
Abstract
Objective
Survey Latin American (LATAM) neurologists on their comfort with prescribing triptans in the setting of common contraindications.
Background
Triptans are associated with multiple contraindications due to 5-HT1B-mediated vasoconstriction. A previous survey study examined the comfort level of headache specialists from the American Headache Society (AHS) in prescribing triptans in the setting of various contraindications, but this has not been studied in LATAM countries.
Methods
We sent a modified and translated survey to LATAM neurologists with headache management expertise grouped in the Latin American Headache Association (ASOLAC). The survey was extended to local Neurology Associations to increase the sample. An eleventh question on selective serotonin reuptake inhibitors (SSRI) use was added to the original 10 questions. Responses were assessed with descriptive statistics.
Results
There were 225 surveys analyzed from 10 LATAM countries. Notable results include that 54.2% (122/225) never use triptans in the setting of stroke, 60.9% (137/225) said never for dissection, and 70.2% (158/225) said never for reversible cerebral vasoconstriction syndrome (RCVS), but for venous thromboembolism responses were sometimes in 26.7% (60/225), rarely in 20.9% (47/225), and never in 31.6% (71/225). 57.8% (130/225) responded never for hemiplegic migraine but prolonged aura responses were 25.3% (57/225) sometimes, 25.3% (58/225) rarely, and 40.4% (91/225) never. Responses for use with aneurysms included 23.6% (53/225) sometimes, 15.6% (25/225) rarely, and 44.0% (99/225) never. For poorly controlled hypertension, 58.2% (131/225) said never. For pregnancy, 57.3% (129/225) reported never. Responses for age over 65 years included 35.6% (80/225) sometimes, 32.0% (72/225) rarely, and 22.2% (50/225) never. For SSRI use, responses were 22.7% (51/225) frequently, 38.7% (87/225) sometimes, and 24.0% (54/225) rarely.
Conclusion
Triptan contraindications were often considered absolute for RCVS, stroke, dissection, hemiplegic migraine, hypertension, and pregnancy. More studies are needed to clarify the true danger of triptan contraindications.
This is a visual representation of the abstract.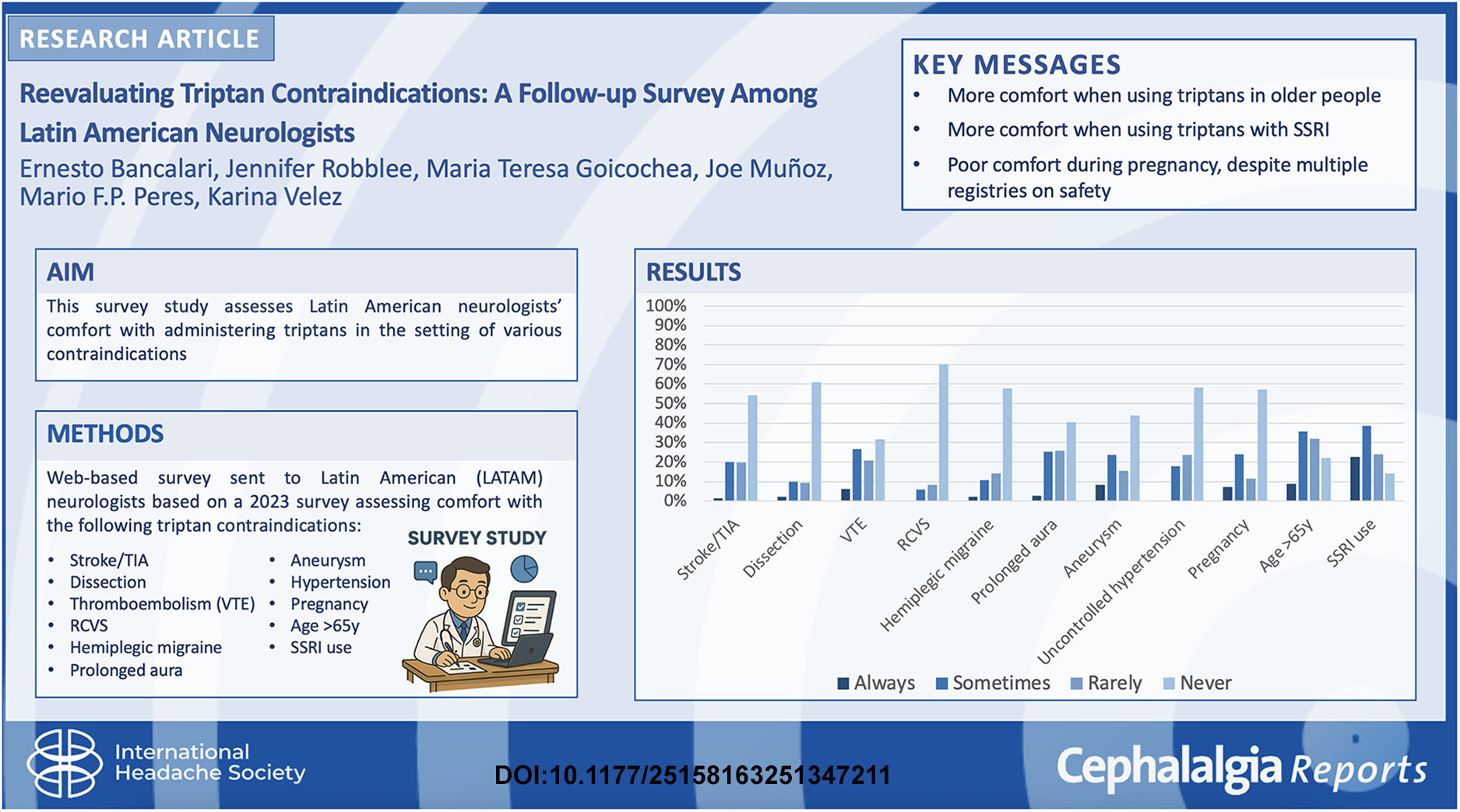
Introduction
Triptans are 5-HT1B/1D agonists used in the acute treatment of migraine; however, there is 5-HT1B-mediated vasoconstriction that has led to several contraindications. Sumatriptan has multiple contraindications on its US Food and Drug Administration approved labeling including coronary artery disease, stroke, hemiplegic migraine, and uncontrolled hypertension. 1 Other situations in which triptan use leads to uncertainty are pregnancy, older patients, venous thromboembolism (VTE), dissection, hemiplegic migraine, and prolonged migraine aura.
Robblee published a survey study in 2023 that assessed American Headache Society (AHS) headache specialist comfort with prescribing triptans in the setting of these various contraindications. 2 The study found that clinicians were often uncomfortable with triptans in the setting of stroke, reversible cerebral vasoconstriction syndrome (RCVS), uncontrolled hypertension and pregnancy, but many clinicians were comfortable prescribing triptans despite age greater than 65 years. Despite pregnancy not being a true contraindication to triptans use based on several registries 3 ; 33.8% of AHS specialists reported that they “never” prescribe triptans during pregnancy.
Global practices vary, and comfort prescribing triptans in the setting of contraindications has not been studied in a Latin American (LATAM) Neurologists/Health care providers. A 2022 study by Lisicki et al. found that 64% (55/86) of clinicians focused on headache medicine reported the absence of headache training programs in their countries, 4 which limits access to headache-specific education. Furthermore, triptan availability and use vary globally. 5 For instance, LATAM countries mainly have access to sumatriptan, naratriptan, and eletriptan, but in Brazil, zolmitriptan and rizatriptan are available. The 2023 survey neglected to assess comfort prescribing triptans to patients on a selective serotonin reuptake inhibitor (SSRI) in light of the black box warning, 6 which AHS has advocated against. 7 Since the late 90's when triptans were launched in LATAM, prescriptions have increased, so we want to understand the common prescription practice of LATAM neurologists in those patients who have triptan contraindications.
This survey study assesses LATAM neurologists comfort with administering triptans in the setting of various contraindications using a modified version of the Robblee 2023 survey. 2
Methods
An anonymous survey based on a previous publication 2 was sent online via SurveyMonkey to LATAM neurologists with expertise in headache management grouped under the Latin American Headache Association (ASOLAC). By completing the survey, respondents provided consent for their data to be used in this publication.
The 2023 survey 2 contained 10 questions that addressed the use of triptans for patients with stroke or transient ischemic attack (TIA), arterial dissection, VTE, RCVS, hemiplegic migraine, prolonged aura lasting more than 24 h, cerebral aneurysm, poorly controlled hypertension, pregnancy, and age greater than 65 years. One question was added to the original questionnaire regarding triptan prescriptions in patients receiving SSRIs: “Do you administer triptans in patients receiving SSRIs?”. In the 2023 survey, each question had six answers on a Likert scale: always, frequently, sometimes, rarely, never and not applicable, but the “Always” response was never used. 2 For this survey, Always and frequently were combined into the Spanish term siempre. Not applicable was translated to mean “have not seen those patients” (“No he visto estos pacientes”). The survey was translated by one of the authors (EMB) for distribution in LATAM countries. See Supplement 1 for the Spanish translation.
The target population was neurologists interested in headache management from LATAM countries. In LATAM there is no formal Headache Specialist certification, so most members gain expertise through International Headache Society (IHS), United States, and/or European Headache Congresses and meetings or through the Headache Masterclass IHS diploma. Some neurologists have trained abroad through fellowships or internships in Europe or the United States. ASOLAC has 147 active members and was used as convenience sampling. To increase the sample size, the survey was expanded to local Neurology Associations, but this left the final number of neurologists contacted as unclear. If more than 50% of the questions were answered with “have not seen those patients,” the survey was excluded. The survey was sent 19 November 2023. Final surveys were received 25 November 2023.
The survey was anonymous, but SurveyMonkey does internally collect IP addresses to prevent repeat responders. The questions are not randomized, and responses could be changed up until the survey was submitted. The Institutional Review Board at St Joseph's Medical Health Center in Phoenix, Arizona gave approval for non-research determination (PHXNR24-500-013-00-10).
The primary analysis was descriptive statistics. Percentages for each response were entered into an Excel spreadsheet. The responses from the original 2023 survey were also compared to the current survey results. Responses between the two surveys that had an absolute difference of 20% were highlighted as clinically relevant.
Results
We received 234 responses from 10 LATAM countries including 50 from Argentina (21.4%), 6 from Bolivia (2.6%), 52 from Brazil (22.2%), 14 from Chile (6.0%), 19 from Colombia (8.1%), 13 from Dominican Republic (5.6%), 2 from Ecuador (0.9%), 37 from Mexico (15.8%), 24 from Paraguay (10.3%), and 17 from Peru (7.3%). Of the 234 responses, nine were excluded due to more than 50% of responses being not applicable (3 from Argentina, 1 from Brazil, 1 from Colombia, 2 from Mexico, and 2 from Paraguay). 225 surveys were left for analysis. It is unclear how many neurologists were contacted once the survey was expanded to local Neurology Associations, so the survey response rate is unclear. There was no missing data as the completeness rate was 100%.
When asked how often respondents administer triptans in a patient with a past medical history of a stroke or TIA, 19.6% (44/225) answered rarely and 54.2% (122/225) never When asked about triptan use in the context of a carotid or vertebral dissection, 60.9% (137/225) never. In patients with VTE on anticoagulation, responders reported using triptans sometimes in 26.7% (60/225), rarely in 20.9% (47/225), or never in 31.6% (71/225). In the context of RCVS, the vast majority 70.2% (158/225) reported never using triptans.
For hemiplegic migraine, 2.2% (5/225) of responders reported that they frequently use triptans, 10.7% (24/225) reported sometimes, 14.2% (32/225) reported rarely, and 57.8% (130/225) reported never. For prolonged aura around 50% of respondents reported that they frequently or sometimes used triptans.
In the context of a treated or untreated cerebral aneurysm, 8.4% (19/225) reported frequently using triptans while 23.6% (53/225) reported sometimes, 15.6% (25/225) reported rarely, and 44.0% (99/225) reported never. With poorly controlled hypertension, none of the responders use triptans frequently, but 17.8% (40/225) reported sometimes, 23.6% (53/225) reported rarely, and a majority of them reported never 58.2% (131/225). During pregnancy, 57.3% (129/225) reported never prescribed a triptan. With age over 65 years, 8.9% (20/225) of responders frequently use triptans, 35.6% (80/225) sometimes, 32.0% (72/225) rarely, 22.2% (50/225) never, and 1.3% (3/225) not applicable. In the context of a patient on an SSRI, 22.7% (51/225) reported frequently using triptans, 38.7% (87/225) sometimes, 24.0% (54/225) rarely, and 14.2% (32/225) never. See Table 1.
Responses to the 11 questions.

N/A: not applicable; RCVS: reversible cerebral vasoconstriction syndrome; SSRI: selective serotonin reuptake inhibitor; TIA: transient ischemic attack; VTE: venous thromboembolism; y: years.
Using an arbitrary 20% differences as relevant, several questions had larger percentage differences between answers across these survey results and those from 2023, usually at the extremes of the Likert scale. When responding to comfort using triptans in the context of a carotid or vertebral dissection, 60.9% of LATAM respondents would never use a triptan while a lower percent, 29.7%, of AHS respondents would never use a triptan with a dissection. On the VTE question, triptan use was reported as frequently for 30.6% of AHS respondents compared to only 6.2% LATAM respondents. Triptan use for hemiplegic migraine was never for 57.8% of LATAM respondents compared to 29.9% of AHS respondents. For prolonged aura, aneurysm, and older age, both extremes of the Likert scale were notable. In prolonged aura, frequently was the response for 24.3% of AHS respondents versus 2.7% of LATAM respondents while never was reported by 40.4% of LATAM versus 14.9% of AHS respondents. Triptan use was reported as frequently for aneurysms in 30.4% of AHS respondents compared to only 8.4% of LATAM with 44.0% of LATAM reporting never compared to 21.6% of AHS respondents. Triptan use in patients of older age was reported as frequently in only 8.9% of LATAM respondents compared to 45.3% of AHS respondents with the response of rarely for 32% of LATAM respondents versus 6.1% of AHS respondents. See table 2 for comparison to the 2023 survey results.
Comparison between percent response rates for the United States and LATAM countries with absolute differences of 20% of more highlighted.

LATAM: Latin America; N/A: not applicable; SSRI: Selective Serotonin Reuptake Inhibitors; USA: United States of America.
Discussion
Triptan contraindications were considered absolute by LATAM respondents for especially patients with RCVS, but over 50% of respondents also considered stroke/TIA, dissection, hemiplegic migraine, uncontrolled hypertension, and pregnancy as an absolute contraindication. These categories are similar to those reported by Robblee, where stroke, RCVS, hypertension, and pregnancy also had high rates (30–60%) of being considered absolute contraindications. 2 As discussed in that paper, pregnancy in particular is no longer considered a contraindication to triptan use after extensive study in pregnancy registries. 2 Age and SSRI use were the two questions with the lowest rate of being considered an absolute contraindication in this survey. Unlike the 2023 survey, none of the questions had response rates of “never” less than 10%.
When comparing this survey's responses in a LATAM population to the 2023 AHS survey results, some patterns were noticed. In all cases, if a percentage was higher in one of the two surveys, the AHS survey respondents were more comfortable with use of triptan in these contexts than the LATAM population. When comparing responses for frequently, there was an absolute difference of 20% or more for VTE, prolonged aura, aneurysm, and age greater than 65 years. When comparing responses for never, there was an absolute difference of 20% or more for dissection, aneurysm, hemiplegic migraine, prolonged aura, and pregnancy. Overall, this suggests that members of the AHS, many of whom are headache specialists, are more comfortable using triptans in complicated nuanced situations like these relative contraindications. A unique limitation and potential bias affecting the lower confidence in prescribing triptans in LATAM is that triptans are available without a prescription. Consequently, even if an initial triptan prescription is given, the prescriber cannot monitor ongoing self-medication use.
The strength of this study is that it expands upon a previous survey by assessing a LATAM population for a broader viewpoint. Furthermore, it added an additional controversial situation of SSRI use with triptans. The limitations include that the response rate is unclear but there was a high number of responders across 10 countries. Important to mention is that there is no formal assessment of the level of expertise nor experience in headaches of the respondents due to the fact there is no sub specialty license as such in LATAM. Similar to the limitations in the 2023 study, the questions were limited to multiple choice which prevents nuanced answers. Also to point out that there is no difference made between “contra-indication” in the acute or subacute stage, or even a situation where the problem has resolved completely. Regardless this study shows that triptans are underused in LATAM countries, perhaps even more than was seen by AHS members. Many of these complicated situations are treated as absolute rather than relative contraindications.
Conclusion
Triptan contraindications were considered absolute by LATAM respondents for especially patients with RCVS, stroke/TIA, dissection, hemiplegic migraine, uncontrolled hypertension, and pregnancy. Respondents were most comfortable using triptans in the context of older age and SSRI use. When compared to AHS membership, there was a pattern of lower rates of triptan use in these various situations. More studies are needed to clarify triptan contraindications, and more education to both general neurologists and headache specialists worldwide is needed on safety of triptans in contexts like pregnancy.
Clinical implications
Triptan contraindications were considered absolute for LATAM respondents RCVS, stroke/TIA, dissection, hemiplegic migraine, uncontrolled hypertension, and pregnancy.
Respondents were most comfortable using triptans in the context of older age
Respondents were most comfortable using triptans in association with SSRI antidepressants.
When compared LATAM to AHS survey data, there was a pattern of lower rates of triptan use in these various situations.
More studies are needed to clarify triptan contraindications
Education to both general neurologists and headache specialists worldwide is needed on safety of triptans in contexts like pregnancy.
Supplemental Material
sj-docx-1-rep-10.1177_25158163251347211 - Supplemental material for Reevaluating triptan contraindications: A follow-up survey among Latin American neurologists
Supplemental material, sj-docx-1-rep-10.1177_25158163251347211 for Reevaluating triptan contraindications: A follow-up survey among Latin American neurologists by Ernesto Bancalari, Jennifer Robblee, Maria Teresa Goicochea, Joe Muñoz, Mario F.P. Peres and Karina Velez in Cephalalgia Reports
Footnotes
Acknowledgments
Not applicable.
Disclosures
Dr Bancalari discloses serving on a medical advisory board for Pfizer as well as serving as the R&D Director for GSK 1999–2016 and the Medical Director for Abbott 1998–1999. Dr Robblee discloses grant support from Barrow Neurological Foundation, investigator support from Eli Lilly and AbbVie, Medical advisory board for Abbvie and Tonix, and a paid editorial relationship with MedLink Neurology and Neurodiem. Dr Robblee also discloses that a family member has partial ownership of Scottsdale Providence Recovery Center. Dr Goicochea discloses serving on a medical advisory board and as a speaker for TEVA, Abbvie, and Pfizer. Dr Muñoz discloses serving as a speaker and medical advisor for Pfizer Latin América. Dr Peres discloses serving on a medical advisory board for Teva, Abbvie, Pfizer, Lundbeck, and Eurofarma. Dr Velez discloses serving as a speaker and on advisory boards for Abbott, Allergan AbbVie, Carnot, and Pfizer. FINANCIAL SUPPORT: None provided for development of this manuscript.
Author contributions
Dr Robblee and Dr Bancalari had the concept and wrote the initial draft. All authors participated in the rest of the roles.
Informed consent
By completing the survey, respondents provided consent for their data to be used in this publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Yes.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.