the research facility from Day −1, at least 10 hours before the first study treatment administration, until the morning of Day 6. On Day 1, no food was allowed from at least 2 hours before the first sumatriptan injection until at least 1 hour after the second sumatriptan injection. On Days 2 to 5, no food was allowed from at least 10 hours before until at least 4 hours after rimegepant or placebo dosing, and no fluids were allowed from 1 hour before until 1 hour after rimegepant or placebo dosing (except for water given with study medication). Water was provided as desired at all other times.
On Days 1, 4, and 5, subjects were required to remain seated and avoid lying down or sleeping for 4 hours after all drug administrations were completed, except if medically necessary, procedurally required, or to use the bathroom. When allowed, subjects were accompanied by a staff member during ambulations. On Days 2 and 3, subjects were allowed to engage in normal activity but were required to avoid lying down or sleeping, unless medically necessary or procedurally required, for 2 hours after drug administration.
Subjects
Eligible subjects were men aged 18–40 years, inclusive, and women aged 18–50 years, inclusive. Subjects were non-smokers with a body mass index between 18.5 and 30.0 kg/m2, a body weight ≥ 50.0 kg (men) and ≥ 45.0 kg (women), no clinically significant illness or surgery within 4 weeks before dosing, and a score of 0 on the S-STS at screening. Women of childbearing potential having a non-sterile male sexual partner agreed to use an acceptable method of contraception throughout the study and for 8 weeks after the last study drug administration. Men who were not vasectomized at least 6 months before study drug administration and who were sexually active with a non-sterile female partner agreed to use acceptable contraceptive methods throughout the study and for 90 days after the last study drug administration.
Subjects were excluded if they had a clinically significant medical history, concurrent diseases, physical and laboratory test findings, or any reason likely to interfere with successful completion of the dosing procedure.
Detailed inclusion and exclusion criteria are provided in Table e-1.
Treatment assignments
On Day −1, subjects were randomly assigned (6:1, rimegepant:placebo) subject numbers that corresponded to a randomization scheme previously computer-generated using SAS (Cary, NC, USA).
Dose selection
Rimegepant dose selection was based on data from previous research that identified 75 mg as the optimal efficacious dose. 9 Sumatriptan total dose selection was the maximum recommended dose that may be administered within 2 hours. 10 On Day 5, the 2 sumatriptan injections were administered approximately 2 and 3 hours after rimegepant or placebo so the active drugs would achieve maximum observed concentration (Cmax) at approximately the same time, and maximal potential concomitant effects on blood pressure could be assessed.
Blinding
Since sumatriptan was administered as an SC injection, only rimegepant and placebo were administered in a double-blinded fashion. To preserve the blind, rimegepant and placebo tablets were identical in size and appearance; subjects and personnel who might influence the outcome of the study were blinded to treatment assignments. Blinding was maintained at least until investigation and reporting of all AEs had been completed for all subjects. Designated pharmacy personnel at the clinical site not directly involved with the clinical aspects of the trial prepared and dispensed the study drugs and were aware of the randomization code.
Prior and concomitant therapy
Concomitant medication use was documented from screening through study exit/early termination. No concomitant medications were allowed during the 5 days of study drug administration, except those required for the medical management of an AE. Subjects were also prohibited from taking monoamine oxidase inhibitors from 30 days before the first dose of sumatriptan on Day 1 until 14 days after the second dose of sumatriptan on Day 5. Treatment compliance was ensured by direct supervision of subjects during dosing, pre-dose verification of subject identity, and visual confirmation that subject identifications matched the labels on pre-dispensed medications.
Outcomes
Blood pressure parameters were mean arterial pressure (MAP), diastolic blood pressure (DBP), and systolic blood pressure (SBP). The primary objective was to evaluate the effect on resting blood pressure of rimegepant when administered concomitantly with sumatriptan, as determined by comparing blood pressure measurements after treatment with rimegepant and sumatriptan on Day 5 with sumatriptan alone on Day 1.
Plasma concentrations of rimegepant on Days 4 and 5 and sumatriptan on Days 1 and 5 were used to calculate the following PK parameters by standard noncompartmental methods: area under the concentration-time curve (AUC) from time 0 to time of last non-zero concentration (AUC0–t), AUC from time 0 to timepoint 24 hours (AUC0–24), AUC from time 0 to infinity (AUC0–inf), residual area, Cmax, time of observed Cmax (Tmax), elimination half-life (t½ el), and elimination rate constant (Kel).
Safety was evaluated through the assessment of AEs; clinical laboratory parameters (biochemistry, hematology, and urinalysis); 12-lead ECG; vital signs; S-STS; physical examination; and injection site evaluation. Data about AEs were collected and documented during the course of the study and for 4 days following the last study drug administration. Subjects experiencing AEs (including those withdrawn) were monitored until complete resolution or until the investigator judged it safe to discontinue follow-up.
Assessments
Details regarding the assessment of blood pressure, PK, and safety are provided in Table e-2.
Statistical analysis
Analysis populations
The safety population included subjects who received at least 1 dose of any study medication. The blood pressure population comprised subjects who completed the study without major protocol violation and for whom the blood pressure profiles could be adequately characterized. The PK population included subjects who completed the study without major protocol violation, and for whom the PK profiles of sumatriptan and rimegepant could be adequately characterized.
Blood pressure
Using automated blood pressure recordings, the time-weighted averages for MAP, SBP, and DBP were computed for each subject using the data from pre-dose to 4 hours on Days 1, 4, and 5.
For the comparison of data from subjects who received sumatriptan on Day 1 and rimegepant plus sumatriptan on Day 5, the MAP, DBP, and SBP data were evaluated using the GLM (General Linear Models) procedure in SAS, with treatment and subject dosing group as fixed factors and subject as a random factor.
The differences in least squares means (rimegepant + sumatriptan on Day 5 − sumatriptan on Day 1) were determined based on pairwise comparison of untransformed time-weighted average of MAP, DBP, and SBP data at the alpha level of 0.05.
For the primary endpoint, the 2 treatments were declared as similar if the upper bound of the 90% confidence interval (CI) of the difference for time-weighted average MAP (rimegepant plus sumatriptan on Day 5 − sumatriptan on Day 1) was less than 5 mm Hg.
Pharmacokinetics
Concentration values below the lower limit of quantification were set to 0. Sumatriptan samples with no reportable pre-dose value were replaced by 0 and set to “missing” for tabulation, graphical representation, and calculation.
Actual post-dose sampling times were used to calculate PK parameters. Pre-dose sampling times of sumatriptan on Days 1 and 5 and rimegepant and placebo on Days 2 to 4 were reported as 0, and pre-dose sampling times of rimegepant and placebo on Day 5 were reported as −2 hours.
Plasma concentrations of rimegepant (Days 4 and 5) and sumatriptan (Days 1 and 5) were used to calculate AUC0–t, AUC0–24, AUC0–inf, residual area, Cmax, Tmax, t½ el, and Kel by standard noncompartmental methods for each day separately. Concentrations and PK parameters for subjects excluded from the PK population were excluded from statistical analyses.
The analysis of the effect of rimegepant multiple-dose on sumatriptan single-dose PK was performed using the GLM procedure in SAS, with treatment (sumatriptan on Day 1 and rimegepant + sumatriptan on Day 5), subject dosing group, treatment-by-group interaction term as fixed effects, and subject as a random effect on untransformed Tmax, Kel, and t½ el and on ln-transformed AUC0–24, AUC0–inf, and Cmax at the alpha level of 0.05.
Based on pairwise comparison of the ln-transformed AUC0–24, AUC0–inf, and Cmax data for sumatriptan, the rimegepant + sumatriptan:sumatriptan ratios of the geometric least squares means and 90% CIs were calculated by exponentiation.
Safety
The safety and tolerability of rimegepant, sumatriptan, and placebo were evaluated through the assessment of AEs; clinical laboratory parameters (biochemistry, hematology, and urinalysis); 12-lead ECG; vital signs; physical examination; and S-STS. Treatment-emergent AEs (TEAEs) were captured during the study and for 4 days following the last study drug administration. A TEAE with a start date and time during a given treatment was attributed to that treatment; events occurring across treatments (e.g. a TEAE worsening in severity) were evaluated individually. On Day 5, TEAEs starting after rimegepant or placebo administration and before the first sumatriptan injection were attributed to the corresponding treatment on Days 2–4.
The relationship of TEAEs to rimegepant and/or placebo and/or sumatriptan was classified as unrelated, remotely related, possibly related, and probably related. The severity of TEAEs was classified as mild, moderate, or severe. For the incidence of subjects who experienced TEAEs (frequency and the percentage of subjects), each subject could only contribute once to each of the incidence rates, regardless of the number of occurrences.
Sample size
Based on data from literature 11 describing the effects of erenumab and sumatriptan on blood pressure, the baseline standard deviation (SD) in the blood pressure variables of interest was estimated at 7 mm Hg. Assuming a within-subject correlation of 0, the SD for a within-subject difference would be approximately 10 mm Hg. With no shift in the true value of blood pressure, it was estimated that a population of at least 36 subjects would be needed to provide a 90% probability that the upper bound of a 2-sided 90% CI for the within-subject difference in blood pressure would be less than 5 mm Hg.
Results
Subjects
Beginning on 18 October 2018, 102 healthy subjects were screened; of these, 54 subjects were enrolled, and 42 subjects were dosed on Day 1 (Figure 2). The last study visit occurred on 11 December 2018. Among the 42 subjects who received at least 1 dose of any study medication, 88% (37/42) completed all treatment periods. Five subjects discontinued from the study: 3 due to AEs, 1 withdrew consent, and 1 by investigator decision.

Subject flowchart. †Eligible subjects who decided not to participate or who were not selected to participate because a sufficient number of subjects had already been enrolled. ‡Standby subjects enrolled to replace any who might have been withdrawn before dosing on Day 1.
Demographics and baseline characteristics are shown in Table 1. The safety population comprised 76% (32/42) men and 24% (10/42) women. Most subjects were white (86% [36/42]), mean (SD) age was 32.4 (7.0) years, and mean (SD) body mass index was 24.7 (2.8) kg/m2.
Demographics and other baseline characteristics.†

SD, standard deviation.
† Based on the last results (scheduled or unscheduled) obtained prior to the first subcutaneous injection of sumatriptan on Day 1.
Blood pressure
No statistically significant difference was detected between treatments with rimegepant + sumatriptan on Day 5 versus sumatriptan on Day 1 for the comparisons between time-weighted average of MAP, SBP, and DBP. The differences (90% CIs), based on least squares means, of time-weighted averages for rimegepant + sumatriptan:sumatriptan were −0.21 (−1.61 to 1.19) mm Hg for MAP, −0.80 (−3.07 to 1.48) mm Hg for SDP, and −0.06 (−0.93 to 0.82) mm Hg for DBP (Table 2).
Automated blood pressure time-weighted averages in the blood pressure population.

CI, confidence interval; TWA, time-weighted average; MAP, mean arterial pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Figure 3 illustrates the mean systolic blood pressure over time during the 4 hours after the first sumatriptan injection on Days 1 and 5 for the subjects who received sumatriptan and rimegepant and completed the 5-day treatment sequence.

Mean systolic blood pressure over the first 4 hours post-dose following sumatriptan on Day 1 and rimegepant + sumatriptan on Day 5.
Pharmacokinetics
Sumatriptan exposure on the parameters of AUC0–inf, AUC0–24, and Cmax was similar whether administered as 2 SC injections on Day 1 or as 2 SC injections following rimegepant administration on Day 5, and the 90% CIs for each parameter were between 0.80 and 1.25 (Table 3). Day 1 and Day 5 values for Tmax and t½ el were also similar.
Pharmacokinetics of sumatriptan on Days 1 and 5.

CI, confidence interval; AUC, area under the concentration-time curve; Cmax, maximum plasma concentration.
After co-administration of rimegepant and sumatriptan on Day 5, AUC and Cmax for rimegepant were modestly (<30%) higher than after administration of rimegepant alone on Day 4 (Table 4).
Pharmacokinetics of rimegepant on Day 4 and rimegepant + sumatriptan on Day 5.
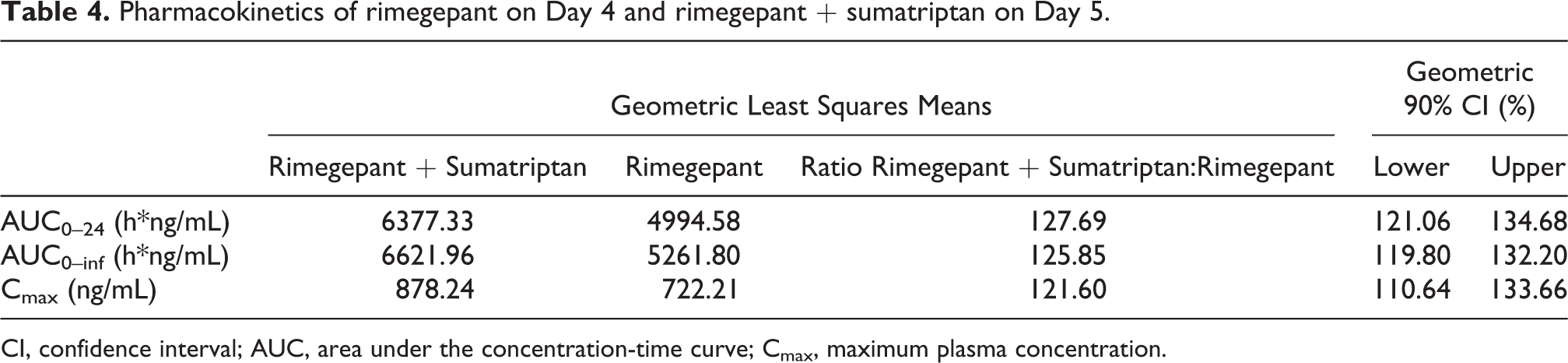
CI, confidence interval; AUC, area under the concentration-time curve; Cmax, maximum plasma concentration.
Safety
Thirty-nine (93%) subjects experienced at least 1 AE. The most frequently reported AEs (>1 subject in any treatment group) are shown in Table 5. Almost all AEs were mild in intensity (98% [188/191]); 3 subjects experienced moderate TEAEs. A majority of TEAEs resolved spontaneously by the end of the study. There were no deaths or serious AEs.
Treatment-emergent adverse events occurring in more than 1 subject† following treatment with rimegepant and sumatriptan.

AE, adverse event; TEAE, treatment-emergent adverse event.
AEs are presented in order of decreasing frequency during the study overall.
† In any treatment group.
‡Discontinued on Day 5, approximately 23 hours after taking rimegepant on Day 4.
Three subjects were discontinued from the study due to AEs. The first was an 18-year-old man who was randomized to rimegepant and who discontinued from the study on Day 1 due to a mild AE of palpitations after the first dose of sumatriptan. The second was a 38-year-old woman who was randomized to rimegepant and was discontinued from the study on Day 1 due to mild AEs of chest discomfort and injection site reaction after the first dose of sumatriptan. The third was a 22-year-old man, randomized to rimegepant, who was discontinued from the study on Day 5 (prior to the Day 5 dose of rimegepant) due to mild AEs of heart rate increased (121 beats per minute) and blood pressure increased (174/106 mm Hg) approximately 23 hours after he received the third dose of rimegepant on Day 4. The subject had received 2 doses of sumatriptan and 3 doses of rimegepant. No medication was given to treat these events, and after approximately 4 hours without treatment, they were considered resolved on the same day (supine blood pressure: 127/74 mm Hg; heart rate: 87 beats per minute). Heart rate and blood pressure measurements of the subject were normal at screening and study exit.
No clinically relevant changes were observed in laboratory parameters, hematology parameters, urinalysis, or vital sign measurements. No elevations were noted for liver function tests (alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, or bilirubin), and the results of ECGs were unremarkable. The S-STS total score was 0 for all subjects at screening and at study exit.
Discussion
This single-center, Phase 1, randomized, partially-blinded, placebo-controlled study in healthy adults evaluated the effect of rimegepant on resting blood pressure when administered concomitantly with sumatriptan. There were no significant differences between rimegepant + sumatriptan on Day 5 and sumatriptan on Day 1 on the time-weighted averages of MAP, SBP, and DBP. Because the upper bound of the 90% CIs for the difference between Day 5 and Day 1 was < 5 mm Hg, it was concluded that the time-weighted average of MAP between rimegepant and sumatriptan was similar. Administration of rimegepant produced no meaningful change in sumatriptan’s effects on blood pressure, even during peak systemic concentrations of both drugs, which indicates that concurrent exposure to both drugs is unlikely to represent a risk of increased blood pressure due to a pharmacodynamic interaction.
The study also assessed the PK of sumatriptan and rimegepant when administered alone and concomitantly. Based on the point estimates for AUC and Cmax, the PK of sumatriptan was similar when administered as 2 SC injections of 6 mg/0.5 mL on Day 1 or co-administered with rimegepant on Day 5. The concomitant use analyses showed that steady-state administration of rimegepant did not affect the single-dose PK of sumatriptan, and single-dose administration of sumatriptan did not have any clinically meaningful effect on the steady-state PK of rimegepant. The modest (<30%) increases noted with rimegepant do not require dose or frequency adjustment.
Since drugs in the triptan class are based on a common core structure (the indolealkylamine scaffold), exert their effects through agonism of serotonin receptors (5-HT1B and 5-HT1D), and share similar metabolic fates, 12 the absence of clinically significant hemodynamic effects or PK interactions observed in this study suggests that these results likely apply to the concomitant use of rimegepant with the triptan class. Of note, eletriptan is metabolized by CYP3A4 and is contraindicated within at least 72 hours of treatment with potent CYP3A4 inhibitors. 13 However, rimegepant is not a strong inhibitor of CYP3A4, and a clinically significant interaction between rimegepant and eletriptan is not likely. Since eletriptan has little potential to inhibit or induce CYP3A4, it is unlikely to cause clinically important drug interactions with rimegepant. 14 Moreover, because the comparator was the SC formulation of sumatriptan, which achieves the highest plasma concentrations and most rapid absorption, the study findings are likely to apply regardless of triptan formulation.
Evaluation of the safety and tolerability of rimegepant and sumatriptan showed that administration of rimegepant 75 mg once daily for 4 consecutive days and SC sumatriptan on Days 1 and 5 was safe and well tolerated in healthy adults. Co-administration of rimegepant on Day 5 with the maximum cumulative dose of sumatriptan that may be given SC in 24 hours (12 mg) removed the possibility of inadequate sumatriptan exposure to due to variable oral absorption. All TEAEs associated with rimegepant were mild, and only 3 sumatriptan-treated subjects had moderate TEAEs. These positive results confirm and extend previous findings showing that rimegepant has a favorable safety profile during acute and long-term use. Similarly favorable safety results were seen in the 12-week preventive treatment trial, in which triptan use was permitted during every other day administration of rimegepant. 6
Limitations of this study include the population of healthy volunteers and the use of sumatriptan as the sole comparator. Recognizing that migraine is a complex neurovascular disorder, caution is warranted when vasoconstrictive drugs such as triptans are administered to individuals with migraine. 15 The possibility exists that the effects of 5-HT1B/1D agonists and CGRP antagonists during migraine attacks may differ from those observed in this study. Additional clinical trials and real-world experience have not demonstrated safety concerns regarding the concomitant use of triptans and gepants or triptans and other classes of medication that block CGRP. 6,11,16 –18
Conclusions
Concomitant administration of rimegepant and sumatriptan was not associated with clinically significant hemodynamic effects or PK interactions in healthy adults. No significant difference in MAP, SBP, or DBP was detected between co-administration of rimegepant and sumatriptan compared with administration of sumatriptan alone. Steady-state administration of rimegepant 75 mg did not affect the single-dose PK of sumatriptan, and single-dose administration of sumatriptan did not have any clinically meaningful effect on the steady-state PK of rimegepant 75 mg. Rimegepant co-administered with sumatriptan was safe and well tolerated in healthy adults.
Clinical implications
The results from this study support the concomitant use of triptans and rimegepant, providing treatment flexibility
There were no clinically meaningful pharmacodynamic or PK interactions observed during concomitant exposure to sumatriptan and rimegepant
The absence of meaningful PK interaction potential and concomitant pressor effects is applicable across the triptan class
The positive safety and tolerability findings among rimegepant-treated subjects in this trial align with the consistently favorable results in previous single-attack and long-term clinical trials in adults with migraine
Supplemental material
Supplemental Material, sj-pdf-1-rep-10.1177_25158163211007922 - A phase 1 randomized study of hemodynamic effects and pharmacokinetic interactions during concomitant use of rimegepant and sumatriptan in healthy adults
Supplemental Material, sj-pdf-1-rep-10.1177_25158163211007922 for A phase 1 randomized study of hemodynamic effects and pharmacokinetic interactions during concomitant use of rimegepant and sumatriptan in healthy adults by Robert Croop, Andrea Ivans, Matt S Anderson, Joseph Stringfellow, Richard Bertz, Michael Hanna, Francine Healy, David A Stock, Vladimir Coric and Richard B Lipton in Cephalalgia Reports
Supplemental material
Supplemental Material, sj-pdf-2-rep-10.1177_25158163211007922 - A phase 1 randomized study of hemodynamic effects and pharmacokinetic interactions during concomitant use of rimegepant and sumatriptan in healthy adults
Supplemental Material, sj-pdf-2-rep-10.1177_25158163211007922 for A phase 1 randomized study of hemodynamic effects and pharmacokinetic interactions during concomitant use of rimegepant and sumatriptan in healthy adults by Robert Croop, Andrea Ivans, Matt S Anderson, Joseph Stringfellow, Richard Bertz, Michael Hanna, Francine Healy, David A Stock, Vladimir Coric and Richard B Lipton in Cephalalgia Reports
Footnotes
Acknowledgements
The authors are grateful to Christopher M. Jensen, PharmD, (Biohaven Pharmaceuticals, Inc., New Haven, CT, USA) for careful review of early versions of the manuscript. Medical writing services were provided by Christopher Caiazza.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Robert Croop, MD, is employed by and holds stock/stock options in Biohaven Pharmaceuticals. Andrea Ivans, MHS, is employed by and holds stock/stock options in Biohaven Pharmaceuticals. Matt S. Anderson, PhD, was a paid consultant of Biohaven Pharmaceuticals. Joseph Stringfellow, MS, was a paid consultant of Biohaven Pharmaceuticals. Richard Bertz, PhD, is employed by and holds stock/stock options in Biohaven Pharmaceuticals. Michael Hanna, MD, is employed by and holds stock/stock options in Biohaven Pharmaceuticals. Francine Healy, BS, is employed by and holds stock/stock options in Biohaven Pharmaceuticals. David A. Stock, PhD, is employed by and holds stock/stock options in Biohaven Pharmaceuticals. Vladimir Coric, MD, is employed by and holds stock/stock options in Biohaven Pharmaceuticals. Richard B. Lipton, MD, reports receiving honoraria as a consultant or speaker from Allergan/Abbvie, Amgen, Biohaven Holdings, Dr. Reddy's, Eli Lilly, GlaxoSmithKline, Grifols, Impel, Lundbeck, Merck, Novartis, Pernix, and Teva Pharmaceuticals. He receives research support from Allergan/Abbvie, Amgen, Eli Lilly, and Electrocore. He holds stock or options in Biohaven Holdings and CtrlM Health. In addition, he receives royalties from Oxford University Press (Wolff’s Headache and Other Head Pain, 7th Edition [2001] and 8th Edition [2007]), Wiley, and Informa.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Biohaven Pharmaceuticals, Inc.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.