
Abstract
Objectives:
To qualitatively identify evidence-based literature related to the daily burden and unmet treatment and psychosocial needs of patients with cluster headache (CH).
Methods:
A literature search was conducted through October 20, 2020 across MEDLINE, EMBASE, CINAHL, and PsychInfo databases exploring quality of life (QoL) and disease burden in adults with CH. The search was restricted to full-text reports in peer-reviewed journals. Methodologic quality was assessed using the Critical Skills Appraisal Program.
Results:
From 11 identified publications, QoL was reduced in persons living with CH, with significant psychological, social, and socio-economic burdens, and work-related disability. The CH disease trajectory is complex, with patients experiencing the impact of their disease across multiple domains beyond the biological manifestation of the disease including stigma, employment limitations, and suicidal ideation, and with a lack of effective treatment from the patient perspective.
Discussion:
These findings strengthen comprehension of the CH patient experience, enabling a deeper understanding of the patients’ perspective and experience of their disease andunmet needs, providing a basis for future research into this debilitating condition. Minor limitations of this study include data extraction and study selection biases.
Introduction
Cluster headache, a trigeminal autonomic cephalalgia, is a primary headache disorder characterized by severe, strictly unilateral headache attacks accompanied by ipsilateral autonomic features with or without a sense of restlessness or agitation. 1 Each headache attack is relatively short (enduring for between 15–180 minutes), but can occur as often as eight times per day during the active phase. 1 It is described as one of the most intensely painful human conditions, characterized as sharp and burning, and patients with cluster headache have rated the pain as significantly more painful than childbirth, kidney stones, gunshot wounds, and migraine. 2 In addition to the headache pain, patients suffering cluster headache report additional autonomic symptoms, including lacrimation, ptosis, conjunctival redness, and eyelid edema, with or without a sense of restlessness or agitation. 1,2 Cluster headache can arise de novo in an episodic or chronic pattern, and both can evolve into the other. 1 In the more common episodic form (85%–90% of patients), the cluster of attacks (referred to as cluster periods) are separated by pain-free remission periods of greater than 3 months. The chronic form occurs without remission periods or with remission periods of less than 3 months. 1,3 Notably, pain intensity is not associated with episodic or chronic cluster headache status. 2
Cluster headache is estimated to affect 0.1% of the worldwide population. 3,4 However, given its low prevalence, the true incidence, distribution, and burden of cluster headache is generally unknown. This results in a limited understanding of the triggers and temporal course of the condition. 3,5 Variability in the clinical presentation, 6 misdiagnosis of symptoms as being migraine-related, 7 and the lack of understanding and awareness, 8 particularly among primary care physicians, contribute to diagnostic delays of several years for most patients with cluster headache. 7,9 A recent study identified that up to 50% of patients were diagnosed with cluster headache by a neurologist, indicating that misdiagnosis or inappropriate treatment may have come from other specialists or self-diagnosis. 10,11
Treatment for cluster headache can be divided into three categories, including: abortive treatment with subcutaneous sumatriptan or oxygen therapy to halt ongoing attacks; transitional treatment with options such as oral corticosteroids to temporarily reduce the severity and/or frequency of attacks; and preventive treatment with therapies such as verapamil and lithium to decrease the frequency of attacks as well as to prolong the interval between attacks. 12 Emerging treatment options include calcitonin gene-related peptide antagonists, non-invasive vagus nerve stimulation, and sphenopalatine ganglion stimulation. 12,13
In line with the greater severity of pain reported by patients with cluster headache when compared with other primary headache disorders, 2 the corresponding quality of life (QoL) of affected individuals is lower. 14 Cluster headache has been associated with significant psychologic, social, and socio-economic burden; work-related disability; and a high rate of suicidal ideation during attacks. 14,15 Patients report an inability to access safe and effective treatment both in the short-term and across their lifetime, which adds to the burden of this condition. 12,16 –21
Preventive treatments, such as verapamil and lithium, are associated with short- and long-term adverse effects and require regular, close monitoring such as electrocardiography (ECG) and blood testing. 18 Transitional treatment options, such as oral corticosteroids, are limited to short-term use because chronic use is associated with hypertension, osteoporosis, cataracts and type 2 diabetes. 20 During headache-free periods, patients also report increased anxiety related to future attacks. 22,23
The paucity of evidential data relating to cluster headache is particularly notable in relation to patient-reported outcomes (PROs). Despite the recent development and validation of specific PRO scales for cluster headache, 23,24 it is apparent that the widespread uptake and administration of these measures within clinical practice and/or research have not occurred. While detailed qualitative data are now available to explore the experiences of individuals living with migraine, 25,26 similar research is not available for cluster headache 14 ; this lack of information is a disadvantage both to healthcare practitioners and to patients when deciding on optimal management for this disorder.
As such, we undertook an evidence-based analysis to systematically identify the body of qualitative literature related to the burden and unmet needs of patients with cluster headache. We anticipate that the resultant findings will strengthen our comprehension of the patient experience of cluster headache, enabling a deeper understanding of the patient’s perspective on the holistic impact and burden of living with cluster headache.
Methods
Data sources
This was a qualitative, evidence-based literature analysis, conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 27 ) guidelines. A comprehensive literature search was conducted across the MEDLINE, EMBASE, CINAHL, and PsychInfo databases, from inception to October 20, 2020. The MEDLINE search string is provided in Table 1.
MEDLINE search string in ProQuest format.
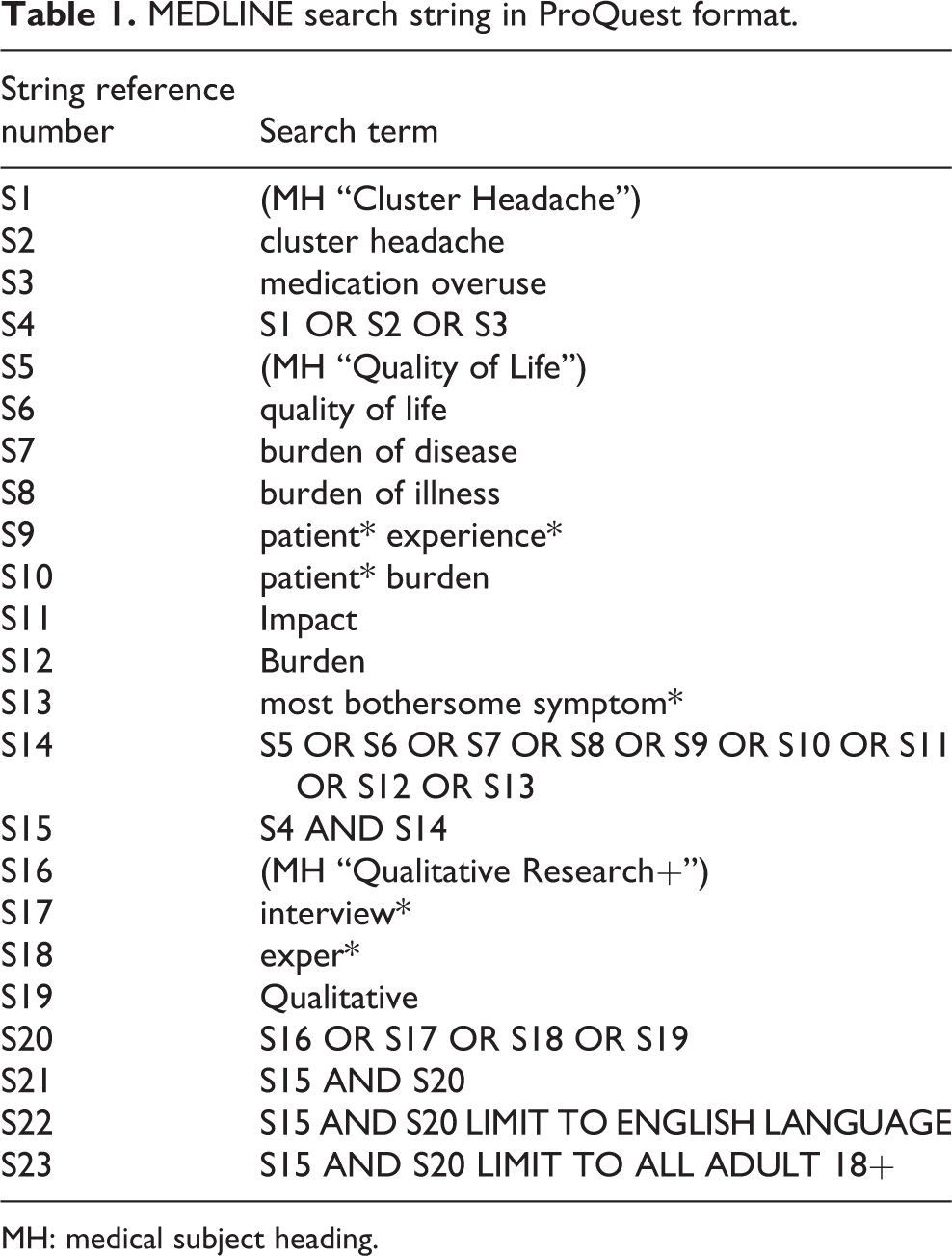
MH: medical subject heading.
Articles exploring QoL and burden of disease for adult patients with cluster headache, in any language, were eligible with the requirement for an English-language abstract. The article types were restricted to full-text reports published in peer-reviewed journals; any letters, abstracts, and conference reports were excluded. Reference tracking of any identified systematic literature reviews was performed to ensure comprehensive retrieval of articles.
Inclusion/exclusion criteria
The definition of cluster headache was based on the International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria. 1 Studies were included for patients who reported at least five attacks with unilateral temporal or periorbital pain, lasting 15–180 minutes, with or without autonomic symptoms, a frequency between one every other day to up to eight episodes per day, as well as patients with episodic (attacks occurring in periods lasting from 7 days to 1 year, separated by pain-free periods lasting at least 3 months) or chronic disease (attacks occurring for 1 year or longer without remission, or with remission periods lasting less than 3 months). Of note, the definitions of episodic and chronic cluster headache changed with introduction of ICHD-3 in 2018, with prior editions having different classifications of episodic and chronic disease based on the timeframe of the remission periods. Therefore, the definition of cluster headache in studies prior to 2018 does not reflect the current definition. Studies that included patients with migraine, migraine symptoms, or other primary headache disorders were excluded.
The burden of cluster headache on patient QoL was broadly defined. Studies were included if they examined any aspect of a patient’s work-life, social-life, education, activities, emotions, mental health, physical abilities, or experience of symptoms. Articles exploring population or macro-financial aspects related to the national economy, healthcare systems, or direct/indirect costs to the society were excluded; reports describing the micro-financial issues and direct economic costs that faced affected patients with cluster headache were included. Research investigating the development of cluster headache PROs were included if they satisfied the other inclusion criteria.
Data extraction
The identified studies were screened for eligibility (DR and RC), with inclusion and exclusion agreed on by consensus after discussion. Patient-based data were then extracted from the included studies. A critical appraisal of the articles identified was also conducted (DR and RC). Methodologic quality was assessed using the Critical Skills Appraisal Program (CASP) domains of aims, design, recruitment, data collection methods, potential bias, data analytic rigor, ethics, findings, research value, and overall quality. 28 The CASP tool, a commonly used checklist/criteria-based tool for quality appraisal in healthcare evidence syntheses, appraises the strengths and limitations of qualitative research methodology. It comprises 10 questions that ask the researcher whether the methodology was appropriate and if the findings were meaningful (see Online Supplemental Material: Table 1). Quantitative economic studies were assessed using the Centre for Evidence-Based Medicine (CEBM) critical appraisal checklist. 29 Although studies were not excluded on the grounds of quality, the results of these assessments were used during the process of weighing research findings, particularly in cases where evidence was contradictory.
Data synthesis
Data were analyzed using a blended qualitative-synthesis approach, using both inductive thematic synthesis and deductive framework synthesis approaches. 30 The preliminary conceptual framework was informed by two standard health and disability measures: the World Health Organization Disability Assessment Schedule 2.0 31 and the 36-item Short-Form health survey. 32 Both have been widely applied across a range of diseases, populations, and cultures. The conceptual model was also informed by the two studies reporting development and validation of PROs for cluster headache. 23,24 Finally, the authors reviewed the current criteria for diagnosis of cluster headache 1 and several quantitative studies in diverse geographic regions 9,33 –35 in order to inductively modify the framework by the addition of new themes. Data were extracted directly using Dedoose software (Dedoose, Hermona Beach, CA, USA), and coded (DR and RC) according to the modified conceptual framework.
Results
Study selection
A total of 645 records were identified via initial database searching, 127 of which were subsequently found to be duplicates. The remaining 518 records were screened for initial eligibility, resulting in the exclusion of 484 that did not meet the inclusion criteria. Of the 34 full-text articles that were screened, 8 met the eligibility criteria, with a further 3 studies added following citation analysis. In total, 11 publications met the overall evidence-based literature search criteria (Figure 1).
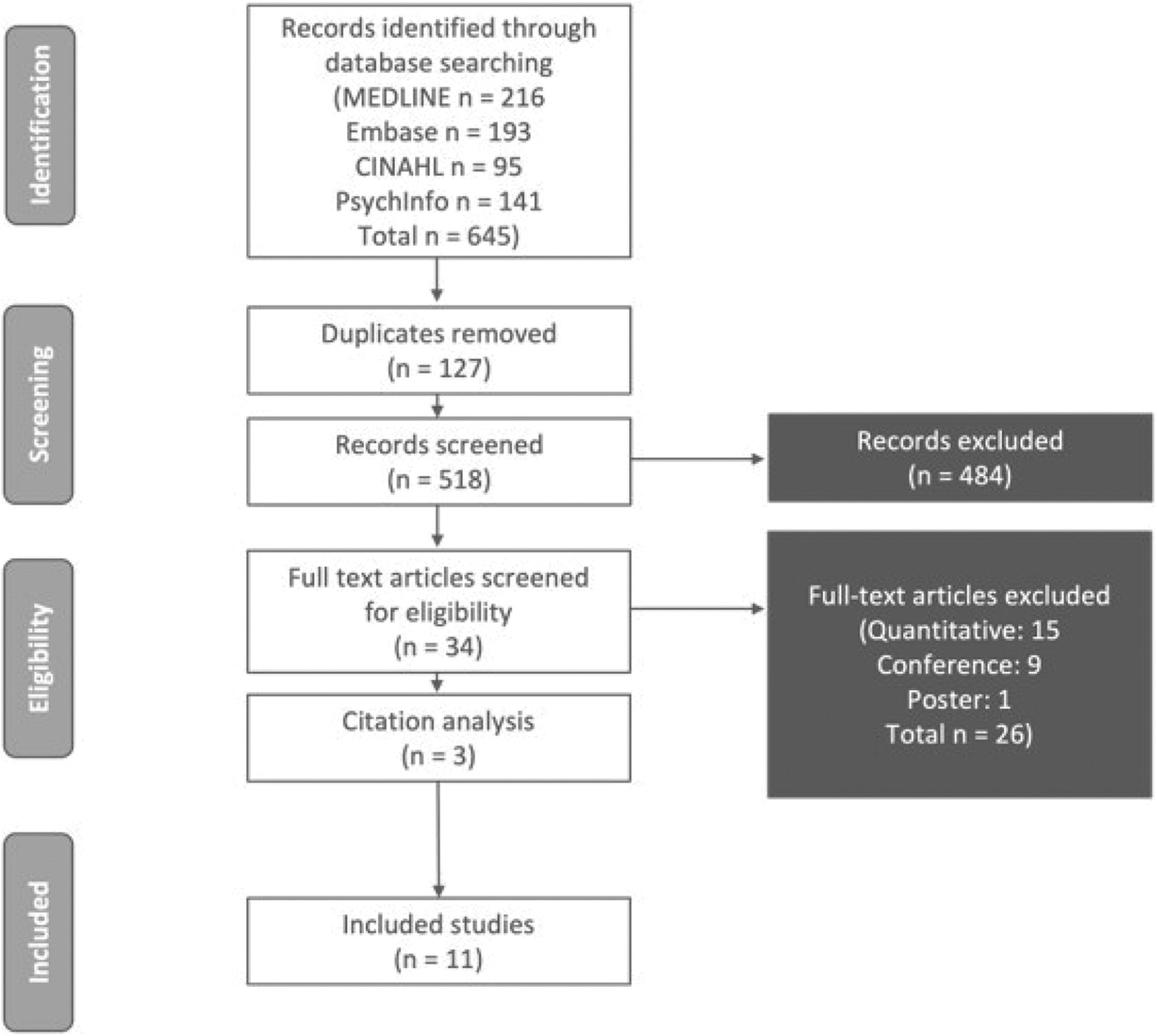
PRISMA flowchart.
Study characteristics and data quality
Table 2 summarizes the characteristics and content of the 11 identified studies included in the analysis. The earliest article was published in 1995, with most studies (7/11) published within the past 5 years (i.e., 2016–2020), indicating a recent growth in interest regarding cluster headache.
Summary of study characteristics.
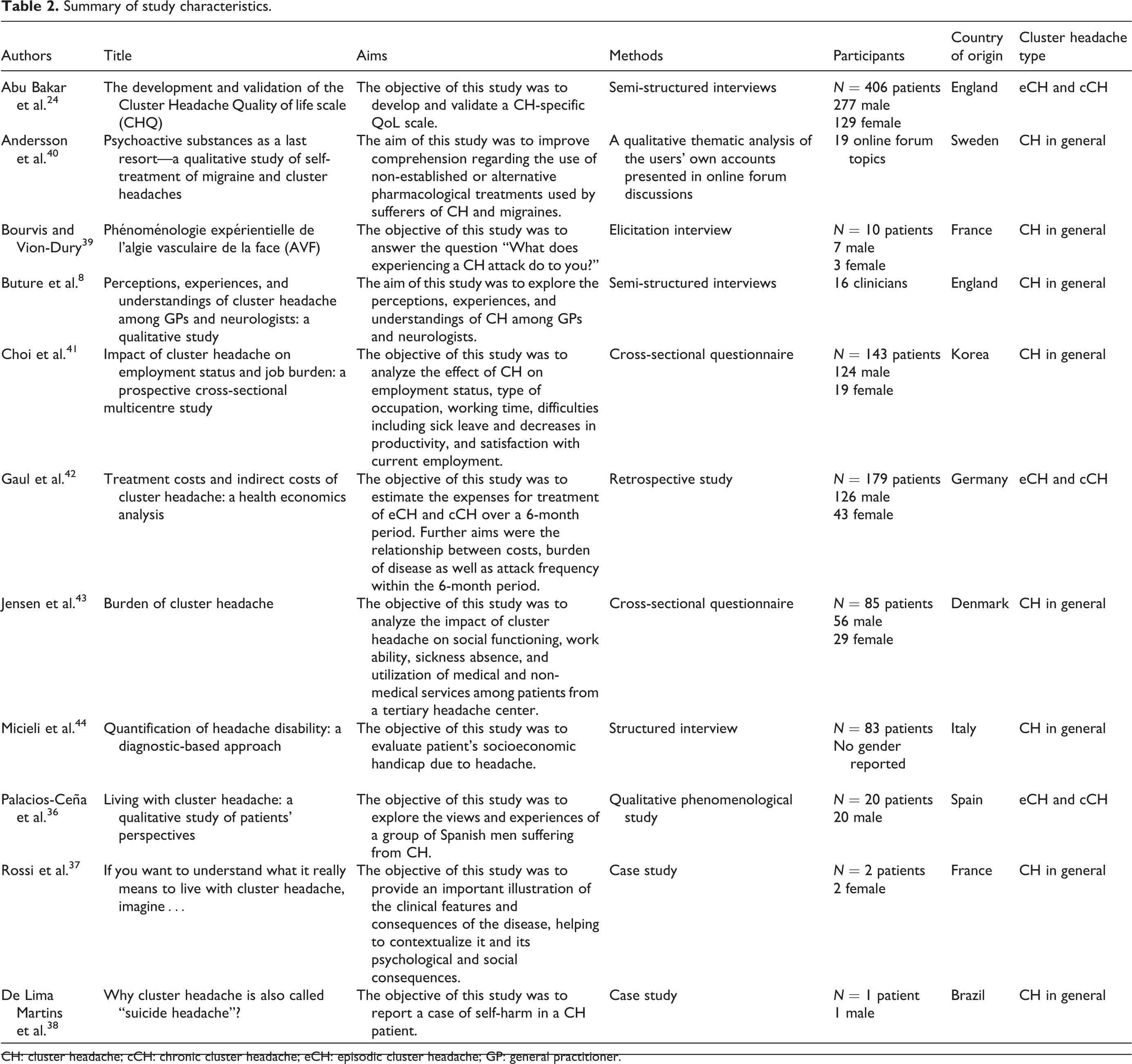
CH: cluster headache; cCH: chronic cluster headache; eCH: episodic cluster headache; GP: general practitioner.
Quality assessment, utilizing the CASP framework, concluded that the identified studies were from different methodological backgrounds (including interviews, questionnaires, case studies, and a retrospective economic analysis) and thus were not easily comparable. The purely qualitative papers contained some studies of high quality, employing a range of appropriate and well-justified research methods; in contrast, some offered limited methodological information. Although the studies by Buture et al. 8 and Palacios-Ceña et al. 36 provided detailed methodologic information (including recruitment, sampling, ethics, reflexivity, and saturation), other studies provided limited information 37 , or utilized data from a single patient. 38 It should, however, be noted that the study by Palacios-Ceña et al. 36 included only male participants from a single center in Spain, introducing potential bias into the resulting data. For other studies, full appraisal was challenging given the limitations of the standardized CASP framework. 24,39,40
Assessment of the four studies reporting the financial impact of cluster headache, 41 –44 using the CEBM checklist, suggested that the evidence from these studies were of reasonable to low quality. Although all four studies had relatively large populations (ranging from 83–179 patients) that may be representative samples, all used convenience sampling methods with no randomization and were at risk of self-reporting bias.
Descriptive analyses of the data
Descriptive analyses describe the burden of cluster headache on patients’ lives by drawing on the evidence found in the included studies. The results presented outline the burden of cluster headache across a comprehensive range of QoL and burden of disease measures.
Disease trajectory
This analysis addresses the overall experience of disease burden for a person with cluster headache, including diagnosis and treatment.
Diagnostic delay and misdiagnosis
For patients with cluster headache, obtaining an accurate diagnosis is an activity fraught with difficulty and often years of delay. Cluster headache is an uncommon condition, and many healthcare practitioners (HCPs) are unaware of or unfamiliar with the clinical symptoms associated with the disease, especially if presenting with non-traditional symptomatology. 8 General practitioners (GPs) and primary care physicians (PCPs) have admitted to not being confident in diagnosing cluster headache, while neurologists have pointed to insufficient and incomplete medical histories as a common source of misdiagnosis. 8 Furthermore, terminology can add to the confusion, with a lack of differentiation between “cluster headache” and “cluster migraine.” 8 For many GPs and PCPs, there may be an incorrect understanding of cluster headache as being “several attacks of headache close together,” whereas for neurologists, a correct and timely diagnosis may be delayed by the fact that the patient does not always present with clear textbook symptoms that are based on diagnostic criteria; this may also result from a lack of clinical awareness of mixed headache syndromes (in which a patient may have both cluster headache and another condition causing craniofacial pain). 8
Information obtained from this patient-focused literature analysis supports the view that HCPs, particularly general practitioners/primary care physicians, are often lacking in their knowledge regarding the symptomatology and accurate diagnosis of cluster headache, and that misdiagnosis is common. 36,37 Unilateral headaches—a key characteristic of cluster headache—are generally assumed to be due to migraine, with migraine being the most common misdiagnosis of cluster headache. 8
Misdiagnosis is of great clinical concern, not only because it can delay appropriate treatment, but because it may also result in unnecessary medical procedures and treatments, leading to unnecessary direct and indirect healthcare utilization costs. HCPs have reported that patients have undergone sinus washouts and tooth extraction in an attempt to alleviate pain associated with cluster headache. 8 Some have even gone in search of potential pain relief outside the healthcare system and approved therapeutic agents, including turning to illicit substances in an attempt to reduce symptoms. 40 The unmet needs arising from the misdiagnosis of cluster headache, as well as delays in diagnosis and treatment, commonly lead patients to practices and activities that result in high healthcare resource utilization. This includes consultation with multiple physicians (often independent to, and unaware of, each another) to manage their disease, as well as visit(s) to the emergency room and after-hours care centers seeking immediate relief from headache pain. Patients have received CTs, EECs, cervical spine X-rays, and skull X-rays to diagnose the source of pain. 7 One study reported that despite having previously consulted with a GP, cluster headache patients in Denmark were found to have a significantly higher frequency of visits to specialists and off-hours services (GP on off-hour duty or hospital emergency department) compared with the general population. 43 In addition to adding to indirect healthcare utilization costs, these secondary referrals can result in unclear responsibilities for care, with confusing guidelines complicating treatment coordination and communication. This creates contentious relationships between primary and secondary care clinicians, as well as between patient and primary clinician, where the patient may have received conflicting advice from the secondary care clinician. 8 For some patients with cluster headache, the introduction of a new (or additional) healthcare professional is welcomed and may be viewed as an opportunity to try new procedures or treatments. 8,36 For other patients, a secondary (GP or emergency room clinician) or specialist (pain specialist, neurologist) referral is internalized and viewed as unsettling, becoming a source of added stress and anxiety, and is often viewed as “going back to square one” in providing headache symptomatology and medical history. 36,37
Connected to these diagnostic issues, people with cluster headache often report feeling unsupported. The available studies evaluating cluster headache highlight patients reporting a common theme that their HCPs express a lack of empathy, as well as a perceived minimization of the severity of pain associated with cluster headache, and even accusations of malingering or psychologic disturbance. 36 –38 For patients with cluster headache, the pain is unparalleled, and they want to be believed; they seek to be understood and to receive an acknowledgment that their condition is not comparable with a migraine or hangover. 36 When they feel their needs are unmet by their HCP or they feel that the patient-physician interaction was unconstructive, patients with cluster headache frequently turn to the internet for online advice and empathy. 36,40 However, patients who distrust their GP and desire additional reassurance may also insist on secondary referrals and unnecessary procedures, such as frequent MRIs, 8 continuing the cycle of diagnostic delay, multiple consultations, stress, anxiety, healthcare utilization, and reduced QoL.
Cluster headache has been traditionally viewed as a chronic disease with a high male preponderance, with literature-based estimates of the male-to-female ratio ranging from 1.9:1 45 to 9.6:1. 46 The identified studies in this evidence-based review highlighted this issue. Palacios-Ceña et al. 36 chose an all-male sample for their study, which explored the experiences of people living with cluster headache, justified by the perceived predominance of males living with the disease. The studies by Gaul et al., 42 Jensen et al., 43 and Rossi et al. 37 had study populations more closely representative (2 to 3:1); however, in the study by Choi et al., 41 the ratio was 6.5:1. Both Palacios-Ceña et al. and Choi et al. acknowledge the limitations of having men overrepresented in their samples. Although scientific literature has highlighted this inconsistency and real-world evidence suggests a male-to-female ratio ranging from 3:2 to 1:1, 47,48 recent interventional clinical studies not included in this evidence-based review still demonstrate male-to-female ratios ranging from 3:2 49,50 to ∼4 to 6:1. 51,52 Further, the authors could not identify qualitative experiential data that were definitively linked to female patients. However, a higher rate of misdiagnosis has been reported in women, with migraine as the most common incorrect diagnosis. 53 Additionally, while ethnicity was not reported in the included studies, differences in the gender ratio and symptomology of cluster headache patients may vary based on the country where a patient resides. For example, a narrative review by Peng et al. 54 highlighted that patients with cluster headache in Asian populations showed a stronger male predominance compared to European and North American populations. The true gender ratio remains unclear and additional research into the true incidence rates of cluster headache is warranted to assist in appropriate diagnosis.
Medical treatment
Once diagnosed, patients with cluster headache often describe that some conventional abortive treatments, as well as preventive medical treatments designed to reduce the frequency of attacks, have little to no efficacy. 40 They feel the treatments they are provided are futile, and are skeptical of any prescribed medication even before they have taken it. 36 Trying different forms of treatment with little to no success produces increased feelings of sadness, despair, and hopelessness. 36,40 This is emphasized by the aforementioned distrust of HCPs stemming from a perceived lack of empathy, furthering the doubts about the efficacy and safety of any prescribed medication. 36
The inability to obtain an effective treatment for cluster headache appears to have multiple causes. The cost of medication is one issue for HCPs to address with cluster headache patients, as is a lack of awareness of how to obtain recommended treatments, such as oxygen administration. 8 The need for referrals in many healthcare systems can also complicate patients’ access to an effective treatment, because certain treatments can only be initiated by specialist healthcare practitioners. 8 Complicating this inability to obtain treatment is the lack of knowledge on the part of the patients themselves; one study indicated that 95% of patients with cluster headache were ill-informed about their condition, 36% lacked information about available treatment, and 29% were unaware of possible adverse effects. 36 Treatment hesitancy may also play a role; in addition to a lack of trust in the efficacy of treatment for cluster headache, patients worried about the concept of being bound to medication for life, or about the potential for addiction to pain medication. 36,40
Alternative and holistic therapies
When patients with cluster headache feel their HCPs are not helping them or when they do not fully understand the information they are given regarding their disease, they are likely to turn to online resources to gain information regarding treatment regimens and alternative therapies. 36,40 The regimens described by patients include lifestyle adaptations (exercise andnutrition), 40 and consultations or treatments with a range of healthcare providers (psychologists, physical therapists, chiropractors, traditional healers, and acupuncture specialists). 36,43 Patients reported that alternative therapies (i.e., vitamin supplements, melatonin, herbal remedies, and energy drinks with taurine or caffeine) had limited to no effect, 40 as did the use of illegal/illicit substances (i.e., psilocybin, lysergic acid diethylamide [LSD], dimethyltryptamine [DMT], cannabis, opium, ketamine, cocaine, lidocaine, and 3,4-methylenedioxymethamphetamine [MDMA]). 36,40 While psychedelic tryptamines such as psilocybin and LSD were anecdotally described as significantly lessening the frequency and intensity of the attacks of cluster headache, 40 usage also resulted in a temporary increase in pain or onset of new symptoms (such as sensory disturbances, anxiety/panic attacks, and perspiration) before any mitigating or preventive effect was observed. 40 The evidence for cannabis was conflicting, with some patients reporting positive impacts and others suggesting that use could possibly trigger attacks. 40 Despite the risks associated with sourcing illegal drugs and the possibility of harm resulting from mis-labeled, adulterated, and impure versions, or from overdosage, patients with cluster headache continued to access such treatments out of despair and desperation for adequate disease management. 40
Finally, coping strategies not involving the use of pharmacologic agents are frequently mentioned in the available studies. While most involve temperature, sound, and/or light adjustment (e.g., leaning against a cold window oragainst the refridgerator, wrapping their heads in cool towels, isolating in a dark room, and engaging in relaxation techniques) and are not harmful to the patient with cluster headache, 36 some patients have used pain (through self-harm) as a distraction technique, which can have devastating physical and psychological consequences. 38
Symptomatology
Pain
Intensity, frequency, and duration were found to be relevant categories for understanding the impact of pain in cluster headache.
The intensity of pain experienced during a cluster headache attack has been described by patients as excruciating, unbearable, paralyzing, and debilitating—with a level of pain that is independent of overall frequency of attacks. 36,40 Pain intensity is described as the “heart” of the cluster headache experience, 39 and has been likened to “a pile of red-hot metal [passing] through your skull,” “someone stabbing a knife in your eye and turning it for hours,” and “a pack of dogs with enormous fangs…tearing you inside your head, tearing off the flesh, crushing everything.” 37 In a study of patients with episodic or chronic cluster headache, participants were asked to rate the level of their pain on a scale from mild to excruciating, with 73.9% (300/406) reporting it to be excruciating, with no difference in pain intensity based on frequency of attacks. 24
The frequency of attacks of cluster headache is variable and can be unpredictable, ranging from once every other day to up to eight times per day. 1 In one study, the average frequency of attacks in 406 patients was found to be 3.5 cluster headache attacks per day. 24 One patient in the case study series described experiencing attacks three times a day. 38 In a separate study, patients reported up to eight attacks within 24 hours. 37
In terms of duration, patients have subjectively described the pain associated with cluster headache as being relentless and continuous. 36 Objectively, in a UK study of patients with cluster headache, the average duration of attacks was 46.5 minutes. 24 Bourvis and Vion-Dury, 39 in their study of French patients with cluster headache, claimed that the pain of the attack ended quite quickly and that there was subsequently an abrupt return to normal. The authors subsequently discussed the credibility of the diagnosis of cluster headache. This type of discussion further increases the stigma associated with cluster headache and raises the potential for further dissatisfaction between patients and their HCPs. Consistent across all the identified studies regarding the duration of cluster headache attacks was the considerable variation in disease presentation and patient symptomatology, which was noted by practice setting, location, and disease frequency.
Associated symptoms
The general published literature reports multiple symptoms associated with the pain of cluster headache; with autonomic symptoms such as facial sweating and lacrimation noted by the International Headache Society.
1
Although not recognized in the diagnostic criteria for Cluster Headache, there were multiple patient testimonials in relation to temperature, light, and sound sensitivity.
24,36,37
One patient said of a family member,
Psychiatric symptoms
Psychiatric co-morbidities are a common and significant concern in patients with cluster headache. Other studies not included in this analysis have shown that patients with cluster headache have a significantly higher lifetime risk of suicidal ideation when discussing treatment options, with chronic cluster headache patients at an even higher risk. 15,55 HCPs have indicated that patients are likely to experience psychiatric comorbidities such as depression, self-harm, psychosis, and suicidal ideation. 8 Patients reported that they often became angry 37 and anxious 40 during their interictal periods, worrying when their next attack would occur, how long its duration would be, and how severe the pain would be, 36,37,40,43 and these feelings have been likened to conditions such as post-traumatic stress disorder. 40 Patients also reported feeling disconnected and isolated from their friends and family, as well as frequently feeling like a burden, which resulted in further anxiety and stress regarding missing family outings and events. 24,37 In addition, patients reported an intense fear and heightened sense of anxiety over the unpredictability of their cluster headache, furthering the development and escalation of stress due to knowing that their current pain-free time was directly linked to their next cluster attack. 36,37,40,43
The likelihood of psychiatric symptoms in patients with cluster headache was confirmed by other studies included in this analysis. In these studies, patients with cluster headache have reported higher levels of anxiety, depression, and stress compared to patients with migraine or tension-type headaches. 24,41 Other data published after the timeline for this review have identified and discussed demoralization and suicidal ideation as key psychiatric symptoms of concern in patients with cluster headache, with higher overall risk of suicidal ideation in patients with cluster headache. 55
Demoralization, largely expressed in terms of lack of vitality and loss of identity, was a common theme throughout the studies evaluated. Although there was limited discussion around experiences of low energy and tiredness, one patient memorably described cluster headache as “life-sucking.” 36 Several authors also reported a loss of identity due to the intense pain, with patients feeling violated, empty, canceled, impotent, and helpless. 36,39 Life is reported to be slipping past while the disease rules their daily existence, 36,37 described as akin to living as “a prisoner in a straitjacket of suffering.” Lamentably, in this context, a lack of vitality, loss of identity, and overall demoralization directly connects to tendencies toward acts of self-harm, suicidal ideation, and suicidal behavior, which were frequently mentioned in these studies, and is cause for great concern for patients with cluster headache. 8,24,36 –38,40
Patients have expressed suicidal ideation at the inability to appropriately manage the pain and headache symptoms associated with cluster headache. 38 The severity and unrelenting nature of the pain associated with cluster headache is described as giving patients delirious thoughts, leaving them wanting to physically flee and run from their pain, and contributing to considerations of self-harm and suicide. 39 Indeed, patients with cluster headache often referred to their disease as having a “suicide headache.” 38 Ideation of jumping from a window to resolve feelings of despair appeared in three separate patient testimonials in the literature reviewed, 36,37,39 with one participant in an online forum discussion suggesting that suicide is the implicit prognosis for patients suffering from cluster headache. 40 In more recent studies not originally included in the literature review, patients with cluster headache were shown to have a significantly higher lifetime risk of active or passive suicidal ideation as compared with controls.
Triggers
Despite documented evidence for triggers for cluster headache attacks, such as alcohol consumption and sleep, triggers were only discussed in one of the identified studies. 56,57 The triggers that were noted included foods like chocolate and fermented cheese, physical or environmental changes (e.g., weather, drop in blood pressure, presence of carbon monoxide), and ingestion of substances like alcohol, cannabis, opiates, sumatriptan, and phenethylamines. 40
Physical, emotional, and cognitive functioning
There was limited discussion of physical functioning identified in this evidence-based literature review, though emotional and cognitive dysfunction have been described. The discussion of emotional functioning in the literature primarily focused on negative emotions that were clearly the result of pain and the direct experiences of how that pain interferes with daily life. The pain of the attacks may elicit feelings of rage or anger, 36,37,39 and this may manifest as hurtful/offensive words and angry gestures. 24,39 A second affective range of sorrow, grief, sadness, disappointment, and despair seemed more directly connected to the disease trajectory. 36,37 As previously noted, another common emotive experience among patients with CH (either episodic, chronic, or both) was intense fear and anxiety over the unpredictable nature of the attacks; waiting for the next debilitating attack to occur during their pain-free time was linked to comorbid anxiety and stress disorders. 36,37,40,43 Moreover, in addition to fearing the next attack, other patients feared their future prognosis, which was a lack of cure, no chance of remission, anticipated stigma, and even the possibility of reaching a point of suicidality. 36 Lastly, irritability, frustration, and restlessness often co-occur with painful attacks. 24,36,38 Patients describe feeling intense frustration because they feel like they have lost control over their lives. 36
In terms of cognitive functioning, patients with cluster headache often report struggling with attention, concentration, and overall functioning at work due to night-time attacks. 8,24 They also report trouble thinking clearly or concentrating due to the relentless nature of the pain. 24,36 Patients with cluster headache may also have difficulty concentrating, leading to simple forgetfulness (e.g., missed appointments), 24 as the pain monopolizes the patient’s full attention.
Quality of life
In addition to the psychiatric symptoms, emotional impact, and suicidal ideation described above, cluster headache results in a significant impact on other aspects of patients’ quality of life. The headache attacks are reported to complicate “the routine activities of everyday life,” including social contacts, work, and the ability to enjoy various activities. Family and other relationships can also be “heavily influenced.” 40
Multiple studies emphasized that the pain and associated symptoms that occur during the ictal (cluster) periods severely restrict the activities of daily living of patients living with cluster headache. 36,37,43 Conversely, the end of the ictal period may be accompanied by intense feelings of well-being, relief, and/or euphoria that are sometimes hard to manage, especially within the context of the cluster headache frequency. 39 Notably, however, during the interictal period, patients with cluster headache continue to experience restrictions and struggles in their daily lives and in their ability to perform simple activities of daily living.
Impact on work
There was a strong consensus across the identified literature that cluster headache has a significant, and often severe, impact on the work-life of patients. This impact is experienced by individuals across interrelated domains: difficulty in completing work tasks, absenteeism, workplace prejudice, and employment limitations, such as job loss, limited career opportunities, or work pattern changes. The impact of these work-related difficulties on an individual can be financial, emotional, and/or psychological, and are often profound. Limitations on career and work performance are an important component of the sense of overall loss of self and identity that is experienced by cluster headache patients, although it is important to note that the impact is heterogeneous across and within different populations. 43
Patients with cluster headache are more likely to be absent from work due to illness (39.4%) than either the general population (3.8%) or patients with migraine or tension-type headache (13.9%), 41 although the rate of absenteeism was considered by one study to be lower than expected, possibly due to the diurnal variation and short duration of the attacks, which allows patients to attend work between headaches. 43 However, while at work between headaches, living with cluster headache may impact the ability to complete tasks, 41,43,44 possibly due to exhaustion from prior attacks, sleep disturbances, and the psychological impact of living with cluster headache. 8 Nonetheless, the available evidence on how diurnal periodicity affects work function was inconclusive and further research is needed.
Matching their experience with HCPs, patients with cluster headache report feeling misunderstood or disbelieved by managers and their co-workers. 8,36 They may be accused of laziness and avoiding their obligations, or be refused permission to attend medical appointments to seek treatment. 36 The ultimate result for many patients with cluster headache is career limitation, job loss, or early retirement. 8,36,41 –43 For those patients with cluster headache who remain employed, changes in working patterns are often needed (either by altering working hours or working from home), 43 particularly for those patients who experience severe attacks. 41 Choi et al. found that pain severity was 9.3 on the visual analog scale in patients with cluster headache who required sick leave, compared with 8.8 in those who did not require sick leave. 41 Moreover, another study found that the proportion of employees was lower in the cluster headache group compared to those with other types of headache and headache-free control groups. 41 These data suggest that patients with cluster headaches may require a more flexible working environment to accommodate attacks, or indicate that patients with cluster headache have a more challenging experience maintaining employment.
Although none of the studies in this analysis contained data that explicitly described or calculated the financial or economic burden of cluster headache on patients, the reported effects on working life and career are likely to be associated with both a direct and indirect financial impact; however, additional studies are needed to confirm this inference.
Impact on social/leisure activities
The general literature on cluster headache points to a significant impact in the social and leisure setting, characterized by the disruption of and abstaining from related activities. In an analysis of headache conditions, including episodic cluster headache, patients reported significant disability in terms of sport, hobbies, and sex, resulting in abstention or reduced participation in all three. 44 In another study, one patient with cluster headache described that “birthday, Christmas, New Year’s Eve, Easter, every kind of holiday” was spent in fear. 37 As a result, patients commonly report avoiding certain activities, including drinking alcohol or attending loud or crowded venues, 24,37,43 leaving them feeling as though they are “shackled” to their homes. 24,36
Impact on family/interpersonal relationships
Those who suffer from cluster headache attacks experience impacts on their family and interpersonal relationships. They describe feeling useless as they are unable to fulfill their roles in the household, including doing chores and planning holidays. 24,37 Family life, housework, and social activities can be decreased to less than one-third of self-described "normal" during cluster headache attacks 43 ; female patients worry about the impact on their children, 37 and male patients worry about being perceived as weak or losing their status as the family provider. 36
Patients with cluster headache also frequently describe feeling like a burden to their friends and families. 24,37 Such feelings add to the sense of isolation and disconnectedness and may cause patients to seek out fellow sufferers online for compassion and understanding. However, for some patients, the presence of an understanding family member provides much-needed support, even though they cannot alleviate the burden of pain. 36,39
Impact on daily activities
Cluster headache attacks can result in patients feeling restricted from carrying out everyday activities, including driving and housework, or even taking care of their personal appearance. 24,36 For those patients who experience their attacks at night, they describe not having a regular sleeping pattern for days, 37,38,43 and going to bed worrying when the next attack will occur. Cluster headache can hinder the ability to do “simple” tasks and gets in the way of making decisions 24,36,39,43 ; over time, this can translate into less and less participation and diminished responsibility.
Stigma related to the misunderstanding of the disease
A further theme that emerged from the literature analysis was that patients with cluster headache are concerned with being stigmatized. As discussed in previous sections, this worry falls into three main categories: being labeled as lazy or malingering, 8,36 being labeled as psychotic or suicidal, 36,37 or being labeled as an addict or junkie. 36,40 In general, the literature in this evidence-based analysis highlighted the overall stigmatization that patients with cluster headache felt in the HCP setting, as well as in family, social, and professional settings. 8,36,37,40 In fact, patients reported concern that family and friends simply do not believe them, 24,36 with one study reporting that cluster headache breaks up families, relationships, and marriages. 40
Discussion and synthesis
Cluster headache results in significant physical and emotional burdens on patients, and this qualitative, evidence-based literature analysis indicates that there are several areas of unmet need for patients (Figure 2). Unmet healthcare needs can be defined as the difference between services “necessary to deal appropriately with health problems and services actually received,” 58 and can involve a broad range of barriers to healthcare access, including accessibility (cost, proximity), availability (timeliness), and acceptability (personal attitudes, personal circumstances), which was consistent among patients in the United States and Europe. 59,60 Notably, unmet healthcare needs can worsen QoL, 61 increase mortality, 62 and negatively impact patient mental health. 63

Unmet needs in patients with cluster headache.
Patients with cluster headache have significant unmet needs. There is a lack of comprehension across society (HCPs, employers, peers, and family) regarding the overall diagnosis of cluster headache, the epidemiology and pathophysiology of the disease, the inconsistent and varied symptomatology that is exhibited, as well as the burden that is a direct impact of this chronic disease. Patients are frequently failed by HCPs across all three domains of healthcare access (accessibility, availability, and acceptability). Central to this failure is the patient’s belief that physicians lack a clinical understanding of the cluster headache diagnosis and do not believe the extent of the pain experienced by the patient. The study by Buture et al., which included both GPs/PCPs and neurologists, supports this assertion, noting that many physicians are confused by the diagnosis and are unsure of the clinical pathway/clinical guidelines. 8 This in turn gives rise to both delayed diagnosis and misdiagnosis. Patients typically spend many years battling symptoms without diagnosis or viable treatment, 36 or they receive unnecessary treatments for the misdiagnosed disorder that are inappropriate and ineffective for cluster headache. 8 This delay can result in patients resorting to alternative therapies or illegal substances.
The lack of understanding received from HCPs is further compounded by the lack of support from family and colleagues, with patients accused of avoiding their responsibilities or exaggerating their pain. 8,36 Moreover, continued struggles in the interictal period related to fear of the next attack and anxiety about the future 36,37,40,43 highlight the general need for a reduction in the physical and emotional impacts of cluster headache across the temporal course of the condition.
Importantly, patients with cluster headache are known to be at particularly high risk of suicidal ideation, 15,55 with the condition colloquially referred to as “suicide headache.” 36,38,40 The evidence from this analysis indicates that patients may resort to self-harm, and many exhibit suicidal thoughts or behaviors. 36 –39 In recent studies, patients with cluster headache were shown to have a significant increase in active and passive suicidal ideation; specifically, patients with chronic cluster headache were at a higher overall risk when compared to the sociodemographically-matched control group. 15,55 Importantly, the authors noted that the likelihood of suicidal ideation was predicted by the presence of demoralization. The qualitative data analysis provides evidence of this link, in which a loss of vitality and identity was a recurring theme, with patients using extremely negative descriptors, such as “violated,” “empty,” “canceled,” “impotent,” and “helpless.” 36,39 Although patients with cluster headache are also reported to be at high risk of developing depression, 64 with lifetime odds of a depression diagnosis almost three times higher in patients with cluster headache than controls, 64 demoralization is a distinct entity and should be specifically addressed when formulating a treatment plan for patients. 55 Overall, patients with cluster headache require accurate and timely diagnosis of their condition by HCPs with an understanding of their symptoms. This should be followed up by improved access to healthcare services, including psychological counseling and therapy and occupational therapy for work and school. This, in turn, would improve the ability of patients to maintain their quality of life, workplace productivity, and social relationships.
Effective and safe treatment options, including appropriate abortive and preventive strategies, are key to managing cluster headache. Our analysis found that a central unmet need is that many patients feel that there are no viable treatment options for cluster headache and that following any prescribed preventive medication course is futile. 36,40 Effective and safe treatment would solve a number of other problems that arise from this unmet need, which we discuss below. This perception of futility is mirrored in the cost distribution, with abortive treatment of attacks comprising the bulk of overall treatment costs related to cluster headache, with a relatively low spend on preventive medication. 42 While this disproportionate expense on abortive treatment is indicative of an unmet need in and of itself, the combination of: lack of healthcare provider knowledge and understanding; additional unneeded medical treatments and clinic visits to various physicians (i.e., (psychologists, physical therapists, chiropractors, traditional healers, and acupuncure specialists)); 36 delayed or misdiagnosis; ineffective treatment options; and sometimes prohibitive treatment costs leads to a “perfect storm” of unmet medical need for patients with cluster headache. This unmet medical need leads to a sense of helplessness and isolation, pushing the patient toward alternative and potentially unsafe treatment options. 36,40 Making use of alternative, sometimes illegal, treatments and therapies can be differentially conceptualized as a consequence of unmet needs, highlighting a lack of effective cluster headache treatments in some patients or as a solution to unmet needs. However, by resorting to illicit/illegal drugs in the attempt to ameliorate their pain, patients are seen to be engaging in risky and negative behaviors, which they themselves feel to be an additional stigma associated with their condition. 40 Although it seems that some HCPs might advise patients to try alternative treatments, 40 these agents cannot be medically prescribed, 65 and it is the online community that plays the major role in sourcing psychoactive substances and determining the optimal dosage. 40,66 As such, patients run the risk of using mislabeled or impure substances that may exacerbate negative effects or cause severe toxicity. 40 Finally, patients with cluster headache often report a loss of identity, 36,39 and this may be exacerbated by risky lifestyle choices or increased anxiety from fear of addiction and stigma.
Additional consequences resulting from current unmet needs in patients with cluster headache include an increased healthcare burden due to delayed diagnosis or misdiagnosis. As previously noted, the lack of awareness of cluster headache diagnostic criteria among all HCPs results in delayed diagnosis, with misdiagnosis resulting in multiple referrals, unnecessary procedures, and costly emergency room visits. 8,43 Furthermore, it can add complexity to the overall disease trajectory: patients with cluster headache who develop mistrust initially may subsequently complicate diagnosis through self-advocacy from online sources, resulting in further frustration and desperation. This, in turn, can lead to patient-requested secondary referrals for scans and other procedures, 8 creating a cyclical dynamic and potentially extending the periods of misdiagnosis and appropriate treatment delay. Increased healthcare burden due to unmet needs also relates to the experience of symptomatology; in addition to the headache pain, the associated experiences of psychiatric comorbidities and suicidality contribute to ongoing financial and societal costs. Patients with cluster headache also may be more likely to have an unhealthy lifestyle compared with healthy individuals, with greater rates of smoking, alcohol abuse, and obesity. 67
The increased emotional and physical impact that cluster headache has on patients is a key unmet burden, which is directly connected to the isolation and vulnerability that many patients feel. 36,40 Patients may self-isolate due to their symptoms and abstain from normal family activities due to fear of the next attack or because of perceived stigma, which significantly disrupts their work and social lives. 8,24,36,37,40,41 Patients report decreased quality of life, loss of workplace productivity, limited career/workplace opportunities, reduced ability to perform activities of daily living, and family break-ups, which adds to the stress, distress, and frustration that many patients already feel. Due to the stigma that many patients experience with their HCP as well as in their family or workplace environment, a large number of individuals with cluster headache rely heavily on online forums and communities to get the support and understanding they desire, which often provides collective thinking of potential treatment solutions for their chronic condition. 40 Addressing the emotional and physical burden is a key unmet need in the treatment of cluster headache that should not be overlooked in any patient management strategy.
Importantly, some aspects of the unmet need for patients with cluster headache may be a reflection of wider societal inequities, resulting from a historical over-estimation of cluster headache as a condition predominantly confined to men 67 ; however the male preponderance is under debate as recent studies have shown the male to female ratio of cluster headache as low as 2:1. 53,68 This view is likely to have biased societal understanding of cluster headache (including patients themselves, as well as their family, peers, and HCPs). 69 This trend was also noted in the studies evaluated in the qualitative review, with one study justifying the selection of male patients with the statement that cluster headache “is typically a male disease.” 36 As such, future studies should seek careful representation and analysis of potentially gendered findings, such as differences in diagnosis and associated treatments, in order to be applicable to the heterogeneous real-world patient population.
Several minor limitations to this analysis exist. Data extraction was undertaken independently by two researchers, with the studies split between them, potentially resulting in discrepancies or personal bias. Although this study utilized a comprehensive and systematic search methodology, including the use of specific bibliographic database searching, citation analysis, and expert consultation, it could have been rendered more comprehensive by the additional incorporation of other electronic bibliographic databases, thereby reducing any inherent selection bias.
Additionally, the body of literature was limited due to the changes in ICHD criteria in 2018, with definitions of chronic cluster headache in studies pre-2018 not reflecting the current definition and so excluded. Furthermore, some papers used majority male cohorts, impacting the resulting data and limiting the qualitative data on the female experience. In addition, some of the selected studies did not assess or report pertinent details such as ethnicity of the patients or the type of healthcare system utilized, which may influence disease symptomology or patient experience, respectively. Finally, in some papers it was difficult to tell whether results referred to cluster headache, another headache disorder, or a group of headache disorders; as such, we were forced to broadly extrapolate information as relating to cluster headache and were unable to clearly differentiate between the episodic and chronic condition based on the description of disease by the patients or authors.
Conclusions
In this article, we reported a qualitative assessment of the scientific literature database, which focused on patient experiences living with cluster headache, and provide a synthesis of the resulting unmet needs in these patients (Figure 2). We found that quality of life is generally much lower in persons living with cluster headache, with significant psychological, social, and socio-economic burden, as well as work-related disability. The disease trajectory for a person with cluster headache includes diagnostic delay and misdiagnosis, primarily due to a lack of knowledge regarding the disease among HCPs and the perception of patients regarding a lack of effective treatment options. Individuals experience the impact of cluster headache across interrelated domains: difficulty in completing work tasks, absenteeism, workplace prejudice, and employment limitations. The subsequent financial, emotional, and psychological burden can be profound. More research is needed to substantiate reported effects on working life that are likely to be associated with a direct financial impact. While not a primary analysis endpoint, no difference in disease burden or unmet needs were identified between patients with cluster headache in Europe or the United States. Further, the kinds of identified burden and unmet needs did not appear to differ between patients with episodic or chronic cluster headache.
Future directions
A clear need exists for disease-state education for patients, caregivers, and clinicians regarding the trajectory and burden of the disease. An increased understanding and awareness of the diagnostic criteria and treatment management of cluster headache would reduce the sense of isolation and demoralization as well as other psychiatric symptoms expressed by patients. Addressing this unmet need should also assist in reducing the overall direct and indirect utilization of healthcare resources that occurs with cluster headache patients.
The impact of cluster headache on the quality of life of patients with cluster headache, as highlighted throughout this paper, along with the widely reported use of alternative or illicit substances, emphasizes both the debilitating nature of the disease and the limitations of available prescribed treatment options to these patients. Not only does the burden of cluster headache impact the patient, it also places significant strain on the family, workplace, and society in general. Without viable treatment options, patients may turn to illicit drug-seeking behaviors or experience suicidal ideations. Further research into treatment options for cluster headache—that are both well-tolerated and effective—is warranted to address this unmet need.
Key findings
Quality of life is generally much lower in persons living with cluster headache, with significant psychological, social, and socio-economic burden, as well as work-related disability.
Patients with cluster headache consistently express a lack of vitality and loss of identity across studies.
Misdiagnosis, diagnostic delays, and a perceived lack of viable and effective treatment options contribute to the unmet need.
Supplemental material
Supplemental Material, sj-pdf-1-rep-10.1177_25158163221096866 - Patient-identified burden and unmet needs in patients with cluster headache: An evidence-based qualitative literature review
Supplemental Material, sj-pdf-1-rep-10.1177_25158163221096866 for Patient-identified burden and unmet needs in patients with cluster headache: An evidence-based qualitative literature review by Emily Freeman, Michael Adair, Dori Beeler, Rozanne Casper, Melissa P Herman, David Reeves and Stefan Reinsch in Cephalalgia Reports
Footnotes
Acknowledgments
The authors thank Sally-Anne Mitchell, PhD, and Philip Sjostedt, BPharm, of The Medicine Group, LLC (New Hope, Pennsylvania, USA) for providing medical writing support, which was funded by H. Lundbeck A/S, Copenhagen, Denmark, in accordance with Good Publication Practice guidelines. The authors also thank Heather-Rae Espinoza, who was involved with the development of the initial research hypothesis and information gathering.
Author contributions
All authors played a major role in the acquisition, analysis, or interpretation of data and revised manuscript critically for important intellectual content.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EF was a full-time employee of H. Lundbeck A/S through October 26, 2021. MA and MPH are full-time employees of H. Lundbeck A/S. RC and DR are full-time employees of Clinigma. DB and SR are consultants for Clinigma. SR is a part-time employee of the Centre for Health Service Research and the Department of Pediatrics of the Brandenburg Medical School Theodor Fontane, Germany.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This analysis was funded by H. Lundbeck A/S, Copenhagen, Denmark. The publication was supported by H. Lundbeck A/S, Copenhagen, Denmark.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.