
Abstract
Objective
To investigate the association between the presence of self-reported neck pain in patients with migraine and clinical features, upper cervical mobility, and neck muscle performance.
Methods
A total of 142 patients with migraine were recruited and stratified by the presence (n = 99) or absence of self-reported neck pain (n = 43). The clinical examination included the Migraine Disability Assessment, the 12-item Allodynia Symptom Checklist, a flexion rotation test, and the Craniocervical Flexion Test.
Results
Migraine-related disability was reported by more than 80% in both groups (p = 0.82). However, there was a greater prevalence and severity of cutaneous allodynia observed in the group with neck pain (p < 0.001). Reduced upper cervical mobility was verified in 67% of the patients with neck pain and in 41% of those without neck pain (p = 0.005). In addition, 67% of the patients with neck pain and 40% without neck pain were not able to maintain the third stage of the Craniocervical Flexion Test without compensation (p = 0.003).
Conclusions
The presence of self-reported neck pain in patients with migraine was associated with a poor clinical presentation regarding cutaneous allodynia, neck mobility, and muscle function. However, there were no differences in migraine-related disability.
Introduction
A migraine is usually categorized according to the presence or absence of aura and by the frequency (episodic or chronic) of migraine attacks as suggested by the International Classification of Headache Disorders (1). In fact, recommendations of the International Headache Society in relation to headache diagnosis have undoubtedly been very useful in researching development and clinical practice. However, this migraine categorization has also been criticized because a migraine exhibits a wide clinical spectrum (especially the chronic subtype), and its diagnosis relies on a cut-off frequency based on an arbitrary number of attacks (2,3).
Ongoing debates arise on the alternate possibility of identifying subgroups of migraine patients to facilitate biological and genetic characterization, to describe specific phenotypes, to better predict migraine prognosis, and to move toward more effective treatment proposals (2,4). Among all comorbid and concomitant symptoms and conditions present in patients with migraine, particular attention has been paid to the presence of neck pain. Neck pain is recognized as a very frequent symptom reported by patients with migraine either during the migraine attacks, preceding the attack, or even interictally (1,2,5–7). According to Viana et al. (8), 91% of patients presenting with self-reported neck pain also have migraine attacks (diagnosed as a migraine or probable migraine), without evidence of causative pathological conditions of the cervical spine.
It has been also found that neck pain is a potential contributor to migraine-related disability (9) and it has a negative influence on acute pharmacological treatment (10). Moreover, several functional (11), sensory (12,13) and musculoskeletal disorders of the cervical spine including altered posture (14), reduced range of motion (15,16), hypomobility of C1-C2 segment (17–19), lower force production, and altered neck muscles control have been associated with migraine (19–21).
To date, there are no studies investigating differences in the clinical profile of patients with migraine, stratified by the presence of self-reported neck pain. Therefore, the aim of this study was to investigate if the presence of concomitant neck pain was associated with the clinical features of a migraine, the presence and severity of cutaneous allodynia, and cervical musculoskeletal dysfunctions. Our hypothesis was that patients who reported neck pain would present with a more severe migraine phenotype characterized by greater migraine-related disability, a more prevalent and severe cutaneous allodynia, and higher cervical musculoskeletal dysfunctions than those migraine patients without neck pain.
Methods
Patients with migraine were consecutively recruited during a headache outpatient clinic routine examination between February 2015 and March 2017. To be included, patients had to be between 18 and 55 years old and diagnosed with a migraine according to the beta version of the third edition of the International Classification of Headache Disorders (ICHD-3 beta) (22). Exclusion criteria included another concomitant headache diagnosis, any potential systemic disease, other neurological disorders, history of head or neck trauma, diagnosis of cervical pathology such as disc disease, pregnancy or lactation. Patients were classified as having migraine either with or without neck pain. Criterion to be included in the migraine with neck pain group was the presence of neck pain episodes over at least the past 3 months with an intensity greater than 3 points on a 11-point numerical pain rating scale (NPRS) on most days when neck pain occurred. This quality criterion was adopted to avoid episodes of low intensity that might occur frequently in the general population (23) or new incident and acute cases of undiagnosed neck pain. The study protocol was approved by the local ethics committee (process n° 16692/2012) and all participants gave their informed consent.
Inclusion and exclusion criteria were first checked from the patient’s records, and then an examiner invited those patients attending the clinic to join the study and confirmed the criteria. Patients responded to a structured questionnaire about migraine characteristics, such as years with the disease, mean intensity of the migraine headache using an NPRS, frequency (days per month) and duration (hours) of migraine attacks, and neck pain characteristics such as frequency, intensity, and timing of the symptoms.
The frequency of questionnaire responses and the accomplishment of the tests varied among individuals because data collection was performed during an outpatient routine. These proportions are described in Figure 1. The Migraine Disability Assessment (MIDAS) (24) and 12 item Allodynia Symptom Checklist (ASC-12) (25) were assessed during the personal interview. Subsequently, an experienced and trained examiner, blinded for the presence/absence of neck pain, conducted the flexion rotation test (FRT) to assess the mobility of the upper cervical spine (C1/C2 segment) and the Craniocervical Flexion Test (CCFT) to evaluate the deep cervical flexors’ function.
Flow diagram of participants’ selection.
Questionnaires
The MIDAS is a five-item questionnaire classifying migraine-related disability according to the impact of migraine attacks on the subject’s professional and social life. The MIDAS classification includes: No disability (0–5 points), mild disability (6–10 points), moderate disability (11–20 points) and severe disability (21 or more points) (24).
The ASC-12 is a 12-item questionnaire aiming to identify the presence and severity of cutaneous allodynia based on the discomfort or pain felt during migraine attacks when performing daily activities, such as combing hair or wearing glasses. It scores up to 24 points and it is classified as: No allodynia (0–2 points); mild allodynia (3–5 points), moderate allodynia (6–8 points) or severe allodynia (9 or more points) (25).
Cervical spine examination
The mobility of the C1-C2 segment was assessed by the FRT using the Cervical Range of Motion (CROM®) device attached to the patient’s head. Participants were placed in a supine position with the head supported by the examiner’s hand, which performed a maximal passive flexion of the cervical spine followed by a maximum passive cervical rotation to each side (26,27). The final passive range of motion was determined when the examiner perceived resistance or when the patient reported pain in the upper cervical segment (26,27). The FRT was reported as positive when subjects reported a range of motion lower than 34° for either right or left rotation (26,27).
The CCFT is a neuromuscular control and low-load test used to evaluate the activation and endurance of the deep neck flexors (28). The test was performed with the subject in a supine position, with a pressure biofeedback unit (Stabilizer, Chattanooga South Pacific; USA) placed behind the neck and inflated to 20 mmHg. The patients were instructed to perform a gentle and slow head-nodding action of craniocervical flexion over five incremental stages of increasing range (2 mmHg each stage), with each stage being maintained for 10 s. Subjects performed two repetitions of 2 s at each stage to familiarize themselves with the task. During this familiarization test, signs of inappropriate performance such as head retraction, head lift, or difficulty relaxing after the contraction were discouraged. Subjects then performed the CCFT holding each target level for 10 s, with a 30-s rest period between levels without any control of compensations. The test was interrupted once any compensation was identified, such as simultaneous palpable contraction of the superficial flexors. The latest stage performed without any compensation was registered as the targeted level (28).
Statistical analysis
Data analysis was conducted using the SPSS 20.0 software, adopting a significance level of 0.05. Descriptive analyses were applied to characterize the sample and to report main variables with their means, standard deviations, frequencies of observations by counts, and percentages. The normal distribution of dependent variables was verified by histograms, comparing between the residual versus theoretical quartiles of a standard normal distribution and confirmed by the Shapiro-Wilk test.
As normal distribution could not be confirmed for all the variables, the main analysis was performed using the Mann-Whitney U test. Comparisons of age, body mass index (kg/cm2), number of years with migraine, and frequency, duration and intensity of migraine attacks were made between the migraine groups with and without neck pain. This test was also applied to compare the range of motion of the FRT.
In order to verify whether there is evidence of an association between the presence of neck pain in patients with migraine and the categorical variables, the Chi-square test (χ2) was used. The comparison between groups was performed with the following criteria: Proportions of females versus males, presence and severity levels of migraine-related disability, presence and severity levels of cutaneous allodynia, positive rates of FRT, and CCFT stages.
In addition, the magnitude of the association was verified by the prevalence ratio of categorical and severity levels as a function of the presence of self-reported neck pain. The prevalence ratio was calculated to verify the association to the risk of presenting with: Any migraine-related disability and each of the severity levels indicated in the MIDAS; cutaneous allodynia and the severity levels classified according to the ASC-12 scores; and positive FRT based on the cut-off of <34°. The prevalence ratio was preferred to the odds ratio because of the considerable “overestimation” of the strength of association by the latter in cross-sectional studies (29).
Results
Among 153 eligible patients, 11 were excluded for having a concomitant diagnosis of other type(s) of headache; therefore, a total of 142 patients (93%) were included (Figure 1). Ninety-nine (n = 99, 70%) patients reported the presence of neck pain (migraine with neck pain), whereas the remaining 43 (30%) did not (migraine without neck pain).
Sample characteristics.

Note: Data are presented as mean and standard deviation.
Mann-Whitney U test.
Migraine-related disability in patients with migraine stratified by the presence of neck pain.

χ2 = 0.05; p = 0.82.
χ2 = 3.90; p = 0.14.
MIDAS: Migraine Disability Assessment; PR: Prevalence Ratio, taking as reference the migraine group without neck pain and without disability; 95% CI: confidence interval of 95%.
Cutaneous allodynia classification in patients with migraine stratified by the presence of neck pain.

ASC-12: 12 item allodynia symptom checklist.
χ2 = 22.60; p < 0.001.
χ2 = 0.09; p = 0.95.
PR: Prevalence Ratio, taking as reference the migraine group without neck pain and without allodynia; 95% CI: confidence interval of 95%.
Flexion rotation test (FRT) in patients with migraine stratified by the presence of neck pain.

χ2 = 7.83; p = 0.005.
Mann-Whitney U test.
ROM: Range of Motion; SD: standard deviation; PR: prevalence ratio, taking as reference the migraine group without neck pain and negative FRT; 95% CI: confidence interval of 95%.
Finally, significant differences in the performance of CCFT were also identified between groups (χ2 = 15.72; p = 0.003): In the migraine group with neck pain, there was a worse performance on the CCFT as 67% of them did not reach the third stage (26 mmHg). However, in the migraine group without neck pain this occurred in only 40% of subjects (Figure 2).
Craniocervical flexion test (CCFT) performance of patients with migraine stratified by the presence of neck pain (n = 121/χ2 = 15.72; p = 0.003).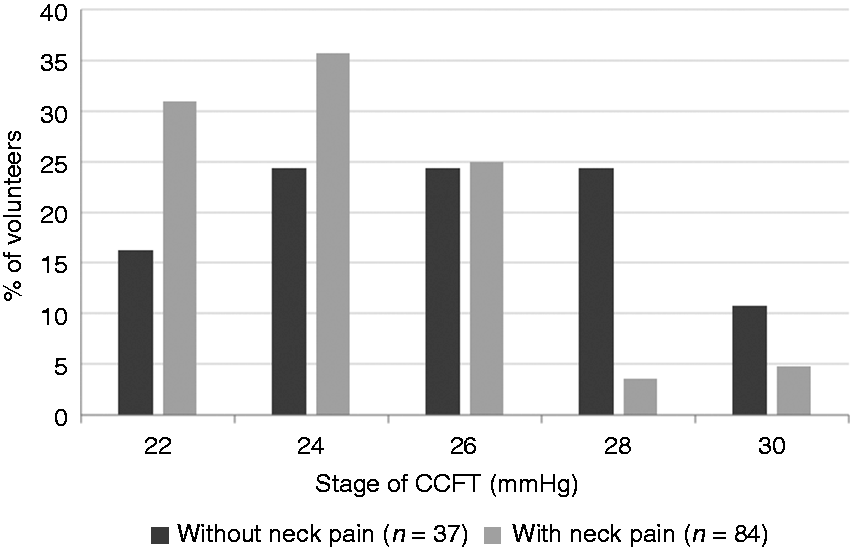
Discussion
The current findings partially confirm our initial hypothesis that patients with migraine and neck pain would present with a more severe migraine phenotype. Indeed, the presence of neck pain in patients with migraine was associated with female sex and a greater risk of presenting with cutaneous allodynia, reduced upper cervical mobility, and poor deep cervical flexor performance. On the other hand, there were no observed differences in migraine-related disability, age, BMI, and migraine features between the two groups.
The absence of a significant association between the presence of neck pain and a more severe migraine-related disability is in accordance with the findings reported by Aguila et al. (30). They also demonstrated that the neck pain reported by the patients was not related to migraine-related disability, nor with the frequency and intensity of the migraine attacks. Despite being highly prevalent in the general population, neck pain is not usually associated with severe disability in daily activities (23,31). In both studies, migraine-related disability was measured by the MIDAS. Therefore, it is logical to conclude that the additional effect of experiencing neck pain as a concomitant symptom does not contribute to absenteeism from work, nor does it affect the social interaction of the migraine patients, since the impact of migraine itself is the most important one. However, it does not exclude the relevance of the relationship between neck pain and migraine-related disability, as this has already been reported as a negative predictor for treatment efficacy in reducing migraine-related disability (30).
The prevalence of cutaneous allodynia observed in our sample of patients with migraine is consistent with estimates that two thirds of these patients would have this symptom (25,32). However, we found that when the migraine was associated with neck pain, the prevalence of cutaneous allodynia was approximately 95%. Moreover, the migraine group with neck pain had an increased association to presenting with any level of severity of cutaneous allodynia based on the PRs for mild (PR: 3.4), moderate (PR: 3.6), and severe cutaneous allodynia (PR: 3.5). These findings suggest that the coexistence of neck pain in the migraine clinical presentation may be related to central sensitization because of its association with a higher prevalence and severity of cutaneous allodynia. Considering the well-known migraine chronification risk attributed to the presence of cutaneous allodynia (33), and previous reports of a negative migraine prognosis associated with both cutaneous allodynia and neck pain (9,30,34,35), these interactions should always be investigated in clinical practice.
In our study, female patients tended to report greater proportions of neck pain concomitant with a migraine than male patients. This supports findings from a recent review reporting that women with migraine present with a worse clinical presentation (i.e. greater duration of attacks, greater risk of recurrence, worse disability) and need more time to recover from an attack than men (35). However, in the same review, it was demonstrated that sex differences regarding the musculoskeletal comorbidities remain controversial (35).
The presence of concomitant neck pain was also associated with a greater risk of reduced upper cervical mobility based on positive rates of FRT. Although this represents a biomechanical alteration and causality cannot be confirmed in our design, it is an important finding for the clinical management of patients with migraine. A poor clinical prognosis has been also related to a positive FRT, as noted in a previous study by Aguila et al. (30). It was shown that patients with a positive FRT are six times more likely to present with no effect in reduction of migraine-related disability after treatment (30).
The FRT has been used as a differential diagnosis test for cervicogenic headache (36). For this reason, one might question whether our results are related to a concomitant cervicogenic headache in our sample. It is noted that the possibility of co-occurrence of two or more types of headaches exists. Therefore, patients whose headache diagnosis was not clearly defined, and those with concomitant cervicogenic headache, were excluded from the study. In addition, if a patient has neck pain or a cervical musculoskeletal impairment along with a headache, this is not sufficient to fulfill the cervicogenic headache diagnosis criteria and the causal relationship between them should be confirmed (1). A recent systematic review reported a risk of inflating the diagnostic accuracy of the FRT to identify a cervicogenic headache, as previous studies that assessed this presented with small sample sizes and/or asymptomatic controls (36). Moreover, some studies that followed this diagnostic criteria report (18,19,37), and even a recent metanalysis, confirmed that patients with migraine also differ significantly from controls at the FRT (38). This does not mean that a reduced FRT is not an important characteristic related to cervicogenic headache, but it might not be exclusively related to this secondary headache.
Although poor performance on the CCFT has already been associated with migraine (19), our study is the first one demonstrating that if the patient self-reports neck pain the CCFT performance is expected to be worse. As our patients were assessed in the interictal phase, it is possible to suggest that altered recruitment of deep neck muscles persists even without the presence of migraine pain.
Regardless of the above-mentioned negative impact of neck pain on the clinical presentation of migraine, the proportion of patients with migraine that did not report neck pain, but still presented with cervical dysfunctions, cannot be ignored. Approximately 40% of this group presented with a positive FRT and poor performance on the CCFT. This may suggest that some cervical dysfunctions are related to the migraine itself and would be worse when associated with pain symptoms. If this is true, it can be hypothesized that migraine is not only characterized by sensory system sensitization (as a consequence of hyper-excitability of the central nervous system) (39), but there is also an association with an altered efferent system that affects motor control and mobility of the craniocervical area. From a scientific perspective, this subgroup draws particular attention and could be better investigated regarding its natural prognosis and treatment response. From a clinical perspective, we advise clinicians to consider and not ignore the cervical musculoskeletal dysfunctions, even when migraine patients do not report neck pain symptoms.
Finally, some limitations of the current study should be recognized. First, the data was collected from a tertiary center, in which the most severe clinical presentations of migraine are seen. Due to the ambulatory routine and availability of patients, it was not possible to guarantee participation of all individuals in all proposed tests. Moreover, as women tend to seek care more frequently, our results may overestimate sex differences (35). This suggests that careful interpretation should be made in order to translate our findings to the general population. Finally, because of the current study design, we cannot assume any causal relationship between factors. However, the strengths of the current study should be considered. It is the first report comparing migraine groups stratified by the presence of neck pain, even though the potential negative interaction was raised as a hypothesis in several reports. By stratifying the patients, it was possible to demonstrate the association of neck pain and migraine with a greater prevalence and severity of cutaneous allodynia, reduced upper cervical spine mobility, and poor neck muscle endurance. These findings might be helpful to guide clinical musculoskeletal assessments, and to optimize treatment in patients with migraine.
Conclusions
The presence of neck pain in patients with migraine was associated with the presence of cutaneous allodynia, a reduced upper cervical range of motion (C1-C2), and poor neck muscle performance compared to that in patients with migraine not reporting neck pain. This should be further investigated in future clinical trials. In addition, recognition of this concomitant symptom during the clinical examination of a migraine patient may signal a more severe clinical presentation.
Clinical implications
Self-reported neck pain in patients with migraine is associated with a greater prevalence and worse severity of cutaneous allodynia. Worse cervical musculoskeletal dysfunction is associated with neck pain in patients with migraine. Neck pain does not seem to be associated with migraine features and with migraine-related disability. Cervical musculoskeletal dysfunction may be present in 40% of those patients that do not report neck pain.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the Fundação de Amparo à Pesquisa (FAPESP) and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior-Brasil (CAPES), Finance Code 001.