
Abstract
Background and objectives
Primary headache disorders, particularly migraine, pose a significant public health challenge in the United States, marked by emergency department (ED) overuse, poor outcomes, and rising costs. Despite their utility in understanding disability, semistructured interviews are underutilized for identifying areas of improvement in system-based care. This project sought to capture patient perspectives on optimizing care for chronic headache patients with refractory symptoms.
Methods
Semistructured interviews were conducted with refractory headache patients in Northeast and Central Pennsylvania who had frequent ED visits, frequent abortive medication refills, or were referred to Neurology without adequate medication trials. An interview guide exploring aspects of headache care was developed. Transcripts underwent coding and collaborative review for inductive thematic analysis.
Results
Sixteen interviews of predominantly middle-aged, unemployed or disabled patients with an average of 20 monthly headache days were conducted. Analysis revealed five themes for system-based care: convenience, empowerment, continuity, timeliness, and acceptance.
Convenience: Over 50% reported negative ED experiences due to prior ambulatory care challenges including issues with refills, prior authorizations, and scheduling. Telemedicine and patient portals improved access and reduced burdens. Empowerment: Patients struggled with understanding and managing their condition; 38% expressed fatalism about treatment. Tools like symptom trackers and structured education were valued but underused. Continuity: Social, economic, and logistical barriers hindered follow-up, with 50% citing transportation and financial issues. Limited access to subspecialists led to ED reliance. Timeliness: Delays in care, diagnostic uncertainty, and failed medication trials were common. Nonheadache comorbidities and rigid care algorithms further impeded timely treatment. Acceptance: Stigma, especially in acute settings, discouraged care-seeking, with 50% being perceived as drug-seeking. Positive provider interactions fostered trust and tailored care.
Discussion
Recommendations include emphasizing telemedicine, streamlined prior authorizations, and automated refills to improve access. Structured educational resources, headache tracking tools, and support groups can enhance patient engagement. Regular follow-ups using pharmacist-led medication management can improve therapeutic consistency. Early diagnosis and treatment through modern triage systems can prevent delays and long-term complications. Reducing stigma via personalized care plans and system-wide programs fosters trust within the headache community. These findings offer a framework for quality improvement in headache care across diverse healthcare systems.
This is a visual representation of the abstract.
Introduction
Primary headache disorders, particularly migraine, present a major public health concern in the United States, affecting approximately 18% of women and 6% of men. 1 The 2019 Global Burden of Disease Study placed primary headache conditions as the 14th leading cause of Disability Adjusted Life Years, tenth in females, yet headache is among the most commonly underdiagnosed and undertreated conditions faced by patients.2,3 The healthcare systems that care for headache patients must continue face the challenge of caring for a large population with complex care needs. As such, headache patients constitute 3% of emergency department (ED) visits annually and represent the third leading cause of visits among reproductive age women. 4 This contributes to the economic burden of headache care with migraine patients incurring almost $9000 more in total annual costs compared with healthy controls, compounded by productivity loss leading to an estimated annual worldwide impact of over $19 billion dollars.5,6 The magnitude of this on individuals and systems highlights the need for a unique, patient-centered, quality-focused approach to care.
The Virtual Headache Hospital (VHH) is a quality improvement (QI) project within the Geisinger Health System designed to identify refractory headache patients and triage them to an appropriate level of care for diagnosis and treatment (see Appendix 1 for further details). We defined refractory headache patients as those that had been to the ED for headache twice in 12 months, refilled abortive medications two or more times within a three-month period, or had been referred to Neurology without trying one abortive and one preventative medication. Patients who met these criteria were considered eligible for further triage by the VHH intake team. In the context of this study, “medication refills” pertains to pharmacy-dispensed abortive medications that typically do not require a new prescription each time, as standard practice in the United States allows for multiple refills under a single prescription.
Prior research studies focusing on development and implementation of headache management programs have often targeted providers and health systems to improve delivery of care.7–10 However, success hinges on also understanding the patient's journey and using this information to drive improvements. Chronic headache patients’ experiences with their condition, documented through different qualitative means including surveys, focus groups, narrative reviews, and ethnographies have identified headaches as complex debilitating neurological diseases with impacts on psychological, economic, and social health.11–16 Precedent also exists for the utility of semistructured qualitative interviews with this population to understand their lived experience with an often-disabling condition.17–20. Despite this knowledge, there is a notable lack of literature exploring how the current healthcare system either facilitates or hinders patients’ ability to access adequate care and achieve wellness—particularly from the patients’ own perspective. This project thus aims to utilize semistructured interviews to establish the patient's perspective regarding the improvement of system-based care for chronic headache patients with refractory symptoms.
Methods
Study setting and design
This study was conducted at Geisinger Health System, an integrated healthcare organization serving patients primarily in Central and Northeastern Pennsylvania. It includes a network of hospitals, clinics, a health plan, and a research institute, with a focus on value-based care, innovation, and population health management. We conducted qualitative semistructured interviews of headache patients with subsequent coding and inductive thematic analysis from generated transcripts. Interviews were conducted as a part of the ongoing QI initiative and did not meet the criteria of human subjects research according to Geisinger's institutional review board (IRB) (No. 2023-1490).
Sampling
Our sample population came from refractory headache patients who were eligible to be enrolled in the VHH. A random number generator was used to select candidates for interview from a biweekly updated list with five new selections for potential interview derived each week until information saturation was observed.
Interview guide development
VHH members including patients, pharmacists, clinicians, and QI experts created and iteratively improved the interview guide addressing the topics of interest (Appendix 2). Semistructured interview topics included: experience receiving headache care, barriers to care, examples of poor or ideal care, patient education, symptom tracking, medication management, provider experience, and desired support from health systems. Four pilot interviews were conducted to ascertain face validity, and the interview guide was edited in accordance with each question's success. The finalized interview guide following pilot interviews was used for all subsequent ones.
Data collection, privacy, and processing
Interviews were conducted over a telephone call from a secure phone line. A maximum of three outreach attempts were made for each patient three– to five days apart during working hours, and voicemails with a call back number were left to facilitate scheduling. Sixteen interviews were completed from November 2023 to March 2024. Patients contacted were assigned a study ID accessible only to the study team. We obtained verbal consent from all patients at the time of the interview. All files were stored in a password protected location. Data collection terminated when informational saturation was achieved. 21 Software for data storage and analysis included Microsoft TeamsTM, WordTM, and ExcelTM. Demographic information and headache history data were collected from interviewees themselves and supplemented by the electronic health record (EHR). Interviews were performed by authors JK and PW and manually transcribed by the interviewers themselves. Of note, both interviewers utilized the finalized interview guide for consistency of data collection, however given the semistructured nature of the interview process, the emphasis on each topic was under the discretion of the interviewer themselves and individualized to each patient. Transcripts were deidentified by removing patient-specific identifiers and replacing them with a study ID number.
Data analysis and reliability
Demographic information was analyzed using basic descriptive statistics including averages or medians, depending on data normality, with appropriate measures of variability. Regarding qualitative data, all 16 deidentified transcripts were independently open coded by interviewers (JK and PW) for codebook generation. An iteratively refined codebook was created and reviewed by the study team for precision and validity (Appendix 3). The codebook contained the following categories: experience with providers, system-based challenges to delivering care, patient lived experience with headaches, technology as an interface with the health system, external and internal barriers, medication related experiences, desired or ideal care, self-management strategies, and patient stigmatization. Any mismatched codes arising from the independent coding were reconciled utilizing collaborative team meetings. Inductive thematic analysis was performed utilizing codes and example quotes. 22 Reliability of the above collaborative analysis methodology has been demonstrated elsewhere in the field.5,19,23–26
Data availability statement
The deidentified aggregate summary data file can be made available from the corresponding author on reasonable request.
Results
Demographics
Demographic characteristics of the sample, in comparison with the entire cohort of eligible patients, suggest similarity between those who participated in interviews and those that did not (Table 1). Eligible patients were contacted at least once for consideration of an interview with a total of 86 patients contacted, 16 of which participated in the interviews (18.6%). The average age of interviewed patients was 46.9 (SD: 14.3) and 10 were female (62.5%). The majority of interviewed patients (56.2%) had a documented diagnosis of migraine prior to the interview, consistent with the proportion observed in the total cohort. However, a substantial number of patients in both groups were recorded as having an unspecified headache condition rather than a clearly defined primary headache disorder—18.8% among interviewed patients and 29.1% in the overall cohort. Despite these similarities, the average number of ED visits for our interviewed sample in the year prior to first contact (1.1) was higher than that of the total cohort (0.44). Among the interviewed patients, the primary eligibility criteria for the VHH was being referred to Neurology without first trialing both an abortive and a preventive medication (62.5%, n = 10) in comparison to having two or more ED visits within the past year—observed in 25% of interviewed patients or refilling abortive medications two or more times within a three-month period (12.5%, n = 2).
Demographics and comparison of interviewed patients to the entire cohort of patients sampled for potential interview.
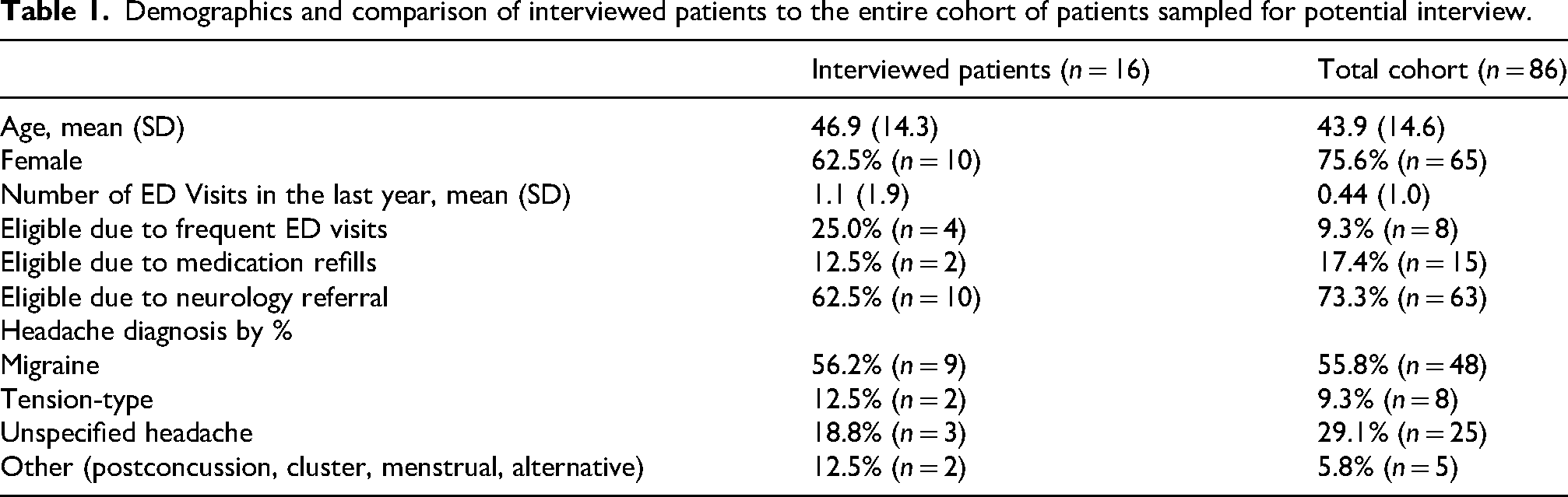
Table 2 examines the characteristics of headache care for the interviewed sample. The average monthly headache frequency in days for our sample ascertained at the time of interview was 20.3. The median duration of time since the last Primary Care, general outpatient Neurology/Headache Specialist, and Emergency Department visit in this population was four weeks (IQR 22.3), 16 weeks (IQR 87.5), and eight weeks (IQR 16.0) respectively. All interviewed patients disclosed that they had been to the emergency department at some point in their illness for acute management of headaches. The average number of lifetime preventative and abortive medications documented for our sample was 2.2 (SD 2.0) and 3.1 (SD 3.9), respectively, ascertained at the time of first contact. With regard to head imaging, 62.5% (n = 10) had received a head CT scan prior to the date of first contact, and 50% (n = 8) had received a brain MRI. Twenty-five percent (n = 4) reported having used alternative medicine specialists such as chiropractors, massage therapists, or acupuncturists, and 43.8% (n = 7) reported being disabled or unemployed at the time of interview.
Characteristics of headache and care received collected for interviewed patients.

Thematic analysis
Through use of our codebook and direct example quotes, we stratified our results into five themes representing five priorities for system-based headache management: convenience, empowerment, continuity, timeliness, and acceptance. Figure 1 lists codebook definitions.
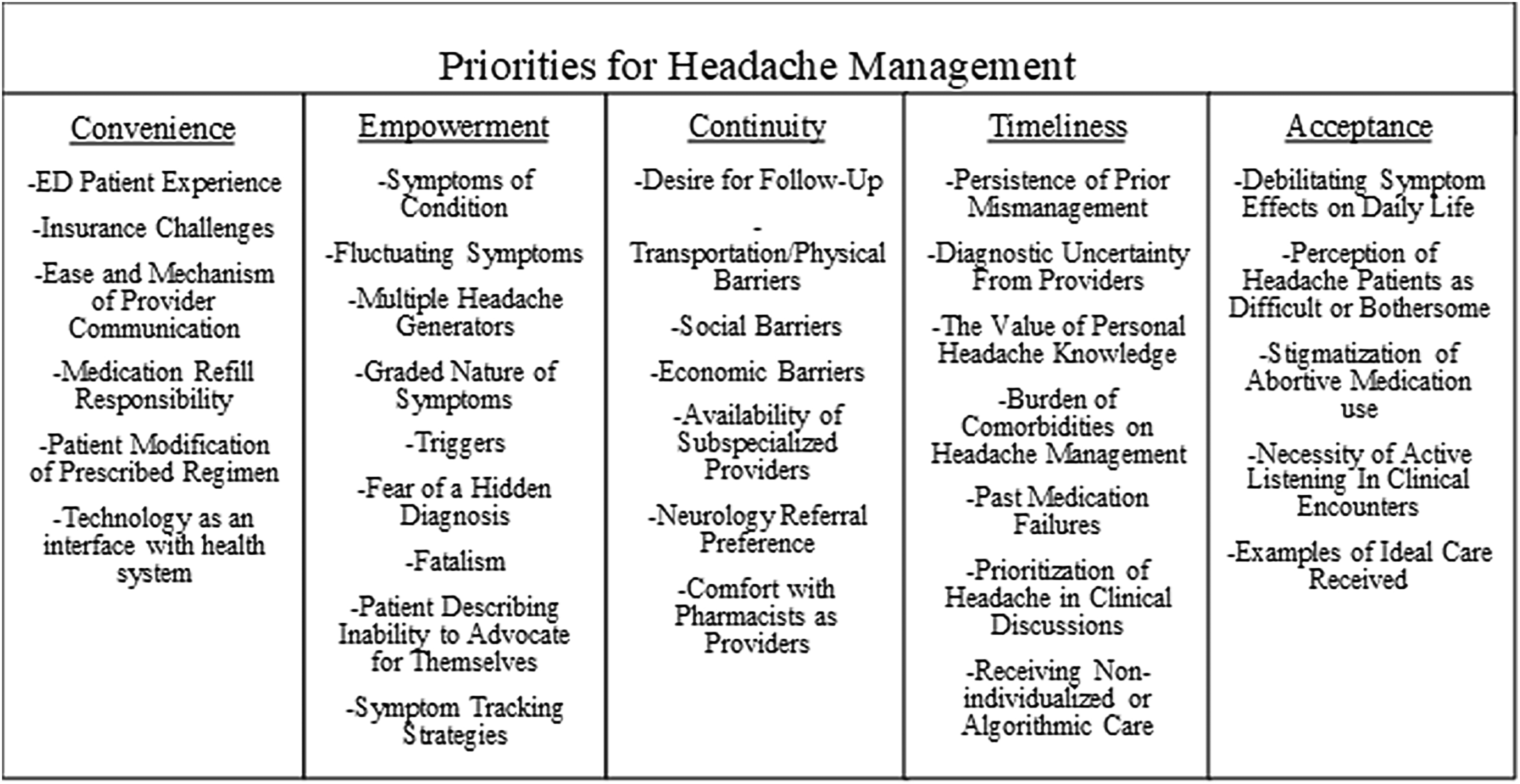
Five themes generated from qualitative codes representing five priorities for headache management.
Convenience
We identified several factors contributing to poor headache control pertaining to the idea of inconvenient care (Table 3). Over 50% of the patients interviewed reported having at least one poor experience while seeking care in the ED; this negative perception was driven by long wait times, unnecessary testing, and inadequate treatment. Patients reported that the decision to seek emergency care was the product of several preceding failures to obtain appropriate care at primary care sites. Over 50% of our sample also reported altering their abortive and prophylactic medications independently for convenience, due to adverse effects or persistent symptoms. This self-titration was reported to be linked to challenging tasks such as regularly requesting medication refills, reminding the office to perform insurance prior-authorizations, finding optimal follow-up appointment dates, and deciphering which services and medications were covered by insurance.
Identified factors relating to the theme of convenience with representative quotes.

Despite these challenges, nearly all patients endorsed the use of technology to perform essential functions such as messaging providers, checking medical records, obtaining postvisit instructions, and scheduling appointments. Geisinger's patient communication portal was widely accepted and utilized by our sample given its ease of use and expanded access capability. All but one of our patients also identified that the most convenient and beneficial visits were those that took place over the phone or through video conferencing. Telemedicine overall was considered highly favorable by our sample of patients.
Empowerment
Another theme that emerged from our discussions was the critical need for patient empowerment (Table 4). Through discussions with our sample, we identified the complexity of the headache conditions themselves as a barrier to care. All patients reported debilitating symptoms that disrupted their ability to function at work and home and interfered with their ability to track symptoms, attend follow-up appointments, and take prescribed medication at predefined intervals or in appropriate amounts, which are necessary steps to achieve control. Discussions also revealed that headache symptoms fluctuated seasonally such that they were powerless to evaluate the efficacy of medications. This left them with the perspective that their headaches were no longer binary all or nothing phenomena, but instead existed along a graded spectrum in severity, frequency, character, and duration with nearly all patients having some degree of symptoms most of the time. Another key factor contributing to this complexity was that over half of our patients reported multiple comorbidities that contribute to their clinical picture as secondary headache etiologies, each with their own set of triggers, making it difficult to ascertain the exact cause of their symptoms at any given time. Examples of comorbid conditions included intracranial aneurysms, Giant cell arteritis, Chiari malformations, Meningiomas, among others. These conditions were reported to confound their clinical picture, disrupting the clear diagnosis of a primary headache disorder alone by introducing secondary headache diagnoses. As such, it became unclear to the diagnosticians involved, and even the patients themselves, whether they have received or should receive a formal diagnosis of a primary headache disorder despite meeting clinical criteria. This is reflected in the large proportion of cohort patients (29.1%) documented as having an unspecified headache disorder upon chart review (Table 1).
Identified factors relating to the theme of empowerment with representative quotes.

Forty-four percent of patients also reported fear of a hidden diagnosis in which the complexity of each patient's condition created a sense that there was a sinister, undiscovered diagnosis causing headaches. Patients described to us how this fear generated distrust in the therapeutic journey and often precipitated the use of unnecessary imaging and specialist consultation at the behest of the patients themselves. In our sample, 38% reported having trouble controlling or understanding their symptoms and disclosed that their headaches were inevitable, with any attempt at symptom control or remission being futile. We described and labeled this phenomenon as fatalism. Compounding the fatalism, patients frequently described being at the periphery of their care, despite being able to contribute the most helpful information given their lived experience with their condition. Seventy-five percent of patients described an inability to advocate for themselves in clinical encounters and a lack of active listening that would have otherwise solved many issues they were facing.
Despite these challenges, our patients highlighted opportunities through which they became empowered to care for their condition. Regarding the complexity of the headache experience, our patients noted positive experiences surrounding symptom tracking and self-education. Two patients detailed the utility of application-based symptom trackers such as Migraine BuddyTM which according to them provided a modern, user-friendly means through which triggers, symptoms, and treatment strategies were tracked. Despite these individual endorsements, 81% of interviewed patients did not track any aspect of their headache condition.
Most of the patients desired education about their headache condition regarding a range of topics including etiology, common triggers, and modern prescription treatment options, with nearly half (44%) of them requesting information about effective lifestyle and over-the-counter remedies. The content of delivered information was identified by our sample as being important, but the means through which it was delivered was as well, with nearly all patients endorsing utilization of online search engines to attempt to find this information independently. Regarding education, two of our patients emphasized the headache community as a resource. Whether through family or friends with headache conditions, patients described the utility of collaborating with fellow members of the headache community to identify helpful providers, learn about treatment options, and find emotional support.
Continuity
The third theme identified pertained to follow-up and continuity (Table 5). Our patients frequently cited discontinuous care as a source of difficulty for them achieving adequate headache control. Social, economic, and transportation barriers were reported to contribute to a lack of consistent follow-up. Fifty percent of patients interviewed described transportation and social responsibilities as barriers to their ability to properly utilize services. Economic barriers identified included difficulty in affording regularly suggested over-the-counter remedies including vitamins and challenges negotiating with insurance for coverage of necessary procedures like Botox. Many (43.8%) of the patients interviewed reported being disabled or unemployed and mentioned that this made affording expensive therapeutics nearly impossible.
Identified factors relating to the theme of continuity with representative quotes.

Another continuity-related challenge faced by our patients was the limited availability of subspecialized headache providers, noted by 44% of our sample. Patients disclosed that busy primary care providers tended to refer in the case of complex headache conditions. On a more practical note, when asked about how comfortable patients were seeing a pharmacist as a regular provider to be evaluated for medication adjustments and to ensure continuity of care, all but two were in favor of this approach.
Timeliness
Patients interviewed frequently identified delays in diagnosis and treatment as significant obstacles to regaining control (Table 6). The first of these pertains to what we called persistence of prior mismanagement, in which the care that was delivered in prior encounters had an impact on the diagnostic and treatment course available for our sample today. For example, one patient revealed that she had not been on preventive medication for 15 years and that delay structured her illness course such that she currently cannot achieve control using modern options. Another example can be found with a patient having seen multiple doctors, all of which kept referring her to others, until eventually her healthcare course was too complicated for anyone to understand.
Identified factors relating to the theme of timeliness with representative quotes.

Similarly to how the complexity of any individual's headache course can become overwhelming to each patient, clinicians were also tasked with deciphering this web of information for diagnosis and treatment. One critical pattern identified among this sample of patients was diagnostic uncertainty, noted in 50% of our sample. Whether this is through miscommunication with providers or breakdown of the diagnostic process, many of our patients were unclear about the exact cause of their headache symptoms. Related to this, one frequently cited concern that our sample of patients endorsed was not being taken seriously enough as experts in their illness history, with many describing years of personal experience as a valuable resource for clinicians that was not the focal point of the diagnostic process. This individualized knowledge represented a major untapped resource for guiding appropriate and timely treatments.
Moving further into the treatment side, 25% of the patients we interviewed possessed nonheadache-related medical comorbidities that clouded the picture of each patient's history and limited the use of certain medications, contributing to a lack of timely therapy initiation. Additionally, many of the patients interviewed described a long history of failed medications, again further limiting the ability of each clinician to make an impact given the momentum of previous encounters. This led to 50% of sampled patients reporting having received algorithmic or nonindividualized care, especially in acute situations.
Acceptance
Our sample described experiencing the perception that they were difficult or bothersome (Table 7). Three patients felt as though their concerns were a nuisance, rather than a legitimate complaint which prohibited them from seeking care. Although the intention of the interviews was not to elicit details pertaining to the systematic stigmatization of headache patients, it became a frequent topic of conversation among patients that identified their position as a marginalized community in healthcare. This stigmatization became especially noticeable when discussing treatment of acute breakthrough symptoms in which 50% of patients felt as though they were being perceived as drug seeking in emergency settings.
Identified factors relating to the theme of acceptance with representative quotes.
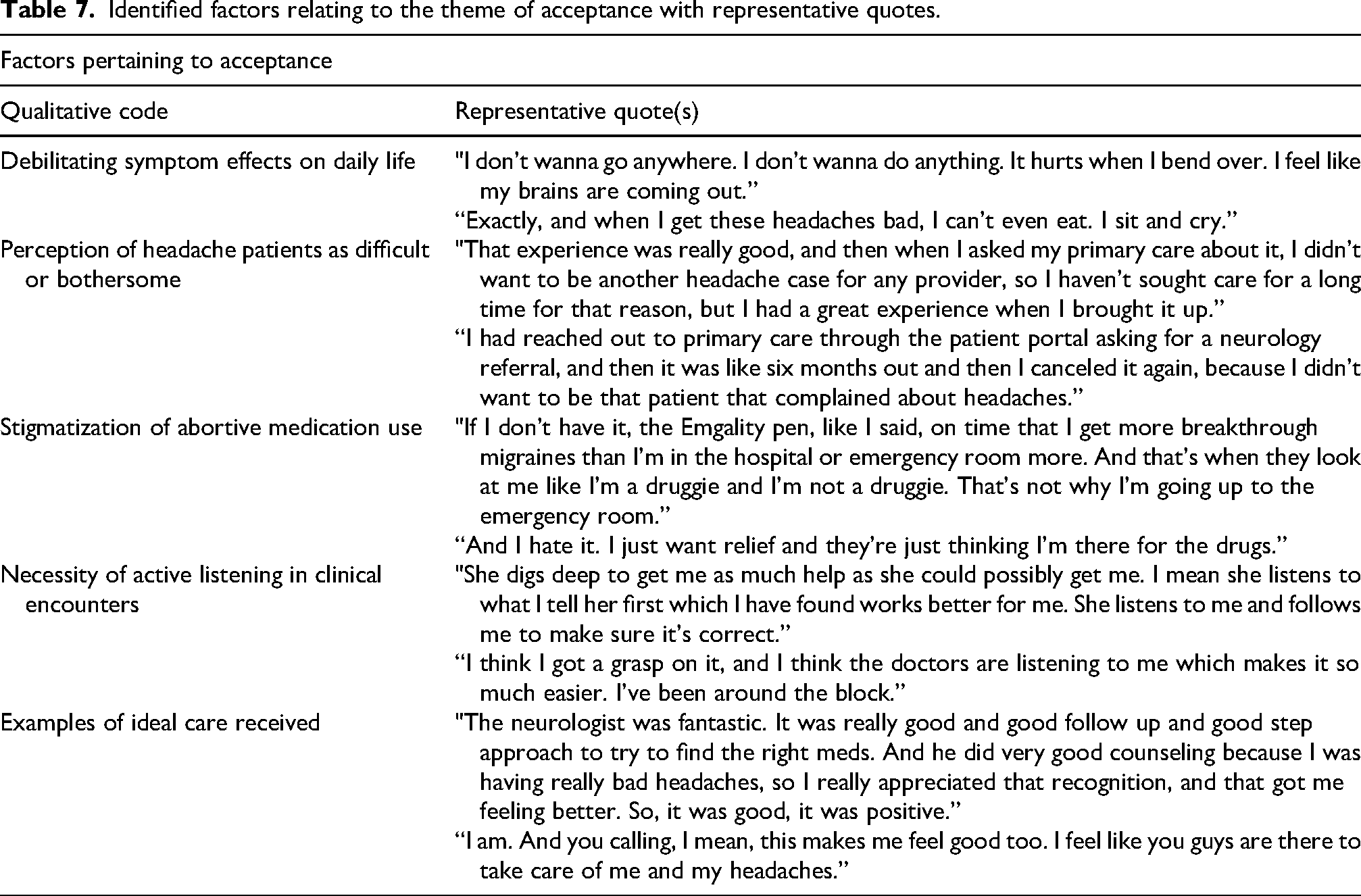
The few positive interactions reported by our sample highlighted providers who acknowledged the significant disabilities faced by this population. These providers actively listened to their patients, tailoring care to address each person's unique challenges. Beyond the positive impact of specific providers, our sample appreciated when our system made an active effort to recognize their struggles. As a succinct example of this, one patient described that simply reaching out to her made an impact and that calling her made her feel cared-for and recognized.
Discussion
We conducted interviews with patients that have refractory headaches within the Geisinger System in Northeast and Central Pennsylvania, and through inductive analysis, identified five key themes that highlight priority areas for system-level management of this distinct population. Each of the above headache QI priorities provides a theoretical framework through which specific, incremental changes can be derived to improve outcomes for any health system. From our discussions, in concert with already published literature, we have identified many practical suggestions that fall within each of the listed priorities above.
Convenience
Headache patients that are challenged with debilitating symptoms and complex socioeconomic barriers rely on convenient healthcare options. It was deduced that the ED, despite being frequently used, is ill-suited to caring for this population because of its structure as a high-throughput acute care facility. Our interviews have revealed multiple opportunities to enhance the convenience of outpatient headache management and avoid overutilization of emergency services. Firstly, telemedicine is a crucial access point including video or phone call follow-up visits, specialist e-consults, provider messaging forums, testing result communication, and educational material delivery. The utilization of telemedicine has been demonstrated to be an effective intervention for improving headache care, a concept supported by our interview patients.28–30 Secondly, based on our discussions, system level efforts to streamline prior authorizations, and facilitating automated refills, when appropriate, would ensure continuity of patient care and reduce periods of potential treatment lags. Insurance authorization, in particular, among our sample and others, was a major barrier to adequate patient care. 27 System-level initiatives to streamline and expedite prior authorizations for all medications are currently underway at Geisinger.
Empowerment
Given the complexity of each patient's headache experience and the shortage of subspecialized headache providers, patients are required to be an active member of their care team and a champion of their wellness. 31 Through our discussions, we learned that many of our patients approached their headache condition through a fatalistic lens, viewing their symptoms as inevitable, creating a psychological barrier toward participation. One mechanism to empower such patients is the provision of structured, accurate, multimodal, education-level appropriate resources to understand their condition. While provision of these educational resources has been validated to improve care already in the literature, we have uncovered the topics most important to patients including lifestyle modifications, natural remedies, current understandings of headache generators, typical triggers, and routine updates regarding new therapeutics such as increasingly popular CGRP antagonists. 32
Furthermore, while patients expressed a desire to track their symptoms, they paradoxically did not follow through. Our discussions suggest several possible explanations for this, including the use of cumbersome tracking methods, a perceived futility in monitoring symptoms that are frequent and stereotyped, and an extension of the fatalism described above—where the overwhelming burden of symptoms discourages engagement in self-monitoring. In addition to educational material, recommendation of validated headache tracking tools, usually in the form of smartphone applications or wearable devices, has the capacity to heighten the ability of each patient to understand the nuances of their idiosyncratic headache experience. 33 However, the reasons for a lack of symptom tracking is nuanced and requires individualized discussion with each patient. Finally, an additional empowerment mechanism is encouragement of collaboration with the headache community such as support groups, a strategy identified in previous studies. 34 Based on our discussions, these groups should focus on collaborative efforts to share prevention strategies, experiences with medications, and accessible updates on research. Most importantly, they should foster a sense of community and mutual support.
Continuity
Among our sample, one frequently cited concern was inconsistency of follow-up to guide changes in therapeutic regimens. The patients interviewed voiced unmet needs regarding ED follow-up and reliable communication with providers for continued management. These results are consistent with prior research showing that patients with migraine face challenges related to seeing the appropriate provider, receiving a diagnosis, and initiating treatment with less than 5% of patients meeting these goals in succession. 3 Despite an expanding range of treatment options, about 40% of patients with episodic migraine report having one or more unmet needs in their treatment leading to overutilization of emergency services, reliance on opioids, dissatisfaction with treatment efficacy or safety, or persistent disability. 35 According to our patients, there exists an increasing need for consistent care which cannot be met currently with traditional care structures that emphasize infrequent and brief ambulatory visits.
Through our discussions, we also ascertained that subspecialized headache Neurologist appointments were scarce, another contributor to the incongruence between supply and demand of specialty care related to a nearly universal preference toward referral to Neurology. 7 A predilection toward referral, combined with a scarcity of subspecialized providers, often creates a triage bottleneck such that patients are left searching for an appropriate care avenue, only to arrive periodically in the ED out of necessity. 7
One potential solution to this dilemma, which has received near-unanimous support from our sample, is to utilize pharmacists trained in headache management as regular points of contact. Medication Disease Therapy Management pharmacists are already effectively used in the Geisinger system, and beyond, for managing chronic conditions such as diabetes or chronic pain by providing regular, frequent visits for evaluation of medication efficacy and adverse effects. 36 Application of this model to headache medicine has already taken place within health systems, creating many contact points for this population and allowing for regular medication adjustment and breakthrough reduction. Additionally, incorporating expert pharmacists trained in headache medicine into primary care settings can help guide appropriate referrals to Neurology, ensuring that patients are effectively triaged and managed based on the severity and complexity of their headaches.
Timeliness
Every interviewed patient described challenges, including perceived delays and complexities in care that misaligned with their treatment goals, that ultimately yielded frustration with their healthcare journey. Each patient emphasized the necessity of early diagnosis and treatment. Our patients reported challenges such as delayed or unclear diagnoses, difficulties in initiating preventive treatments, and early specialist referrals that may not have fully addressed their needs and therefore provided opportunities for improvement. This is a phenomenon previously identified in other population-based studies.3,7,11,20,27,37 Our discussions have identified further from the perspective of patients that the effect of previous misalignment in care compounds over time. Delayed or incorrect diagnosis at the onset often leads to ongoing complications, even years later. 38 Therefore, each episode of untimeliness does not necessarily represent an independent, singular event, but instead represents a deterministic path toward continued issues. 38 Ultimately, these paths are known to be detrimental to patient well-being with these patients having a consistently diminished health-related quality of life. 38 Practically overcoming delays in diagnosis and treatment is a complex issue requiring at least a modern triage system capable of automatically identifying refractory headache patients by their status as overutilizers of abortive medication and/or emergency services as a first step toward improved care. 39 The nearly uniform experience among our participants—marked by an accumulating burden of disease over time—contributes to a cycle of chronic illness that is psychologically difficult to break. Nevertheless, system-sponsored support groups present a valuable opportunity to foster adaptive coping strategies and promote a forward-looking focus on wellness.
Acceptance
Stigmatization of patients with chronic headache disorders is a well-documented phenomenon that has direct implications for clinical outcomes. 40 Semistructured interviews of patients with migraine reveal that the condition negatively impacts emotional and psychological health, cognitive function, and work productivity, all exacerbated by the effect of stigmatization leading to frustration, hopelessness, and isolation.18,41 Our discussions expand these findings by providing patient perspectives regarding the perception that they are difficult, bothersome, or drug seeking in healthcare settings. These patients, often with underlying psychological comorbidities, frequently face the perception that they are inappropriately seeking pain medication for secondary gain. 17 Patients during our discussions disclosed hesitancy about seeking care for fear of being perceived in this way. Alternatively, the most positive experiences noted were those of providers employing active listening toward their experience with a chronic neurological condition.
Beyond the empathic ability of each practitioner, caring for patients with chronic headaches requires system-wide programs tailored to the unique needs of headache patients to create a culture of acceptance. Firstly, integrating personalized abortive medication action plans directly into the EHR—similar to those used for epilepsy management by some systems—would streamline the process for emergency providers, eliminating the need for patients to advocate for themselves to receive effective acute medications. 42 Additionally, a suggestion gleaned from our discussions would be for providers to negotiate with health-system-based insurance plans for streamlined prior-authorization processes and more flexible approval criteria for effective modern treatments to demonstrate to patients that their care systems are prioritizing their interests. Initiatives such as the VHH and the centralized pharmacy services within Geisinger are being developed with the intent to bridge these gaps and facilitate quality care for our patients.
Strengths and limitations
This project possessed several strengths. Firstly, given the nature of the VHH QI initiative, we sampled headache patients that have difficulty navigating the healthcare system to achieve control, fostering the generation of data directly from patients most affected by system-level changes to care. Secondly, the rich nature of qualitative interviews provided a window into the lived experience of these patients wherein we ascertained system-level opportunities for improvement. Lastly, incorporating these findings into broader QI efforts enabled practical, stakeholder-informed suggestions for change.
However, there are limitations. Firstly, our sampled population consisting of undermanaged and refractory headache patients may represent the extremes of the headache community and thereby may not be representative of the overall headache patient population. Additionally, there may be some degree of participation bias. Despite this, those most affected may provide critical insights for improvement. Also, as with any qualitative investigation, the interpretation of the obtained data is subjective, however this effect was minimized through collaborative, iterative, systematic, expert-driven discussion to guide generation of the interpretations above.
Future directions
The five principles of system-based headache management outlined above can serve as a framework for deriving practical changes that can be made to any system attempting to improve care for their population of headache patients. Given the similar challenges faced by all systems caring for patients with chronic headaches, application of these principles to improvement projects in many contexts has the potential to yield meaningful results on healthcare utilization. Furthermore, the success of our discussions themselves validates the use of interview methodology for improvement purposes such that other systems with unique headache populations can engage their communities to uncover idiosyncrasies. Following initiation, the effectiveness of each of these interventions should be validated through iterative QI methodologies tracking quantitative outcomes.
Conclusions
Using semistructured interviews with refractory headache patients within the Geisinger system, we have uncovered a system of factors contributing to either poor or successful headache management. We have identified five priorities for guiding decision-makers within our QI initiative with applicability to every health system facing similar challenges. These priorities of convenience, empowerment, continuity, timeliness, and acceptance have generated patient-derived recommendations for improved outcomes for refractory headache patients. These include automated care process for medication approval and delivery, patient-specific acute care plans for emergency settings, utilization of telemedicine and pharmacist-based follow-up for improved access, and resource provision including multimodal education, modern tracking tools, and creation of headache support group material for collaboration and empowerment. Perhaps most importantly, we have demonstrated that the patient perspective is a valuable resource for any system attempting to improve outcomes for their population of refractory headache patients.
Clinical implications
Patients’ priorities for system improvement centered around five themes—
Barriers included inconvenient and delayed care, self-management struggles, fragmented follow-up, stigma in medical settings, and fatalism about treatment outcomes; telemedicine and structured education emerged as favored solutions.
Proposed improvements included expanding telehealth, providing easy-to-use educational resources and symptom tracking tools, integrating pharmacists into headache care, enhancing early diagnosis, and creating system-level supports for patient advocacy and acceptance.
Strengths included capturing insights from highly affected patients and integrating them into QI efforts; limitations included potential sample bias; the five principles were suggested as a broadly applicable framework for future system-level interventions.
Supplemental Material
sj-docx-1-rep-10.1177_25158163251378644 - Supplemental material for Five priorities for headache quality improvement: Lessons from qualitative interviews of patients in Geisinger's virtual headache hospital
Supplemental material, sj-docx-1-rep-10.1177_25158163251378644 for Five priorities for headache quality improvement: Lessons from qualitative interviews of patients in Geisinger's virtual headache hospital by Justin Kosman, Payton Whary, Peyton Latorre, Scott Friedenberg and Apoorva M. Pradhan in Cephalalgia Reports
Footnotes
Acknowledgments
We would like to acknowledge and thank the entire VHH team staff and the Geisinger Health System for their collaboration on this project.
Consent to participate
Under Geisinger IRB decision No. 2023-1490, this project met criteria for QI and therefore the requirement of written consent was waved as no identifiable personal data were presented.
Consent for publishing
All authors provide consent to publishing.
Author contributions
Justin Kosman: interviewer, project designer, data analyst, manuscript author, and editor; Payton Whary: interviewer, data analyst, manuscript author, and editor; Peyton Latorre: project manager, data analyst, and editor; Scott Friedenberg: principle investigator, project designer, and editor; and Apoorva Pradhan: project designer, data analyst, manuscript author, and editor.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was completed through funding from Geisinger Health Plan Inc. The funder was not involved in the study or the decision to submit for publication.
Data availability statement
Justin Kosman had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.