
Abstract
Background
Interictal burden impacts the quality of life of migraine patients especially the fear of the next attack. However, it is unclear which variables influence the fear of the development of a future migraine attack. Therefore, the aim of this study was to identify factors contributing to the fear of attacks in patients with episodic migraine and to investigate the differences between individuals with low and high attack anxiety.
Methods
Potential factors affecting fear of attacks were assessed by using the Headache Impact Test, Central Sensitization Inventory, Allodynia Symptom Checklist and the Neck Disability Index. Fear of attacks was quantified using Fear of Attacks in Migraine questionnaire. A multiple linear regression was used to evaluate which of these factors would explain the dependent variable fear of attacks.
Results
The included sample of patients with episodic migraine (n = 46) had a mean of 79.4 (21.2) points on the Fear of Attacks in Migraine Inventory questionnaire and according to its subscales; attention and anticipation had the highest score of 37.8 (9.3) points. Headache impact and allodynia symptoms explained 35.2% of the results of the fear of attacks questionnaire in episodic migraine (p < 0.001). High attack anxiety individuals had higher scores regarding headache impact, central sensitization, allodynia symptoms and neck disability, compared with low attack anxiety.
Conclusion
Allodynia and headache impact are major factors affecting the fear of attacks and might subsequently be addressed in the management the interictal burden of episodic migraine.
This is a visual representation of the abstract.
Keywords
Introduction
Migraine is a neurological condition characterized by alternating ictal and interictal phases.1,2 Migraine is recognized as a leading cause of disability worldwide, impairing quality of life, disrupting social interactions with family and friends, 3 causing absenteeism at work and contributing to the economic burden through increased direct and indirect costs.4,5
During a migraine attack, the condition is characterized by sensitivity to light, noise, smell, 1 signs of allodynia 6 and central sensitization, 7 and even physical impairments such as cervical dysfunction and disability. 8 However, evidence from the literature demonstrates that the impact of migraine extends beyond the acute attacks, significantly affecting individuals even during interictal periods, which are typically expected to be pain-free, when the anticipation and fear of the next attack are particularly notable.9,10
The burden associated with the fear of attacks is linked to anxiety and avoidance behaviours. This includes feelings of being unable to plan, perceiving oneself as unreliable regarding scheduled activities and social interactions, the need for adaptations to daily routines, lifestyle changes, reducing or ceasing work, avoiding social or family activities, and experiencing anticipatory anxiety about the next migraine attack, 9 which may lead to different forms of stigma. 11
Many qualitative studies9,12,13 have demonstrated that the interictal burden can be as disabling as the ictal one. A global survey 14 across individuals with migraine diagnosis and a monthly frequency of migraine attacks ≥4 showed that fear of the next attack was among the negative aspects of living with migraine in 55% of the respondents. 14 In a Delphi study including patients with migraine as experts, fear of attacks was included as an outcome measure considered meaningful to the patients and widely neglected. 15 Not many quantitative studies evaluated the interictal burden of migraine, yet. Among episodic migraine patients, an interictal burden has been reported in 10% to 26% of the cases. 16 Additionally, when assessed using the Migraine Interictal Burden Scale (MIBS-4), findings indicate that the interictal burden exhibits a moderate correlation with migraine-related disability and a weak correlation with attack frequency. 17
Therefore, following on from the available literature, it is crucial and necessary to quantitatively evaluate the interictal migraine burden, especially to better understand fear of attacks. A tool to evaluate fear of attacks is the self-reported Fear of Attacks in Migraine Inventory (FAMI),18,19 which assesses the attack anxiety in migraine patients, considering fear of negative consequences, attention and anticipation, as well as fear and avoidance behaviour. The tool was developed in 2022 and has not been used in additional studies, yet. During its development, it was shown to be correlated to the frequency of attacks and headache-related disability as well as psychological variables. 19 For a targeted patient management, it is important to understand, whether this relationship is a simple co-existence of different aspects of a disease or whether and to which extent fear of attacks is influenced by other variables.
Aim of the study
The aim of the study was to evaluate the factors influencing fear of the next attack in patients with episodic migraine, and to investigate the differences between individuals with low and high attack anxiety, according to the FAMI questionnaire, considering headache impact, central sensitization, allodynia symptoms and neck disability.
Methods
This cross-sectional study is part of ‘MigrainePREDICT – influencing factors for the onset of migraine attacks’ project and it has been pre-registered on the Open Science Framework platform (doi.org/10.17605/OSF.IO/CTKHM) and approved by the Ethics Committee at the Universität zu Lübeck (file number: 2023-725). All participants provided written informed consent prior to the data collection.
Participants
A total of 46 patients with migraine and 47 healthy controls were recruited for the MigrainePREDICT study. Only the data of patients with migraine were analysed for the purpose of this substudy. The recruitment occurred through campus advertising and social media. Included were participants older than 18 years and diagnosed with episodic migraine by a medical doctor. Due to other research aims of the project, patients were excluded if they had:
Headache on the day of the examination Other headache diagnoses or other neurological disease Systemic diseases (e.g. rheumatic diseases) Neck injuries, e.g. rear-end collision in the last 10 years Other diagnoses that affect the muscles or joints of the cervical spine Psychiatric illnesses untreated Other reasons for increased pain sensitivity Pregnancy or breastfeeding Use of painkillers in the past 48 h.
Measurements
Statistical analysis
The statistical analysis was conducted using the statistical software R. For the descriptive analysis, the relevant variables (socio-demographic data, as well as headache characteristics, FAMI, NDI, HIT-6, CSI and ASC-12) were analysed using means or medians, standard deviations, and percentages.
A multiple linear regression was used to examine which variables influence attack anxiety according to FAMI questionnaire. The dependent variable for the regression analysis was the FAMI total score, and HIT-6, ASC-12, CSI and NDI scores were used as predictor variables. In preparation for the multiple regression, multicollinearity, the variance inflation factor [VIF] and the tolerance value were assessed.
The FAMI questionnaire was analysed considering the total score and the scores of the three subscales (fear of negative consequences, attention and anticipation and fear-avoidance behaviour). Shapiro-Wilk test was used to analyse whether FAMI values were normally distributed.
The cut-off value of 116 points for a high level of attack anxiety, as suggested by the original authors of the FAMI, reflects a threshold above which individuals are considered to exhibit significant fear of the next migraine attack. However, it is important to note that this threshold was not reached by participants in either of the clinical groups (migraine with and without aura, and chronic migraine) used in the original validation study. 19 Additionally, while a percentile rank of ≥84 has been proposed for diagnostic screening purposes, the method used to establish this specific value was not detailed. 19 In the present study, only patients with episodic migraine were included, a population not directly addressed by the original cut-off definitions. Therefore, in the absence of an established cut-off value tailored to this specific group, and in order to enable a more balanced categorization of participants, we adopted a data-driven approach using the median of the sample distribution. A cut-off value of 81 points was defined, classifying participants into two approximately equal groups: scores <81 indicating low fear of the next attack, and scores >81 indicating high fear. This approach allowed for a more representative and internally consistent classification within our specific sample.
Exploratory t-test were used to evaluate the difference between high and low FAMI groups considering sex, age, and migraine impact, central sensitization, allodynia symptoms, and neck disability.
Results
Of the 46 patients with migraine, approximately 80% were female and the mean age was 33.8 years. All socio-demographic data and characteristics are shown in Table 1.
Socio-demographic data and characteristics of headache in episodic migraine patients (mean, standard deviation and percentage) (n = 46).

SD: standard deviation.
The mean FAMI score was 79.4 points. Score distribution and results for the three subscales are shown in Table 2.
Results of the FAMI questionnaire total score and subscales (n = 46).

FAMI: Fear of Next Attack in Migraine Inventory; SD: Standard deviation.
All prerequisites were met for the multiple linear regressions. The overall regression model including the predictors NDI, CSI, ASC-12 and HIT-6 was statistically significant [F = 14.138, p < 0.001; R2adjusted = 0.352] and correctly classified 35.2% of individuals according to the FAMI questionnaire. The chosen model showed that significant factors that influence fear of the next attack are allodynia (p = 0.009) and headache-related disability (p = 0.033) (Table 3).
Results of the linear multiple regression with FAMI as the dependent variable.

NDI: Neck Disability Index; CSI: Central Sensitization Inventory; ASC-12: Allodynia Symptom Checklist; HIT-6: Headache Impact Test; VIF: variance inflation factor; FAMI: Fear of Attacks in Migraine Inventory. The values in bold type indicate statistically significant P-values (P < 0.05).
When stratifying patients into two groups according to the FAMI median split (81 points), there were significant differences between the groups with high and low fear anxiety for central sensitization, neck disability, headache impact and allodynia, while there was no significant difference regarding age (Table 4).
Differences between patients with a low and high FAMI score.
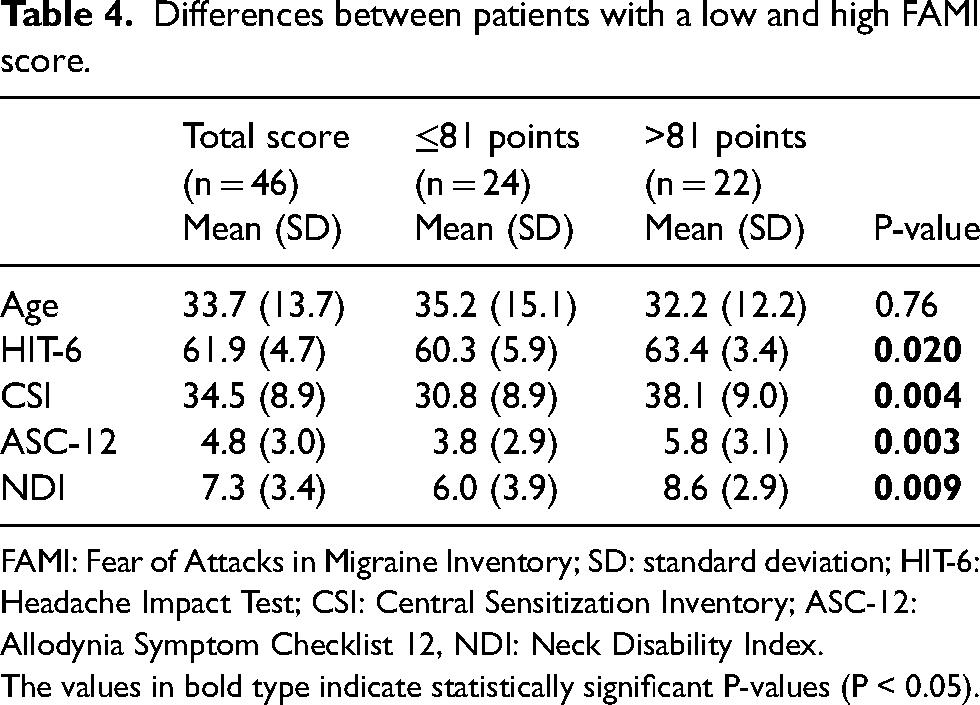
FAMI: Fear of Attacks in Migraine Inventory; SD: standard deviation; HIT-6: Headache Impact Test; CSI: Central Sensitization Inventory; ASC-12: Allodynia Symptom Checklist 12, NDI: Neck Disability Index. The values in bold type indicate statistically significant P-values (P < 0.05).
Discussion
This study aimed to explore the influence of variables typically associated with migraine onto fear of attacks as one of the main interictal burdens of the disease. The results revealed that 35% of the fear of the next attack was explained by headache impact and allodynia symptoms (p < 0.001). When the sample was stratified based on the FAMI media split score, significant differences emerged between the groups regarding headache impact, central sensitization, allodynia symptoms and neck disability with the high scoring FAMI group consistently showing higher levels of impairment.
The impact of migraine significantly affects the individual's behaviour, career, daily activities and social functioning. 9 Results from the current dataset implicate that this impact also contributes to the fear and anxiety surrounding the next attack, as patients remain uncertain about when the next episode will occur. If fear is considered a stress response 24 and stress is reported as one of the most common triggers for a migraine attack, 24 this might contribute to the creation a self-perpetuating vicious cycle exacerbating the overall burden of the disease. Fear of attacks was considered a very specific feature in individuals who experience recurring attacks of headache, 18 however, in the present study, although only two of the 46 episodic migraine patients reached the cut-off value of 116 points in the FAMI proposed by Klan et al. (2022). 19 On the other hand, only one participant had a FAMI score of less than 40 points, while 25% of the patients achieved FAMI scores between 90 and 110 points. These results suggest that attack anxiety affects a considerable proportion of the patients in the sample surveyed although only patients with episodic, not with chronic migraine were included. This might be particularly relevant since the authors of the FAMI questionnaire also pointed out that results in the middle range can indicate treatment-relevant attack anxiety. 18
The overall model explained 35% of the results from the FAMI questionnaire and showed that self-rated disability and allodynia symptoms in combination significantly influenced the fear of attacks in episodic migraineurs. It seems natural that the fear of attacks is stronger when the migraine attack is accompanied by more severe symptoms and when migraine limits daily functioning. Hence, these two aspects are important to address and evaluate in patients with migraine to reduce the additional stress imposed by fear of attacks.
Clinical studies suggested that two-thirds of migraine patients develop allodynia symptoms, 6 and since it is a marker of central sensitization, it is considered a risk factor for progression to chronic migraine. 25 Up to 63% of migraine patients present allodynia in the ictal phase, 26 but some patients also report interictal allodynia. 27 Allodynia was related to poorer clinical outcomes such as increased migraine disability, 28 worse quality of life and it was also associated with psychiatric symptoms, being exacerbated by acute stress. Besides, allodynia is negatively related to one's own self-efficacy. 29 Taking this information into account, the current results are well aligned with previous knowledge on the negative influence of perceived allodynia on migraine symptoms.
Fear of attacks has been identified as a distinct characteristic in individuals with recurrent headache disorders, such as chronic migraine, compared to those with episodic migraine with and without aura. 12 However, the findings of this study reveal a divergence, as nearly half (48%) of episodic migraineurs demonstrated a high fear of attacks when using 81 points as a cut-off level for a high level of fear. This observation underscores that factors beyond attack frequency contribute to the fear and anxiety surrounding future migraine episodes, highlighting their role in the interictal burden of migraine. Furthermore, within the migraine cycle, certain comorbidities such as allodynia symptoms, 6 central sensitization, 7 and neck disability 21 manifest not only during attacks but also in the interictal period, exacerbating the overall impact on patients.
More surprisingly, CSI scores did not influence the level of fear of attacks. This questionnaire was designed to provide a proxy for central sensitization and investigates various symptoms that are frequently observed in chronic low-back pain, knee osteoarthritis 30 and chronic musculoskeletal disorders. 31 The questionnaire has been previously used in migraine populations.30–35 However, the use of the CSI to indicate central sensitization in patients with migraine should be questioned, since a number of the items on the questionnaire are typical migraine symptoms, such as headache, temporomandibular pain, nausea, disturbed sleep, impaired cognition and sensitivity to light. Therefore, patients with migraine will always score higher on the CSI than healthy control participants by simply reporting their migraine-related symptoms. Data from this current study indicated that CSI scores did not correlate with allodynia symptoms and also not significantly contribute to fear of attacks, while allodynia significantly influenced FAMI scores.
Previous research indicated that in patients with migraine who additionally suffered from neck disability, the NDI questionnaire showed a high correlation with allodynia symptoms and migraine impact and did not relate to cervical musculoskeletal dysfunction. 36 A systematic review showed that neck disability scores are higher in individuals with chronic migraine compared with episodic migraine. 37 In this current sample, neck-related disability was considered mild in patients with high or low fear of the next attacks, hence neck disability did not seem to influence whether patients had a high level of fear of attacks. However, these results might be different in samples with higher levels of neck-related disability and a higher frequency of migraine attacks.
While this study provides valuable insights into the role of fear of attacks in the migraine syndrome, several limitations should be considered. The sample consisted only of individuals with episodic migraine, and it is likely that chronic migraine will be associated with a greater fear of attacks. Despite this, the findings emphasize the need to assess fear in individuals with less frequent episodes. The FAMI questionnaire, introduced only recently, lacks standardized data, and although a cut-off score of ≥116 points is recommended for migraine with and without aura and chronic migraine, this study adapted it for episodic migraine. Additionally, the study did not differentiate between mild, moderate or severe attack anxiety, which may limit its representativeness of the broader episodic migraine population. The FAMI questionnaire does not account for medication use, and future studies could benefit from examining the relationship between medication consumption and attack anxiety and explore the connection between attack frequency and coping strategies.
Conclusion
Fear of the next migraine attack plays an important role in individuals with episodic migraine, particularly those with increased headache impact and allodynia symptoms. Furthermore, key migraine-related factors such as central sensitization, neck disability, headache impact and allodynia symptoms show significant differences based on the level of the fear of the next attack. These findings underscore the critical role of fear and anxiety of the next attack in shaping the overall interictal burden of migraine, and it provides possible treatment targets that address the fear itself or the two contributing variables allodynia and headache impact.
Clinical implications
Among episodic migraine, headache impact and allodynia symptoms are significant factors contributing to fear of next migraine attacks.
Individuals with high attack anxiety exhibit greater headache impact, central sensitization, allodynia symptoms, and neck disability.
Addressing headache impact and allodynia symptoms using validated tools such as the HIT-6 and ASC-12 questionnaires may help clinicians identify patients in need of targeted management strategies to reduce interictal burden and improve quality of life in individuals with episodic migraine.
Footnotes
Acknowledgements
Not applicable.
Ethics
All participants provided written informed consent prior to the data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed, in part, by the São Paulo Research Foundation (FAPESP), Brazil. [Grant no. 2023/00357-8].