
Abstract
Background
Primary headache syndromes such as migraine are among the most common neurological syndromes. Chronic facial pain syndromes of non-odontogenic cause are less well known to neurologists despite being highly disabling. Given the pain localization, these patients often consult dentists first who may conduct unnecessary dental interventions even if a dental cause is not identified. Once it becomes clear that dental modalities have no effect on the pain, patients may be referred to another dentist or orofacial pain specialist, and later to a neurologist. Unfortunately, neurologists are also often not familiar with chronic orofacial pain syndromes although they share the neural system, i.e., trigeminal nerve and central processing areas for headache disorders.
Conclusion
In essence, three broad groups of orofacial pain patients are important for clinicians: (i) Attack-like orofacial pain conditions, which encompass neuralgias of the cranial nerves and less well-known facial variants of primary headache syndromes; (ii) persistent orofacial pain disorders, including neuropathic pain and persistent idiopathic facial/dentoalveolar pain; and (iii) other differential diagnostically relevant orofacial pain conditions encountered by clinicians such as painful temporomandibular disorders, bruxism, sinus pain, dental pain, and others which may interfere (trigger) and overlap with headache. It is rewarding to know and recognize the clinical picture of these facial pain syndromes, given that, just like for headache, an internationally accepted classification system has been published and many of these syndromes can be treated with medications generally used by neurologists for other pain syndromes.
Introduction
Clinicians will not accept the unsophisticated diagnosis of ‘just headache’ since treatment is critically dependent on the specific type of headache syndrome. The overwhelming success of the International Classification of Headache Disorders (ICHD-3) (1) in providing robust clinical criteria to define headache syndromes, is ultimately evident in scientific and treatment success. Neurologists rightly are the primary discipline to approach with headache, that is pain in the first division of the trigeminal nerve, since in addition to the medical history the neurological examination is critical to distinguish primary from secondary headaches (1). However, due to their heterogeneous nature, pain conditions affecting the 2nd and/or 3rd branch of trigeminal nerve, pose diagnostic and management difficulties for neurologists. Chronic orofacial pain that has no dental cause is certainly underdiagnosed and definitely undertreated (2). One of the reasons why we do not recognize chronic orofacial pain as a neurological disease, with the possible exception of trigeminal neuralgia, is that we know so little about its mechanisms and have as yet no specific treatment to offer. The consequence is often a life-long odyssey of affected patients without a correct diagnosis. As a result, management of orofacial pain conditions is unsuccessful and risks irreversible harm to the patient (2,3). Indeed, orofacial pain and its many facets cannot be reduced to trigeminal neuralgia or persistent idiopathic (former: atypical) facial pain. We need to see orofacial pain syndromes as independent and distinct trigeminal disorders which as such need to find recognition in the headache field (4). Our narrative review summarizes the diagnosis and treatment of orofacial pain syndromes highlighting for each of the disorders the relevance for neurologists.
Search strategy and selection criteria
References for this review were identified by searches of PubMed between 1970 and April 2023, and references from relevant articles. The search terms ‘facial pain’, ‘orofacial pain’, ‘atypical facial pain’ ‘headache’, ‘PIFP’, ‘neuropathic’, ‘neuralgia’, ‘treatment’, ‘TMD’ and ‘ICOP’ were used. There were no language restrictions. The final reference list was generated on the basis of relevance to the topics covered in this review.
Diagnosing orofacial pain syndromes
Orofacial pain (OFP) syndromes are diagnosed based on the criteria outlined in the International Classification of Orofacial Pain (ICOP) (5) in harmony with the current headache classification ICHD-3 (1). Due to the interdisciplinary nature of orofacial pain disorders, the ICOP has been developed by dentists, pain specialists and neurologists to seek a consent among specialties and has therefore also been endorsed by the International Headache Society. For example, the recent definitions of trigeminal neuralgia and temporomandibular disorder (TMD) are identical in both classifications, avoiding different definitions for the same disease. ICHD-3 and ICOP can therefore be cited equally but given that ICOP is more specific for OFP it should be favored. A close interaction between dental and neurological specialists is necessary for diagnosing such diseases (4) where the dentists primarily exclude dental and other oral causes and the neurologists or OFP specialists, on the basis of this exclusion, diagnose the specific facial pain and treat the patient (6). Trigeminal neurophysiology (SEP) and neuroimaging of the head (CCT and MRI) may be needed based on the same principles as in headache diagnosis (7,8). Just like in the diagnostic workup of headache disorders, diligent history taking, and neurological examination are key in finding the right diagnosis – and therefore treatment – in non-dental facial pain.
Attack-like orofacial pain
If pain in the orofacial area occurs in clearly described attacks, there may still be a dental cause such as ‘cracked tooth’ or pulpitis; but a non-dental pain condition is also possible, and neurologists should be aware of the relevant conditions. Broadly speaking, attack-like facial pains are subdivided into neuralgias and orofacial variants of headache syndromes. Neuralgias can affect most cranial nerves with the trigeminal, occipital, and glossopharyngeal nerve being the most common.
Neuralgias
Trigeminal neuralgia
In contrast to most other orofacial pain syndromes, cranial neuralgias are well-defined clinical syndromes with a broad consensus among clinicians. As a result, diagnostic criteria have been harmonized in ICHD-3 (1) and ICOP (5) and clear guidelines for clinical management have been developed (9). Due to some similarities in presentation, the most common cranial neuralgia, trigeminal neuralgia, is often misdiagnosed as dental pulpitis, and it is not uncommon that patients with trigeminal neuralgia have received invasive (but ineffective) dental treatment before the correct diagnosis is identified. As the present review focuses on the lesser-known orofacial pain syndromes, we refer to an excellent and exhaustive review on trigeminal neuralgia that has recently been published (10).
Facial presentations of primary headaches
The clinical borders for headache and orofacial pain are often blurred. Migraine and other primary headaches may extend to the maxillary dermatome (V2), sometimes even to the mandibular dermatome (V3) of the trigeminal nerve (11,12). Some patients experience an isolated facial migraine – defined as attacks fulfilling the criteria for migraine located exclusively in the V2/V3 dermatomes (13). The signs and symptoms follow the diagnostic criteria of the eponymous headache syndromes (see Table 1). Facial manifestations of a primary headache present as three types: primary headache that spreads into the face (type 1), orofacial pain which seems to have replaced a former headache but maintained the same clinical phenotype (type 2) and de-novo orofacial pain that resembles the primary headache phenotype without any involvement of the ophthalmic trigeminal branch (type 3). The prevalence of each subtype remains unclear and is probably frequently misdiagnosed and underreported. Isolated orofacial pain replicating headache (type 3) seems rarer (14), and in this specific and complex presentation, underreporting due to misdiagnosis is even more likely.
Clinical characteristics of attack-like non-dental facial pain and treatment options. *neither chronic facial migraine nor facial MOH has yet been described.**analog to migraine therapy. Whether CGRP-antibodies are effective in facial migraine is not known.
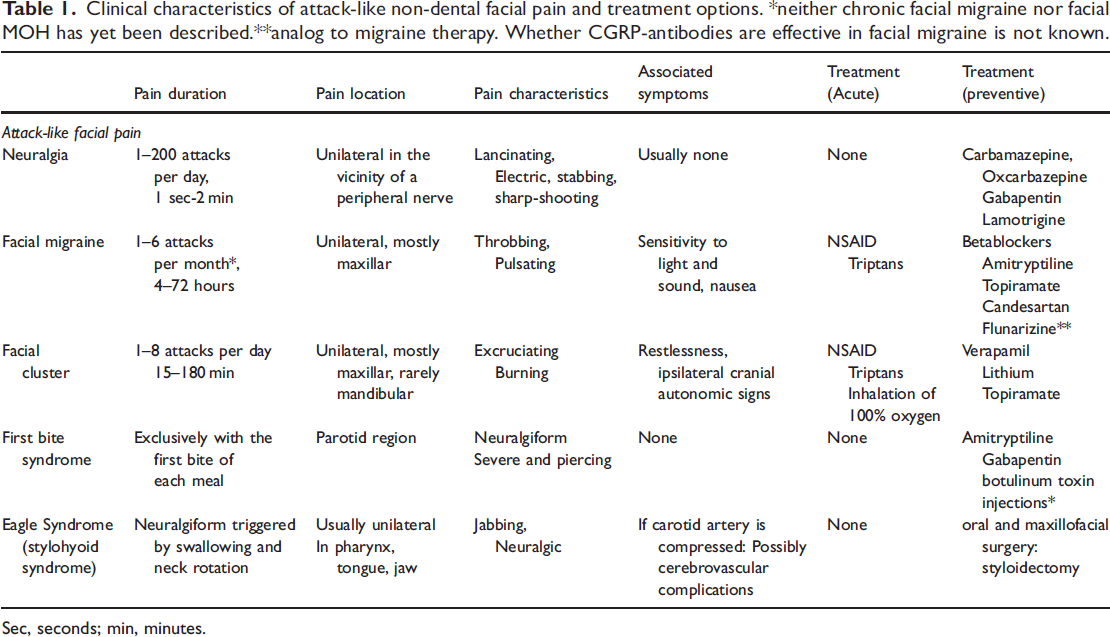
Sec, seconds; min, minutes.
Orofacial migraine
Migraine is probably the first primary headache that ignited interest in the relationship between head pain and facial pain. The fact that migraine involves orofacial structures was already noted by Harold Wolff in 1963 (15). Without clear diagnostic criteria, various terms were assigned such as orofacial migraine, lower-half migraine, or migraine with isolated facial pain (16). Applying the ICOP criteria, series of patients presenting with migraine as isolated facial pain have recently been published (14,17). Although the spread of headache to the face is certainly not rare, isolated migraine in the face is rather uncommon (14). The presentation of isolated V2 migraine, often throbbing, accompanied by mild rhinorrhea, and pain on head movement may additionally lead to misdiagnosis as sinusitis (18–23). As a general rule, facial presentations of migraine is associated with later age at onset (24), and aura is absent or at least less common (14). We note that that neither chronic facial migraine nor facial MOH has been described as yet.
Facial trigeminal autonomic cephalalgias (TACs)
TACs can present in the orofacial region (V2 and/or V3). These findings align with reports of ‘lower face cluster’ (25), and short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT) presenting equally in all trigeminal dermatomes (14,26), and even the facial variant of paroxysmal hemicrania has been reported (27). Autonomic symptoms may vary in facial TAC (14), which raises the question how specific symptoms such as conjunctival injection and tearing are for the diagnosis of TAC or whether these autonomic signs are more specific for the involvement of the ophthalmic division.
Facial variants of short-lasting primary headache
Reports of orofacial variants of primary headache types other than migraine and cluster headache occur with an unclear prevalence. An orofacial variant of idiopathic stabbing headache (28) has been reported. A very peculiar new entity is constant unilateral facial pain with additional attacks (CUFPA) (5,14) where the constant dull pain is intercepted with distinct non-neuralgic pain attacks of a completely different pain character and without any accompanying symptoms, which lasts 10–30 minutes and occurs between two and 20 times per day. These attacks distinguish this type of side-locked facial pain from persistent idiopathic facial pain (PIFP), which is defined as constant orofacial pain without any other positive or negative features and without attacks (5,14).
Treatment
The treatment of a primary headache manifested as orofacial pain is similar to the corresponding primary headache. For example, an orofacial migraine is treated like a migraine and an orofacial cluster headache (CH) is treated like a CH. While there may be subtle differences between a primary headache and its orofacial counterpart, such as for example the prevalence of aura or associated symptoms (14), no data exist whether medications are more or less effective in orofacial variants of primary headaches. The publication of ICOP with its clear criteria will facilitate standardized trials to compare these types (4).
First bite syndrome
Clinical relevance
Although a rare disorder, patients with the diagnosis of first bite syndrome are likely to consult a neurologist or general practitioner rather than a dentist. It is important to differentiate first bite syndrome from other short-lasting paroxysmal facial pains.
First bite syndrome (FBS) is another unusual but very memorable orofacial pain syndrome of severe and piercing pain in the parotid region that eponymously occurs with the first bite of each meal and improves with subsequent bites. Pathophysiology has been attributed to an unbalanced sympathetic/parasympathetic innervation of the parotid gland and the syndrome is mostly seen following surgery of the parotid or parapharyngeal region. The pain lasts seconds to a few minutes and this syndrome is sometimes misdiagnosed as atypical trigeminal neuralgia, but sodium blockers are largely ineffective. In contrast, botulinum toxin injections and medications used for the treatment of neuropathic pain are generally useful (29). However, since the syndrome is rather rare, there is no consensus regarding treatment of FBS, as evidence is limited to case reports/series. A typical differential diagnosis is salivary gland pain due to sialadenitis (see below).
Eagle syndrome
Clinical relevance
The uniform clinical picture of throat pain triggered by jaw opening and particularly swallowing makes it easy to recognize and manage the patient. Serious neurological complications including cerebral infarction and sudden death due to involvement of the carotid arteries are rare but possible (30–32).
The Eagle syndrome (stylohyoid syndrome) is a rare disease characterized by unilateral neuralgiform pain usually in pharynx, tongue and the jaw triggered by jaw opening, swallowing and neck rotation (5,33). Eagle himself described two types of this syndrome (34). In the classic type, the cranial nerves are directly or indirectly irritated by the elongated styloid process after tonsillectomy and in the carotid type, the carotid arteries are impinged by the ossified stylohyoid ligament and the irritated nerve plexus leads to the facial and head pain (35). Repeated compression of the carotid artery may result in cerebrovascular complications. Neurological complications encompass aneurysm, dissection, occlusion of the internal and more rarely the external carotid arteries, transient ischemic attack, cerebral infarction (30,36) and sudden death due to mechanical irritation of the carotid sinus (37).
When a patient complains of oropharyngeal pain in association with the neck and jaw movement, digital palpation of the tonsillar fossa is recommended (36,38). If there is an elongated styloid process, a bony structure may be palpable that triggers the pain and discomfort. Diagnosis of Eagle syndrome should be established with imaging modalities (36). Differential diagnoses include idiopathic cranial neuralgias, migraine and TACs, temporomandibular disorders, ear, nose and throat (ENT) diseases and space occupying lesions.
Treatment
There is no established strong evidence for treatment of Eagle syndrome and the treatment strategy should be discussed based on the seriousness of the patient’s symptoms. Styloidectomy is probably the method of choice and if necessary, carotid stenting should be considered in patients with neurological signs. However, surgical procedures are not always efficient and first line drugs including pregabalin, gabapentin and duloxetine are recommended for the pain (38).
Persistent orofacial pain
When non-dental orofacial pain is persistent and not attack-like, in principle two types exist: the pain is either accompanied with somatosensory changes (for example post-traumatic trigeminal neuropathic pain PTNP) or not (PIFP) (see Figure 1).

Non-odontogenic orofacial pain is divided into attack-like and constant pain syndromes. Attack-like orofacial pain is either a cranial neuralgia or an orofacial variant of a headache syndrome consisting each of three types: primary headache that spreads into the face (type 1), orofacial pain which seems to have replaced the previously existing headache but maintained the same clinical phenotype of the former headache (type 2) and de-novo orofacial pain that resembles the primary headache phenotype without any involvement of the ophthalmic trigeminal branch (type 3). Persistent orofacial pain is either neuropathic with negative and/or positive neurological signs of nerve damage in the area of the pain or, in the absence of such symptoms an idiopathic facial pain, namely PIFP, PIDAP or CUFPA (5).
Post traumatic neuropathic pain (PTNP)
If somatosensory changes occur, these characteristically appear directly in the painful area and can be either negative (hypesthesia and hypoalgesia) or positive (allodynia and hyperalgesia) or both. Hence the old name ‘anaesthesia dolorosa’ describing persistent pain following (surgical) nerve damage (39). Trigeminal neuropathic pain is persistent and dull/pressing, superimposed neuralgic pain paroxysms may occur but these are not the predominant pain type (5). Probably the best-known sub-form of trigeminal neuropathic pain is postherpetic neuralgia which is, due to the pathognomonic efflorescence in the distribution of one or more branches of the trigeminal nerve, usually easy to diagnose and consequently treated by neurologists or pain therapists (40). The clinical picture of neuropathic pain and PIFP is nearly identical although the pain character in neuropathic pain is more often described as ‘burning’ (3). It seems that in most cases PIFP ceases at night (3) and this may be an additional discrepancy between these two conditions. Additionally, the pain location of PIFP may shift over the years and even cross to the other side, which is per definition not seen in neuropathic pain since the latter is elicited by a damage of the affected peripheral nerve. As the present review focuses on the lesser-known orofacial pain syndromes, we refer to an excellent and exhaustive review on neuropathic pain that has recently been published (40,41).
Persistent idiopathic facial pain (PIFP)
Clinical relevance
PIFP is underdiagnosed and undertreated and since it is a distinct trigeminal pain entity that responds to neuropathic pain treatment, dentists will refer patients to neurologists, pain doctors or general practitioners who need to recognize the syndrome.
Persistent idiopathic facial pain, formerly called atypical facial pain, is defined as a constant facial pain with a dull, aching or nagging quality, poorly localized and not following the distribution of a specific branch of the trigeminal nerve (5). Patients do not describe a neuralgiform, sharp-shooting pain component. Maximum pain intensity is described mostly over the cheekbone and the upper jaw. Most PIFP patients describe a subjective swelling over the affected region, attributed to central mismatch or perceptual distortion (42). While initially the pain is unilateral, with increasing duration it may cross the midline. Clinical and radiographic examinations in PIFP patients are normal and do not show local causes (5). If the pain is localized exclusively to a dentoalveolar site such as teeth and dentoalveolar bone, it is classified as persistent idiopathic dentoalveolar pain (PIDAP) (5), formerly atypical odontalgia (see Table 2).
Clinical characteristics of persistent non-dental facial pain and treatment options.

*Since these syndromes are rather rare, there is no consensus regarding treatment as evidence is limited to case reports/series.
It can be difficult to distinguish PIFP from painful post-traumatic trigeminal neuropathy (1). Many patients with persistent orofacial pain report a dental intervention or trauma around the time of pain onset. The key question is whether the orofacial pain is result of dental pathosis or not. Unfortunately, patients frequently have difficulties in reconstructing the sequence of events. The resulting difficulty in disentangling the causality of the orofacial pain and the fact that these patients primarily consult dentists (43) lead to root-canal treatment or extraction of healthy teeth, even though tooth extractions (i.e., a denervation of the dental nerve fibers in this context) carry a high risk of aggravating the situation further (3) (see Figure 2). The combination of constant pain without objective findings frequently leads to the incorrect suggestion that the condition is the mere expression of a psychosomatic disorder which adds weight to the psychological burden. This situation is reminiscent of that of a migraine patient 30 years ago (44). As a result, patients frequently move from specialist to specialist without receiving adequate diagnosis or treatment (43).

Model of a patient journey with chronic orofacial pain. The clinical picture of chronic non-dental facial pain is in many cases similar to pain due to dental causes. If the pain has a dental origin, dental intervention will be highly effective. If the pain has no dental origin, most of these patients undergo invasive procedures anyway in the hope of finding an occult dental cause (2).. If this is still not effective a craniomandibular disorder is suspected and the patients are prescribed with occlusal splints (43) or the neighboring teeth are operated on. If this is not effective a psychopathological cause is often suspected, and the patient may be frustrated and consults another dentist, and the circle starts again. Most patients with PIFP lose several teeth because of the disease (43).
The underlying cause of PIFP remains unclear. Considering that the pain does not follow the distribution of a specific branch of the trigeminal nerve, and that it can cross the midline, dysfunctional pain processing within the central nervous system seems more likely than a purely peripheral mechanism of action (45,46). The clinical characteristics of PIFP and PIDAP are consistent with the recently introduced pain category: nociplastic pain, for which the underlying mechanisms are not completely understood but include an augmented pain response characterized by centrally altered sensory processing and pain modulation, appearing either in solitude or as a mixed-pain state also involving components of nociceptive and neuropathic pain (47). Part of the clinical picture is multifocal pain; co-morbidity between chronic pains is frequent. In line with this, PIDAP was recently proposed to be a chronic overlapping pain condition (COPC) (48) although this attribution needs more clinical data. In this context it should be considered that the inconclusive electrophysiological results may also result from the limited field testing of the ICOP criteria as it may be the case that different pathologies lead to the same clinical phenotype.
Treatment
For the treatment of PIFP there are currently no randomized controlled trials (RCTs). As a result, pharmacological treatment very much resembles the treatment of neuropathic pain, which has been recently described in an extensive review (40). In short, the main pharmacological strategy involves antidepressants such as amitriptyline (10–150 mg), duloxetine (60 mg) or doxepin (10–150 mg), anticonvulsants such as gabapentin (1200–3600 mg), pregabalin (150–300 mg), or combinations. As in other pain syndromes, when combining different medications, it is important to use different mechanisms of action (e.g., not combining two sodium-channel blockers but rather a sodium- with a calcium-channel blocker or a tricyclic) to achieve the highest possible synergistic effect. Evidence for any of the treatments is limited, and randomized clinical trials are missing. Therefore, a conservative, multidisciplinary approach based on experiences with comparable chronic headache disorders including medications, relaxation training, psychological interventions and physiotherapy is recommended (2,49). A multidisciplinary biopsychosocial approach with the use of antidepressants and cognitive behavioral therapy offers the opportunity for alleviating pain and enhancing quality of life (50).
Burning mouth syndrome (BMS)
Clinical relevance
When intraoral causes of a burning sensation in the mouth are excluded, such patients need to be seen by general practitioners to exclude other secondary causes and confirm the diagnosis of BMS. Treatment of BMS is empirical and the first line treatment at this moment includes intraoral clonazepam or capsaicin and cognitive behavioral therapy.
Patients with BMS complain of superficial burning pain or discomfort most frequently from the tip to bilateral border of the tongue followed by the lower lip mucosa and the hard palate (5). Frequently accompanying complaints include xerostomia, dysgeusia and exaggerated response to hot and spicy food and drinks. Patients often report pain relief during meals and gum chewing. There is a strong gender predilection to women in peri- and postmenopausal state and a high preponderance of psychosocial comorbidities, similar to other chronic pain conditions (51). The pathophysiological background is unclear, and some reports have suggested abnormality in somatosensory function and reflexes (52,53) and small fiber atrophy in the tongue specimen of BMS patients (54,55). However, the pathology of this syndrome that mimics a neuropathic condition has not been elucidated. Dysfunction of the pain modulating system has been reported in psychophysical and imaging studies (56). The burning sensation in the oral mucosa can be classified as either primary BMS or as secondary to a wide array of oral conditions (such as lichen planus, oral candidiasis, metal allergy etc.) and nutritional deficiencies (such as zinc, vitamin B12, folic acid etc.) (56).
Treatment
RCTs on topical clonazepam and capsaicin, cognitive behavior therapy and laser therapy demonstrated favorable outcome in both short- and long-term assessment although the evidence level remains low. Clonazepam (57) is used as 0.5 mg two or three times daily and the patient is instructed to suck the tablets for 1–2 minutes and then expectorate the remaining saliva (56,58). This should be repeated every day for two weeks. Clonazepam probably acts locally in disrupting the mechanisms underlying stomatodynia, since there is a low systemic uptake for a two-week protocol (57). Capsaicin solution has been tested in randomized double-blind studies with a 0.01%–0.025% capsaicin solution for eight days (59) and 14 days (60) and 250 mg of chili powder emulsified in 50 ml water with a dose concentration of 3.54 µg/ml capsaicin (56,61). It should be emphasized that at present, there is no known curative treatment for BMS as the etiology remains uncertain. An exhaustive review of the literature regarding treatment has recently been published (56).
Other differential diagnostically relevant orofacial pain conditions encountered by clinicians
Dental (odontogenic) pain
Clinical relevance
Pain originating from the teeth is the most common secondary orofacial pain. It is exclusively treated by dentists but radiating and referred pain is common. Chronic forms with occult morphological causes (such as a cracked tooth) may mimic PIFP or more likely PIDAP (see above) and it is mentioned here for the purpose of differential diagnosis (see also Table 3).
Clinical characteristics of differential diagnostically relevant orofacial pain conditions encountered by neurologists and treatment options.

ICOP defined dental pain as ‘pain caused by lesions or disorders affecting one or more teeth and/or their immediately surrounding and supporting structures: the tooth pulp, periodontium and gingivae’ (5). Commonly known as toothache, the most common cause is dental caries and its sequelae which, depending on geographic location and socio-economic factors, may be highly prevalent. Referred pain is frequent; pain caused by a dental problem often spreads or radiates to other areas of the face and head (62,63). Hence, dental disease can present with pain in the face, ears, or jaw muscles (62). As a general rule, when the orofacial pain is described as dull localized pain which is intensified on provocation (such as chewing or percussion), usually the pain has a dental or possibly jaw muscular origin and needs to be treated by dentists. The exception to this presentation is painful pulpitis; sharp, intense and intermittent pain lasting seconds to hours, often elicited by changes of temperature (hot/cold drinks or food) and interspersed by pain free periods. If the pain-inducing disorder goes untreated or ineffectively treated, for example due to dental anxiety, acute pain may persist or recur, and eventually become chronic.
Sinus pain associated with rhinosinusitis
Clinical relevance
The most common cause for facial pain that becomes a frontal headache when increasing abdominal pressure is acute or chronic rhinosinusitis. However, this finding overlaps with migraine, which is an important differential diagnosis suggested to be the true diagnosis in 80–90% of cases of pain suspected to be caused by a sinus disorder (64,65).
Rhinosinusitis is most frequently caused by a viral and sometimes a bacterial infection, but also may have traumatic, chemical or iatrogenic causes and may be acute (signs and symptoms lasting <12 weeks) and chronic (lasting >12 weeks) (66). Chronic rhinosinusitis is generally considered multifactorial. The close anatomic relationship between maxillary posterior teeth and the maxillary sinus underlies up to 20% of acute cases, termed odontogenic sinusitis. The patient with acute rhinosinusitis commonly presents with facial pain and/or headache, often accompanied by other symptoms, e.g., nasal congestion, purulent nasal drainage, and hyposmia or anosmia. Local pain in the sinus area is frequent (67). Teeth in the posterior upper jaw can become tender on chewing and percussion (allodynia/hyperalgesia) and a primary dental cause may be necessary to exclude.
Salivary gland pain
Clinical relevance
In addition to dental pain and TMD pain, orofacial pain associated with eating or even thinking of food is most likely due to a disease of the salivatory glands.
Pain originating from the salivary glands is mainly categorized as being due to obstruction of the salivary ducts, bacterial or viral infection (sialadenitis), recurrent juvenile parotitis, immunologically mediated disorder, or other causes (5). The pain is usually intermittent, moderate to severe in intensity, and may be associated with swelling and pain to palpation of the affected gland in cases with superimposed sialadenitis. Salivary flow is either reduced or completely abolished, and pain and swelling may appear or increase in situations with increased salivary production, e.g., when starting a meal, thinking about food, or citric stimulation applied to the tongue. Removing the cause of salivary duct obstruction is associated with a good prognosis for pain relief.
Inflammation of the salivary glands may be acute or chronic and may be associated with inflammatory pain, swelling and redness. Acute sialadenitis may be caused by viral (such as mumps, coxsackie, or cytomegalovirus) or bacterial infection, most often with staphylococcus aureus leading to acute suppurative sialadenitis (68). Most viral infections are self-limiting, and treatment includes symptom management, whereas bacterial infection requires antibiotics.
Painful temporomandibular disorders
Clinical relevance
Since the prevalence of TMD is high, it is rather likely that headache patients may have a TMD as well. Although TMD is not causal for a primary headache, the constant input into the trigeminal system may well trigger or worsen a primary headache and treatment of TMD may reduce headache for this reason.
Temporomandibular disorder (TMD) is an umbrella term for a group of musculoskeletal conditions involving pain and/or dysfunction in the masticatory muscles, temporomandibular joints (TMJ) and associated structures. The three major signs and symptoms are pain, limited range of motion, and jaw movement sounds. The pain in the preauricular area is described as aching, pressing and tender with spreading and referral to the face, ear, temple, and teeth. The pain does not have a paroxysmal component and no associated autonomic features are noted. There is an ongoing discussion on the clinical importance on differentiating between jaw muscle and TMJ types of TMD pain and although there may be similar mechanisms and common traits of vulnerability at play, it may still be premature to confine all types of TMD pain into one (69). The frequency may vary from a few infrequent episodes to more frequent and even chronic types probably forming a continuum such as the one observed for tension-type headaches (5). The current diagnostic criteria for TMD (DC/TMD) distinguish between muscle disorders (myalgia and myofascial pain), TMJ disorders (arthralgia, disc displacements, degenerative joint diseases and dislocation) and headache attributed to TMD (5,70). Whereas clicking sounds and crepitations during jaw movement may be asymptomatic with no need for management, pain and limitations in jaw movement often demand treatment from a dentist or OFP specialist (71). TMD pains are also often associated with psychosocial and emotional distress and reduced quality of life (72).
Bruxism
Clinical relevance
Bruxism as such is not a pain disease. Self-reported bruxism is nearly always associated with painful TMD and also an exacerbation of pre-existing primary headache. Myofascial pain due to bruxism can be clinically indistinguishable from tension-type type headache but needs a different treatment concept. Therefore, bruxism, and particularly day-time bruxism should be recognized.
Bruxism is defined as a repetitive jaw-muscle activity that is characterized by clenching or grinding of the teeth and/or by bracing or thrusting the mandible and occurs during sleep (sleep bruxism) or during wakefulness (awake bruxism) (73). Self-reported bruxism is associated with TMD pain in many epidemiological studies, however, bruxism assessed with more stringent criteria, i.e., electromyographic recordings have failed to show a linear relationship to TMD pains (74). Recent evidence suggests that sleep bruxism may be a natural behavior in most individuals and help with airway patency and salivary secretion during sleep (75). Headache may be more related to awake bruxism and is clinically indistinguishable from tension-type headache (76). Sleep bruxism did not show any association with headache development, although the relationship is somewhat controversial (74). Patients with migraine may also suffer from bruxism and in this case bruxism is not the cause but may act as a trigger (77). Removing or reducing the trigger using physical strategies (e.g., stretching, relaxation, oral splints) may help reducing the frequency of migraine attacks and can protect the dentition from excessive wear but interestingly does not reduce the jaw muscle activity in the long-term perspective. A recent systematic review suggested that oral splints have no significant effect on pain in TMD or bruxism (78). Local application of botulinum toxin into the masseter and/or temporalis muscles may be an effective alternative (79,80).
Conclusion and expert outlook
The recent publication of ICOP will act as a catalyst to advance the orofacial pain field in the same way ICHD revolutionized the understanding of headache disorders. Just like in ICHD, the ICOP is subject to the evidence-based process of disease classification and will change when field testing suggests that such changes are necessary. Functional neuroimaging and neurophysiological studies of the newly defined disorders will play an essential role in this endeavor and may – just like in headache disorders (81,82) shed some light on the underlying mechanisms of orofacial pain disorders (83). Likewise, the establishment of adequate animal models is urgently needed to investigate molecular pathways that may explain the different susceptibility to the different pain-alleviating pharmacological strategies compared to other trigeminally mediated pain syndromes (e.g., migraine) or even non-trigeminal pain.
Triptans are so-called headache specific medications since they are ineffective in somatic pain (84). Whether they have any effect in orofacial pain syndromes remains unknown because of a lack of appropriate clinical trials. Equally, treatments targeting the calcitonin gene-related peptide (CGRP) pathway are emerging treatment options in migraine and CH (85), but their effect in orofacial pain needs investigating. Such studies will not only expand our therapeutic armamentarium for these syndromes, but beyond that provides valuable new insight into our understanding of the underlying disease mechanisms. Ultimately this will lay the foundation for the development of novel and currently unknown treatment possibilities. Just like in headache it is important that pain specialists and neurologists engage and adopt orofacial pain diagnoses and treatments and thus shape the future of these patients.
Article highlights
Just like for headache, an internationally accepted classification system for facial pain (ICOP) has been published. Three broad groups of orofacial pain patients are important for clinicians: attack-like orofacial pain conditions, persistent orofacial pain disorders, and differential diagnostically relevant orofacial pain conditions. It is rewarding to know and recognize the clinical picture of these facial pain syndromes, as they can increasingly be treated.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JH has received honoraria for consulting and/or serving on advisory boards as well as for speaking from Allergan, Autonomic Technologies Inc. (ATI), Cannovex BV, Chordate Medical AB, Eli Lilly, Hormosan Pharma, Lundbeck, Novartis, Sanofi and Teva. He receives research support from Bristol Myers Squibb. He received personal fees for Medico-Legal Work as well as from Oxford University Press, Quintessence Publishing, Sage Publishing and Springer Healthcare. All these activities are unrelated to the submitted work.
LBH, MP, PS, and YI have nothing to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.