
Abstract
Background:
Non-dental orofacial pain disorders are not uncommon, but idiopathic or primary facial pain syndromes are rare. Inadequate recognition of these disorders usually leads to unsatisfactory and unmet treatment needs.
Methods:
We conducted a narrative review with a literature search in PubMed until December 2021, focusing on current guidelines and the recently published International Classification of Orofacial Pain (ICOP).
Results:
In this paper, we provide an updated overview of the common orofacial pain disorders following the ICOP, covering the classification, epidemiology, pathophysiology, clinical approaches, and treatment options. Additionally, we propose a pragmatic approach focusing on the attack duration to improve distinguishing orofacial disorders.
Conclusion:
The introduction of ICOP offers the opportunity to better coordinate and concentrate scientific efforts, which lays the foundation for the identification of the disease mechanism of facial pain disorders and the optimization of the currently still insufficient therapeutic strategies.
Introduction
Orofacial pain refers to pain within the trigeminal system. The demarcation between orofacial pain and headache lies in the involved trigeminal dermatomes. Headache involves the ophthalmic branch (V1) of the trigeminal nerve and the dermatomes of greater and lesser/least occipital nerves, whereas facial pain, according to the latest International Classification of Headache Disorders (ICHD-3), is defined as pain below the (infra-)orbitomeatal line, anterior to the pinna, and above the neck, 1,2 an area innervated by the maxillary (V2) and mandibular (V3) branches of the trigeminal nerve. Contrary to headache disorders, in which primary headache disorders predominate, facial pain is more commonly due to secondary causes. Inflammation or infection of craniofacial structures often leads to facial pain, such as sinusitis and dentoalveolar diseases. 3 Orofacial pain is present in approximately 10% of patients with primary headache disorders. 4 Facial pain, in this case, is a symptom of primary headache disorders, such as migraine 5 or cluster headache. 6 Occasionally, diagnostic work-ups reveal no evidence of an organic lesion, and the facial pain itself is the disease – these patients are diagnosed with idiopathic (primary) orofacial pain. 7
Since the common causes of facial pain are secondary to a disorder of an adjacent structure, most commonly a dentoalveolar one, the first-opinion providers for patients with facial pain are usually dentists. 8,9 However, dental diagnostic work-up sometimes reveals no tangible aetiology despite the typical presentation of dental pain. These patients often visited various doctors of different specialities before ultimately pursuing care from a tertiary headache/facial pain centre because of inadequate treatment response. 10 In clinical practice, identifying the aetiology of facial pain can be sometimes challenging. Uncertain diagnosis sometimes leads to (unnecessary) trials of interventions. For example, a dental origin was assumed, and the tooth was extracted, but the facial pain remains unimproved (Figure 1). Multidisciplinary collaboration among specialists (e.g. dentist, otorhinolaryngologist, neurologist) is crucial in establishing an accurate diagnosis. For this purpose, common terminology in classifying facial pain disorders is the critical first step, with the ultimate goal of better understanding facial pain disorders and improving the treatment quality. In this review, we will give an overview of orofacial pain disorders that follows the recently introduced classification of orofacial pain disorders.

Panoramic radiograph of a 44-year-old patient after 12 years of treatment for facial pain. The pain started in the left maxillary branch of the trigeminal nerve. The patient initially received root canal treatment, root removal and finally tooth extraction. Because the pain spread to the neighbouring teeth, subsequently the ipsilateral lower jaw (mandibular branch), and finally switched side, the patient received multiple root canal treatment and tooth extraction. With only few teeth left, the facial pain persists until today.
Classification
With the goal of better classifying orofacial pain disorders, the International Headache Society, the International Association for the Study of Pain, the International Network for Orofacial Pain and Related Disorders Methodology, and the American Academy of Orofacial Pain collaboratively introduced the first edition of the International Classification of Orofacial Pain (ICOP) in 2020. 11 The structure and content follow the logic of the classification of headache disorders (ICHD-3) strictly. 1 Under ICOP, facial pain is divided into six categories (Table 1), with the first four chapters concerning facial pain disorders related to or attributed to another structure in the orofacial region, including Chapter 1: pain attributed to dentoalveolar and related structure, Chapter 2: myofascial pain, Chapter 3: temporomandibular joint (TMJ) pain, and Chapter 4: lesion or disease of the cranial nerve. Chapter 5 introduces facial pain that resembles headache disorders, and Chapter 6 deals with idiopathic (primary) orofacial pain syndrome. Contrary to headache disorders, the differentiation between primary and secondary aetiologies can be sometimes complicated. Therefore, orofacial pain with primary and secondary designations are categorized within the same chapter. Orofacial pain disorders in the first three chapters are primarily treated by dentists, whereas disorders in the remaining three chapters are of non-dental origins and usually require multidisciplinary collaboration among different specialities.
Classification of facial pain according to ICOP. 11
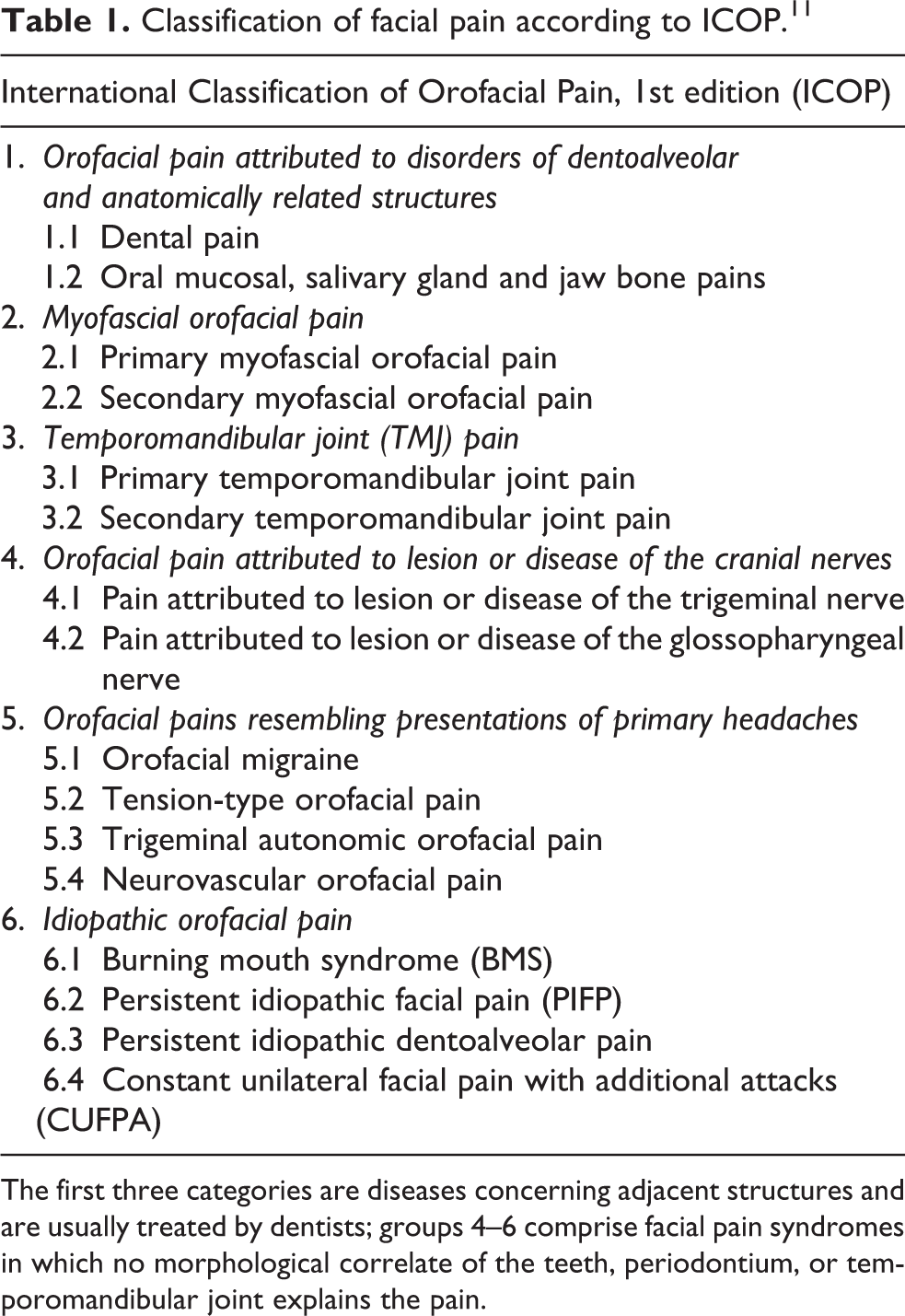
The first three categories are diseases concerning adjacent structures and are usually treated by dentists; groups 4–6 comprise facial pain syndromes in which no morphological correlate of the teeth, periodontium, or temporomandibular joint explains the pain.
Epidemiology
The incidence of facial pain in the general population is low compared with that of headache disorders. In a Dutch study, the estimated incidence rate of (any) facial pain is 38.7 per 100,000 person-years, and women are more commonly affected than men. 12 Another UK study reported the overall prevalence of facial pain of 1.9% in the general population, among which approximately 50% were chronic. Women were twice as likely to be affected than men. 13 The discrepancy between both studies reflects the difficulty in estimating the true prevalence of facial pain partially because of a wide variety in the definition and a lack of common terminology for facial pain. Besides, some patients may consult other specialties, such as otolaryngological practices, because of the pain location, 1,14 which further complicates the estimation of the prevalence/incidence. Disorder-specific epidemiology following the ICOP structure is as follows: The lifetime prevalence of toothache was estimated at 7–32%, and pain or discomfort in the mouth, teeth or gums ranged from 19–66%. 15 The 1-year prevalence of myofascial pain in the jaw-face region ranged from 4% to 19% based on the diagnostic criteria. 16 and the 1-year incidence of temporomandibular joint pain was 8% among university students. 14 Therefore, orofacial disorders categorized under the first three chapters of ICOP are relatively common and probably account for the majority of orofacial pain patients.
For orofacial pain attributed to the cranial nerves, the incidence of trigeminal neuralgia ranged from 4 to 20 per 100,000 person-years, and the prevalence was 0.01–0.02%, whereas the incidence of glossopharyngeal neuralgia is 5–10 times lower compared with trigeminal neuralgia. 17 Epidemiological studies on orofacial neuropathic pain other than neuralgia are still lacking. Concerning facial presentation of headache disorders, community-based epidemiological studies are lacking. However, epidemiological studies of primary headache disorders are abundant. The prevalence of migraine worldwide is 14.4% (13.8–15.0), 18 and 2.3–8.9% of them reported facial involvement, 4,19 corresponding to an estimated 0.3–1.3% of the general population with facial presentation of migraine. Notably, trigeminal autonomic cephalalgias (TACs) are more likely to involve the face (14.8–45%), 4 but their prevalences remain extremely low (0.1%) in the general population. 20 For idiopathic orofacial pain disorders, the incidence of persistent idiopathic facial pain (PIFP) was 4.4 per 100,000 person-years, 12 and the prevalence was 0.03%. 21 These earlier studies were conducted before ICOP, and based on their case definition, some may include patients with neuropathic pain, 22 whereas ICOP now allows differentiation and, therefore, proper investigation. 23 In summary, epidemiological studies on primary orofacial pain disorders remain insufficient. Facial pain due to dentoalveolar or myofascial aetiologies is the most common type of facial pain, followed by the facial presentation of headache disorders because of the high prevalence of primary headache disorders. Neuralgia/neuropathic facial pain or idiopathic orofacial pain remains relatively rare.
Approach to facial pain
History taking and general approach
An accurate diagnosis relies on good history taking. Patients should be allowed to express their symptoms openly. The history taking should focus on the timing, duration, location and radiation of pain, its quality and severity, aggravating/relieving factors, associated symptoms, and/or other accompanying pain conditions. Facial pain due to dentoalveolar causes usually aggravates with temperature change, chewing, or biting. Symptoms of TMJ disorder are often associated with jaw movement. 24 Maxillary sinusitis is commonly accompanied by nasal discharge or associated with lesions in the adjacent structure, e.g. upper posterior teeth. 25 In patients with chronic orofacial pain, a common history is the previous insufficient treatment of acute pain. De novo chronic orofacial pain is rare. Besides, in the process of chronification, the initially localized pain, e.g. dental pain, may spread to neighbouring regions and even cross to the other side. 22,26 A proper diagnosis requires the clinical plausibility of causation and the identification or exclusion of secondary causes, which requires multidisciplinary collaboration.
Dental investigation
In a community-based setting, dental pain accounted for the majority of orofacial pain. 26 In addition to dental pain, myofascial pain and TMJ pain are also diagnosed and treated by dentists. In principle, the dental examination should be exhaustive since the identification/exclusion of a dentogenic focus is essential to establish a correct orofacial pain diagnosis. Dental investigation in facial pain disorders has been reviewed elsewhere in detail. 26
Neurological examination
The focus of the neurological examination targets needs to exclude secondary aetiologies and identify concomitant headache disorders. For this purpose, the neurological examination should focus on the followings: (i) sensory abnormalities, such as the presence/absence of allodynia, hyperesthesia, or sensory triggers in case of neuralgia; (ii) cranial autonomic symptoms and/or associating symptoms such as photophobia in cases of facial presentation of headache disorders; (iii) tenderness or abnormality of the temporal artery in elder patients with clinical suspicion of temporal arteritis. Occasionally, space-occupying lesions or inflammation in the skull base or adjacent structures may accompany facial pain, and the neurological examination may reveal cranial nerve abnormalities, e.g. ophthalmoplegia in cases such as nasopharyngeal carcinoma, Tolosa-Hunt syndrome, or Ramsay-Hunt syndrome. 27
Imaging study
Imaging studies are commonly required to narrow the differential diagnosis. Imaging modalities used by the dental profession may include panoramic tomography (DPT), intraoral radiographs, and cone-beam computed tomography (CBCT). These modalities have been extensively reviewed elsewhere. 28 No guideline exists yet for the indication of neuroimaging in orofacial pain disorders. The indications for neuroimaging studies in headache disorders include new or progressive headaches with red flags, headaches with suspected trigeminal autonomic origins, or in the presence of focal neurological deficits. 29 –32 These principles may be adapted in the evaluation of orofacial pain. The role of neuroimaging study, preferably magnetic resonance imaging (MRI), lies in differentiating certain specific secondary causes: (i) compression of the (trigeminal) nerve root in classic (trigeminal) neuralgia; (ii) space-occupying lesion (or skull base lesion) with trigeminal nerve involvement; (iii) brainstem lesion as in secondary trigeminal neuralgia; (iv) infection or inflammation of craniofacial structures. 3 Neuroimaging studies in patients with idiopathic orofacial pain syndrome are usually unremarkable.
Chronological pattern of orofacial pain
Once secondary/symptomatic orofacial pain is excluded, the next step is to classify the orofacial pain based on the timing/patterns: Is the pain episodic (attack-like) or persistent? Idiopathic orofacial pain and neuropathic pain are nearly persistent, although the pain intensity may fluctuate, and some patients may experience short (up to hours) pain-free intervals. For this reason, idiopathic facial pain syndrome was previously named ‘atypical facial pain’ for its chronic and persistent characteristics, in contrast to the typical facial pain – trigeminal neuralgia, which features short-lasting attacks (1–120 seconds) and attack-free periods. 11,33 The facial presentation of headache disorders is also episodic, the attack duration of which closely resembles the corresponding headache types. For example, facial migraine is featured by attacks that last 4–72 hours and facial cluster headaches of 15–180 minutes. 34 The chronological patterns of orofacial pain disorders are summarized in Figure 2.

Diagnostic clues of orofacial pain disorders based on the chronological pattern. Dental orofacial facial pain (including pain associated with other dentoalveolar and adjacent structures) can present with any chronic pattern. A common history in patients with idiopathic facial pain is a previously inadequately-treated secondary facial pain, e.g. dental pain. TMJ: temporomandibular joint; SUNCT: Short-lasting unilateral pain attacks with conjunctival injection and tearing; SUNA: Short-lasting unilateral pain attacks with autonomic symptoms.
Specific orofacial pain disorders
Orofacial pain attributed to disorders of dentoalveolar structure, myofascial origin, or temporomandibular joint
Orofacial pain disorders concerning the masticatory system cover the first three chapters of ICOP. 11 The classification concerning dentoalveolar structure (Chapter 1) was based on the anatomical structure (e.g. §1.2.2 Salivary gland pain). Under the ICOP system, the classification of myofascial orofacial pain (Chapter 2) and TMJ pain (Chapter 3) differentiates between primary and secondary pain, and primary pain is subdivided into acute or chronic subforms. Disorders in these chapters were exclusively treated by dentists, orofacial pain specialists (a speciality of dentistry) or maxillofacial surgeons. Treatment relies on proper identification of the underlying aetiology and will be tailored based on the corresponding disorder. 35 The current review will focus on the remaining three chapters (non-dental) of orofacial pain disorders.
Neuralgia
Trigeminal neuralgia (TN) is an exemplary condition of facial pain and probably the most well-recognized non-dental facial pain syndrome. Typical clinical features of TN comprise intense shooting or jabbing pain that lasts for seconds, which is nearly always unilateral and involves primarily the V2 dermatome. Another hallmark clinical feature is the triggerability of attacks by touching the skin, chewing, or brushing teeth. 36,37 Despite being categorized as neuropathic pain, most patients fail to show sensory abnormalities in the trigeminal territory. The phenotypes, pathophysiology, and management of TN have been recently reviewed elsewhere. 38,39 The diagnosis of classical trigeminal neuralgia requires the demonstration of neurovascular contact (NVC) to the trigeminal nerve root. 40 However, certain patients have atypical features such as longer duration of pain, background pain, or objective sensory changes, and an NVC is absent. 41 ICOP follows the structure of the latest International Classification of Headache Disorders 1 and divides TN into three different diagnostic categories 11 Besides classical TN, secondary TN is diagnosed when other structural changes involving trigeminal sensory processing can be demonstrated. In the absence of either NVC or other structural changes, idiopathic TN is diagnosed. 11 Sodium channel blockers, e.g. carbamazepine and oxcarbazepine, are the first-line treatment. Other antiepileptic medications such as lamotrigine and gabapentin can also be used as an add-on or an alternative monotherapeutic treatment. 36 Microvascular decompression is indicated in refractory cases with classical TN, and neuroablative procedures may be beneficial but remain the last resort option due to potential complications and adverse events 42
Neuropathic facial pain syndromes other than neuralgia
Despite being categorized under Chapter 4 – orofacial pain attributed to the lesion of the cranial nerves, the clinical presentations of neuropathic pain other than neuralgia may sometimes mimic those of PIFP, especially in chronic cases with bilateral presentations. Both feature persistent and poorly localized pain with (sometimes) fluctuation in intensity. 22 The differentiation of neuropathic pain from idiopathic facial pain thus relies on a documented nerve lesion or disease in the involved area and signs suggestive of neuropathy, including positive signs (allodynia, dysesthesia) or negative signs (numbness, hypoesthesia). 43 Pharmacological treatment of neuropathic facial pain syndromes other than neuralgias usually follows the principle of treating systemic non-orofacial neuropathic pain, including tricyclic antidepressants (TCAs), selective noradrenaline reuptake inhibitors (SNRI), or gabapentin/pregabalin, 43,44 but the response rate may be lower than those in neuralgia. 45
Facial presentation of headache disorders
Typical headache syndromes like migraine or cluster headache are not foreign to headache specialists. However, a group of patients sometimes raises clinical uncertainty due to the atypical location of pain, i.e. those with a facial presentation of primary headache disorders. Orofacial migraine may present with unilateral facial pain attacks lasting for 4–72 hours, involving the V2/V3 dermatomes, and sometimes associated with photophobia and nausea. 46 These patients generally fulfil the diagnostic criteria for the corresponding headache disorders except for the pain location. However, orofacial presentation of headache may subtly differ when compared to the pure headache type. Orofacial migraine, for example, featured fewer migraine-associated symptoms (nausea, vomiting and photophobia) 4 but more frequent cranial autonomic symptoms. 19 The somewhat different clinical presentations may further increase the diagnostic difficulty, but ICOP allows for the first time to differentiate and, therefore, study such subtypes.
In a large clinical cohort study (n = 2,912), the facial presentation was present in 10% of the patients with primary headache disorders, and the V2 dermatome is most commonly involved. 4 Pure facial presentation, defined as no V1 dermatome involvement in the entire disease course, was rare and accounted for only 17 of the 291 patients with a facial presentation, corresponding to a prevalence of 0.6% among patients with primary headache disorders. 4 The prevalence of facial involvement differs in headache disorders: 14.8–45% in those with TAC and 2.3% in those with migraine. 4 Clinical diagnosis strongly relies on the attack duration – the attack duration of facial pain should correspond to the headache diagnosis. For example, the attack of facial presentation of cluster headache lasts for 15–180 minutes. 1 Treatment should follow the corresponding headache diagnoses, and these patients usually respond well to the corresponding headache disorder treatment. 4
Idiopathic facial pain syndromes
These syndromes are rare and comprise four subgroups according to the ICOP: §6.1 Burning mouth syndrome (BMS); §6.2 Persistent idiopathic facial pain (PIFP), previously known as atypical facial pain; §6.3 Persistent idiopathic dentoalveolar pain, previously known as atypical odontalgia; 6.4§ Constant unilateral facial pain with additional attacks (CUFPA). In some patients, idiopathic orofacial pain can be traced back to an initially localized pain. As the disease progresses, the localized pain spreads to adjacent regions and, eventually, involves the contralateral side. When the patient presents to the tertiary orofacial pain centre, the orofacial pain is usually chronic (defined as >2 hours per day for >3 months). In reality, most patients experience continuous pain throughout the day, sometimes with fluctuating pain intensity. The pain rarely disturbs the patients during sleep, and some reported a brief pain-free interval after waking in the morning. Facial pain in patients with CUFPA is somewhat different and consists of two different kinds of facial pain simultaneously – a background continuous pain and an attack-like pain that lasts 10–30 minutes, but without the typical cranial autonomic symptoms, the absence of which differentiates CUFPA from §5.3.4 Hemifacial continuous pain with autonomic symptoms – an equivalent to the facial presentation of paroxysmal hemicrania. 11 Notably, BMS is currently classified under the idiopathic orofacial pain syndromes 11 ; however, accumulating evidence suggests that BMS may be neuropathic pain, whereas electrogustometry indicates Aδ-fibres abnormalities. 47
The treatment of chronic facial pain must be carefully balanced between the benefits and risks. It is of critical importance in treating patients with idiopathic facial pain syndrome, in which no organic lesion can be identified. Up to 50% of these patients received unnecessary interventions, including teeth extraction (45.3%) and root canal treatment (50%), which were not only ineffective, and, in some cases, worsened the existing facial pain. 9 Pharmacological treatment of idiopathic orofacial pain disorders remains empirical. Treatment options commonly include antidepressants (amitriptyline, duloxetine) or antiepileptic drugs (gabapentin and pregabalin). 48 Non-invasive treatment options, such as multimodal pain therapy, can be considered as an add-on therapy to improve the quality of life. Available treatment for idiopathic orofacial pain is not optimal. The principle of ‘do no harm’ should always be reminded. The diagnostic approach and treatment strategy for facial pain disorders are summarized in Figure 3.

A flowchart approach to facial pain disorders and treatment options. §: Facial pain corresponding to the chapter of the International Classification of Orofacial Pain (ICOP). ENT: Ear, Nose, and Throat; Na-Blocker: sodium channel blocker; SUNCT: Short-lasting unilateral pain attacks with conjunctival injection and tearing; SUNA: Short-lasting unilateral pain attacks with autonomic symptoms.
Conclusion
Research in facial pain disorders is burgeoning; however, fundamental research exploring the disease mechanism is to date insufficient. The introduction of the new classification provides a common ground for communication between clinicians with different specialities and basic scientists alike and benefits future research. The ultimate goal is to improve therapeutic options in years to come, and currently, the attention should be focused on improving diagnosis and providing a better understanding of the pathophysiology.
Clinical implications
Orofacial pain disorders should be approached based on their chronological patterns.
Multidisciplinary collaboration is indispensable in diagnosing and treating patients with orofacial pain disorders
The introduction of the ICOP classification offers the opportunity to coordinate and concentrate scientific efforts to the research on orofacial pain disorders
Footnotes
Author contributions
KP: Drafting of the study, data analysis, data interpretation, drafting and writing of the manuscript.
TO: Data acquisition and analysis, data interpretation, drafting and writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Research Foundation, SFB936/A5 to Prof. Arne May. The funding source did not influence study conduction in any way.