
Abstract
Objective
To estimate the relative frequencies of hemicrania continua and its clinical features in adult patients who were evaluated for headache in a clinic-based setting.
Methods
PubMed and Embase were searched for observational, clinic-based studies published between 1 January 2004 and 1 February 2022, that reported on the relative frequencies of hemicrania continua and its clinical features. Two independent investigators (HMA and SA-K) screened titles, abstracts, and full text-articles. A random-effects meta-analysis was conducted to estimate pooled relative frequencies of hemicrania continua and its clinical features across clinic-based studies.
Results
Eleven clinic-based studies were deemed eligible for inclusion. Of these, eight studies reported on the relative frequency of hemicrania continua among adult patients (n = 9854) who were evaluated for headache in a tertiary care unit. The pooled relative frequency of hemicrania continua was found to be 1.8% (95% CI; 1.0–3.3). Considerable heterogeneity was noted across studies (I2 = 89.8%). The three most common symptoms associated with hemicrania continua were lacrimation (72.3%), conjunctival injection (69.8%), and restlessness/agitation (60.2%).
Conclusion
The findings of this meta-analysis suggest that there is limited epidemiologic data on the relative frequencies of hemicrania continua and its clinical features. Standardized data acquisition and reporting are needed to estimate prevalence rates more accurately and to better understand epidemiologic patterns. This, in turn, should increase awareness of the impact that hemicrania continua has in clinical practice.
Keywords
Introduction
Hemicrania continua is a rare neurologic disorder that is classified as a trigeminal autonomic cephalalgia (TAC) in the International Classification of Headache Disorders, 3rd edition (ICHD-3), (1–3). The clinical presentation is characterized by persistent unilateral headache for more than three months accompanied by autonomic symptoms ipsilateral to the headache (4). Diagnostic criteria require an absolute response to therapeutic doses of indomethacin (4). Distinction of hemicrania continua from other TACs and migraine can be challenging for clinicians which, in turn, might lead to misdiagnosis and failure to initiate appropriate treatment with indomethacin (2,5).
All of what we know about hemicrania continua comes from clinic-based studies (6,7), and among those with hemicrania continua, the relative frequencies of specific headache features or autonomic symptoms remain unclear (6,8–10). A synthesis of the existing evidence is therefore needed to increase awareness among clinicians and facilitate a timely and correct diagnosis. Here, we examine the relative frequencies of hemicrania and its clinical features in adult patients who are evaluated for headache in a clinic-based setting. This is followed by a review of methodological limitations to better guide future research efforts.
Methods
Search strategy
This systematic review and meta-analysis is reported according to the Meta-analyses Of Observational Studies in Epidemiology (MOOSE) Checklist (11). A database search was carried out in PubMed and Embase to identify clinic-based, observational studies published between 1 January 2004 (hemicrania continua was first introduced in ICHD-2), and 1 February 2022, that reported on the relative frequency of hemicrania continua and/or its clinical features in adult patients. The following search string was used: “hemicrania continua”. No language restrictions were applied, and reference lists of full-text screened articles were searched to identify additional studies that might be eligible for inclusion. We also contacted the relevant investigators to supplement incomplete reports or obtain unpublished data.
On 18 July 2022, an additional database search was carried out in PubMed and Embase to identify clinic-based, observational studies on the relative frequency of hemicrania continua that had been published between 1 January 1984, and 31 December 2003. None of the screened papers reported on the relative frequency of hemicrania continua, and the available literature was limited to case reports and case series that used various case definitions to assign patients with a diagnosis of hemicrania continua.
Selection criteria
Eligible studies included those with an observational, clinic-based, prospective, retrospective, or cross-sectional design that reported original data on the relative frequency of hemicrania continua and/or its clinical features in adult patients (≥18 years of age) who were evaluated for headache. A diagnosis of hemicrania continua had to be made in accordance with ICHD-2, ICHD-3β or ICHD-3 (Table 1), (1,12,13). Eligible studies also had to include at least 10 study participants. Table 2 summarizes the full list of inclusion and exclusion criteria.
Evolution of the diagnostic criteria for hemicrania continua.

Inclusion and exclusion criteria.

ICHD: International Classification of Headache Disorders.
Study selection and data extraction
Two independent investigators (HMA and SA-K) screened titles, abstracts, and full-text articles. Any disagreements were resolved by the opinion of a third investigator (HA). For each study deemed eligible for inclusion, HMA and SA-K independently extracted data using a pre-defined data extraction form. The following data was collected for each study: country, study design, ICHD-criteria used to diagnose hemicrania continua, the number of participants, the number of participants with hemicrania continua, the number of male and female participants, and the number of male and female participants with hemicrania continua. Data were also extracted for the relative frequency of individual clinical features of hemicrania continua: conjunctival injection, lacrimation, nasal congestion, rhinorrhea, eyelid oedema, forehead and facial sweating, forehead and facial flushing, sense of fullness in the ear, miosis, ptosis, restlessness, agitation, aggravation of pain by movement, photophobia, phonophobia, and nausea.
Quality assessment
Quality assessment of the included studies was performed by two independent investigators (HMA and RHC) using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Studies Reporting Prevalence Data (14). This instrument comprises nine questions that can be answered with one of four standardized options: yes, no, unclear, and not applicable.
Data synthesis and analysis
The primary outcome was the relative frequency of hemicrania continua in observational, clinic-based studies, and the secondary outcomes included relative frequencies of individual clinical features of hemicrania continua in observational, clinic-based studies. A qualitative assessment was performed using a pre-defined data extraction form and the JBI Critical Appraisal Checklist for Studies Reporting Prevalence Data. A random effects meta-analysis was conducted, whenever possible (≥2 eligible studies), for all outcomes using a random intercept logistic regression model on log transformed data. The Maximum Likelihood method was used to calculate between-study variance while the normal approximation method was used to calculate confidence intervals. The I2 statistic was used to assess between-study heterogeneity, with values ≥75% suggestive of considerable heterogeneity. All statistical analyses were performed with R version 3.5.2 using the “meta” and “metafor” packages.
Results
The literature search identified 957 citations, of which 946 were excluded based on the title and abstract screening (Figure 1). Eleven clinic-based studies were retrieved for further review and met the eligibility criteria for inclusion (2,15–24). All included data originated from the outpatient clinic of tertiary care centers. Six studies had a prospective design (17–22) while the remaining five were retrospective cohort studies (2,15,16,23,24).

Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram.
Of the 11 included studies, eight reported on the relative frequency of hemicrania continua in adults (2,15–21), and four reported on the relative frequencies of individual clinical features (17,22–24). Based on the quality assessment of all included studies, it was deemed that study quality was high in four (15,18,21,22) studies, moderate in five (2,16,17,23,24), and low in two (19,20).
Relative frequency of hemicrania continua
The pooled relative frequency of hemicrania continua was estimated to be 1.8% (95% CI, 1.0–3.3) among adult patients (n = 9,854) who were evaluated for headache in a clinic-based setting (Figure 2, Table 3), (2,15–21). Considerable heterogeneity was noted across studies (I2 = 89.8%). The lowest reported relative frequency of hemicrania continua was 0.4% (2), whereas the highest was 9.2% (15).
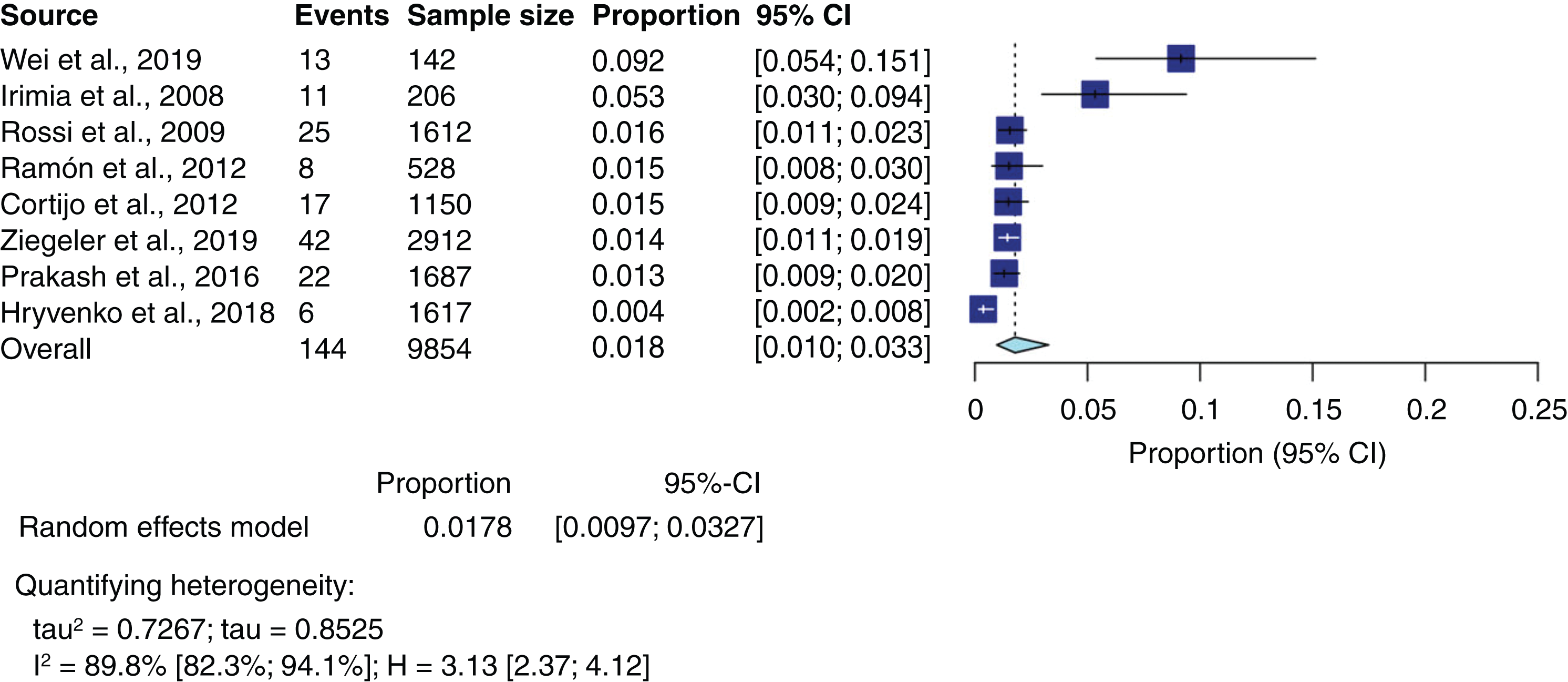
Pooled relative frequency of hemicrania continua and event rates for included studies.
Characteristics of the included studies on the relative frequency of hemicrania continua.

ICHD: International Classification of Headache Disorders; P: Physician, Q: Questionnaire.
Based on data from two clinic-based studies (n = 3,299), gender-specific pooled relative frequencies of hemicrania continua were calculated (18,20). The pooled relative frequency was 0.79% (95% CI, 0.5-1.0; I2 = 0.0%) for women and 0.64% (95% CI, 0.4-1.0; I2 = 0.0%) for men.
Autonomic symptoms and restlessness/agitation in hemicrania continua
The frequency of individual autonomic symptoms in hemicrania continua was assessed retrospectively in two studies (23,24) and prospectively in two other studies (17,22) (Table 4). Three studies also provided data on the occurrence of restlessness/agitation (22–24).
Prevalence of Individual Autonomic Symptoms in Hemicrania Continua.

ICHD: International Classification of Headache Disorders; P: Physician.
The pooled relative frequency of lacrimation was 72.9% (95% CI, 63.2-80.9; I2 = 0.0%) based on data from clinical samples (22–24). The corresponding pooled relative frequencies were 69.8% (95% CI, 59.9-78.1; I2 = 0.0%) for conjunctival injection (22–24), 60.2% (95% CI, 37.7-79.0; I2 = 83.0%) for restlessness/agitation (22–24), 45.9% (95% CI, 33.9-58.4; I2 = 0.0%) for rhinorrhea (22,24), 44.8% (95% CI, 35.2-54.8; I2 = 0.0%) for nasal congestion (22–24), 12.1% (95% CI, 6.2-22.4; I2 = 39.1%) for ptosis (22,23), 9.8% (95% CI, 4.5-20.2; I2 = 0.0%) for eyelid edema (22,24), 3.3% (95% CI, 0.8-12.2; I2 = 0.0%) for miosis (22,24), 15.2% (95% CI, 8.4-25.2; I2 = 0.0%) for forehead and facial flushing (22,23), and 9.1% (95% CI, 4.1-18.8; I2 = 0.0%) (22,23) for forehead and facial sweating (22,23). In addition, one study provided data on the sensation of fullness in the ear which was reported by 4 (12.9%) of 31 patients with hemicrania continua (22). No studies reported data on the aggravation of pain by movement.
Photophobia, phonophobia, and nausea in hemicrania continua
Four studies, comprising 107 patients with hemicrania continua, provided data on the occurrence of photophobia, phonophobia, or nausea (17,22–24). The pooled frequencies were 34.6% (95% CI, 26.2-44.0; I2 = 0.0%) for photophobia (17,22–24), 21.6% (95% CI, 12.7-34.2; I2 = 0.0%) for phonophobia (17,22–24), and 43.8% (95% CI, 31.8-56.7; I2 = 57%) for nausea (22–24).
Discussion
To our knowledge, this is the first systematic review and meta-analysis on the relative frequencies of hemicrania continua and its clinical features in adult patients who were evaluated for headache in a clinic-based setting. In summary, the pooled relative frequency of hemicrania continua was found to be 1.8% based on data originating from the outpatient clinic of tertiary care centers. The three most common symptoms associated with the unilateral headache were lacrimation (72.3%), conjunctival injection (69.8%), and restlessness/agitation (60.2%).
Methodological considerations
The calculated estimates should be interpreted with caution, as some were limited by considerable between-study heterogeneity, and most studies were of low to moderate quality. Since the number of included studies is low, it is not possible to explore causes of heterogeneity across studies using meta-regression or subgroup analyses. We speculated that specific methodological differences might, in part, explain the considerable between-study heterogeneity. First, the pooled relative frequency of hemicrania continua was less than 2% in six of the eight studies that provided data for our meta-analysis (2,16,18–21). In comparison, the remaining two studies had smaller samples and reported higher relative frequencies of hemicrania continua among adult patients who were evaluated for headache (15,17). This might then explain some of the observed between-study heterogeneity, as small samples increase the likelihood of random errors. Second, the ICHD diagnostic criteria for hemicrania continua has evolved over time (1,12,13). More clinical features have been included in ICHD-3β and ICHD-3 (1, 12), compared with ICHD-2 (13). This might account for some of the observed between-study heterogeneity, as five of the included studies applied the ICHD-2 criteria to diagnose hemicrania continua (17,19–21,24), while the remaining six studies applied the ICHD-3β or ICHD-3 criteria (2,15,16,18,22,23). A quick glance on the relative frequencies that were reported in the included studies does, however, reveal that there is no obvious association with the applied ICHD version. Third, subtypes of hemicrania continua have been introduced in ICHD-3 criteria and include a remitting and unremitting subtype (1,5). The former is an important change from ICHD-2 in which pain-free periods were not allowed (13). Fourth, the method for data collection varied across studies, with some acquiring data using a prospective design (17–22) while others used a cross-sectional, retrospective design (2,15,16,23,24). The former might prevent clinicians from verifying the diagnosis of hemicrania continua in suspected cases, as evaluating the response to indomethacin carries the risk of loss to follow-up. Interestingly, none of the included studies reported whether the clinicians, in some cases, had been unable to verify the diagnosis because the response to indomethacin could not be evaluated at follow-ups. A cross-sectional, retrospective study design is nonetheless more problematic, and the quality of data might be limited by inaccurate and more so incomplete documentation, particularly on the frequency of specific symptoms. Most included studies did not report whether specific clinical features were absent (22–24). Absence of specific clinical feature are thus likely to be underreported. Lastly, study samples were generally small and only two studies provided data on the gender/sex distribution in patients with hemicrania continua which, in turn, precludes us from exploring whether hemicrania continua is more common in a specific gender (18,20). In the two studies with robust gender data, there was a slight gender predilection for women.
Hemicrania continua and other TACs
The epidemiologic patterns of TACs have generally received limited attention, with most observational studies focusing exclusively on people with cluster headache. There is, to our knowledge, only one clinic-based, observational study, in which the relative frequencies of several TACs have been directly compared in patients presenting with unilateral headache (18). The authors enrolled consecutively 307 adult patients with side-locked headache and facial pain who had been referred to a tertiary care unit. Following clinical evaluation and magnetic resonance imaging of the brain, 91 of 307 patients were diagnosed with a TAC. Of these, 47 patients had cluster headache, 22 had hemicrania continua, 14 had short-lasting unilateral neuralgiform headache attacks, nine had paroxysmal hemicrania, and three had probable TAC. These results indicate that cluster headache is the most prevalent TAC in practice which accords well with our clinical experience. Further large-scale studies are however needed to ascertain how frequently specific TACs are encountered in practice. On a similar note, it would also be useful to compare the relative frequencies of individual autonomic symptoms between TACs. This has, to our knowledge, only been examined in one clinic-based, observational study (23), in which 35 patients with hemicrania continua and 27 patients with paroxysmal hemicrania were included. No differences were found between the two groups in terms of the severity of cranial autonomic symptoms.
Hemicrania continua and migraine
A frequent misdiagnosis of hemicrania continua is migraine (20,25). This is, in part, explained by nausea, photo-, and phonophobia being common in both headache disorders, albeit considerably less prevalent in hemicrania continua (26). The present study found that the prevalence rate of these symptoms in patients with hemicrania continua were 43.8% for nausea, 34.6% for photophobia, and 21.6% for phonophobia. The corresponding figures are 80–90% for photophobia and phonophobia but sometimes lower for nausea. (27,28). Nonetheless, one study found that 24 (71.0%) of 34 patients with hemicrania continua met the ICHD criteria for migraine during their headache exacerbations of moderate to severe intensity (25). The differential diagnosis between hemicrania continua and migraine might depend upon the application of the requirement that the headache is not better accounted for by another disorder. Unilateral headache is a diagnosis feature of both migraine and hemicrania continua (1). A few patients with migraine also benefit from treatment with indomethacin which can further contribute to diagnostic confusion (29,30). However, there remains clear differences between hemicrania continua and migraine. Migraine usually alternates sides while hemicrania continua is almost always side locked. Though cranial autonomic symptoms can occur with migraine as well as hemicrania continua, they are more prominent in the later. The restlessness/agitation of hemicrania continua contrasts with the preference to lie in a dark, quiet room during migraine attacks (31).
Indomethacin response
Hemicrania continua is defined by an absolute response to therapeutic doses of indomethacin (1). This diagnostic requirement is somewhat problematic because it eliminates all suspected cases who have contraindications (e.g. gastric ulcers, renal failure) to indomethacin use. Moreover, some patients might not receive therapeutic doses of indomethacin. One case series found that six of 39 patients fulfilled all ICHD-2 criteria for hemicrania continua, except these patients did not respond absolutely to indomethacin (4). Other studies have also reported cases in which the patients seemingly met the ICHD criteria for hemicrania continua apart from not having an absolute response to indomethacin (16). For instance, one cross-sectional retrospective study identified that nine out of 62 patients met all ICHD-2 criteria except a complete response to indomethacin (24). Another study enrolled 44 patients with a putative diagnosis of HC and excluded six patients, due to no or incomplete response to indomethacin (22). There is also an absence of data on whether long-term use of maintenance doses of indomethacin continues to provide absolute therapeutic response.
Future directions and conclusions
Among adults evaluated for headache at the outpatient clinic of tertiary care centers, hemicrania continua was diagnosed in 1.8% with some considerable heterogeneity among studies. Further work is, however, needed to ascertain the prevalence of hemicrania continua and its clinical features, as small samples and inconsistent reporting of data limit the generalizability of our results. Methodologic shortcomings in the available literature must, in particular, be addressed in the future investigations. Above all, it is important to identify individual clinical features (including autonomic symptoms) associated with hemicrania continua more accurately. This can be done by asking open-ended questions at first and then follow up by using a pre-defined list of individual clinical features. The latter in isolation might lead to overestimations due to agreement and recall bias which are prevalent in survey research. In this context, it can also be useful to develop diagnostic headache diaries with daily entries in order to better characterize subtypes of hemicrania continua prospectively and avoid misdiagnosis. An international expert consensus on best scientific practices and methodologic guidelines is probably a pre-requisite to adequately characterize the epidemiologic patterns of hemicrania continua and other rare headache disorders.
Key findings
Among adult patients who were evaluated for headache in a tertiary care unit, the pooled relative frequency of hemicrania continua was found to be 1.8% (95% CI; 1.0-3.3). The three most prevalent symptoms associated with hemicrania continua were lacrimation (72.3%), conjunctival injection (69.8%), and restlessness/agitation (60.2%). The scarcity of robust epidemiologic data limits the conclusions that can be made based on the present meta-analysis. Further studies are thus needed to estimate prevalence rates of hemicrania continua using standardized methods of data acquisition.
Footnotes
Author Contributions
HMA, FMA and HA conceived and designed (including search strategies) the review. HMA did the literature search with SA-K. HMA and SA-K wrote the first and subsequent drafts of the manuscript. FMA, SA-K, RHC, RBL and HA participated in critical revision and writing of the article. All authors have seen and approved the final version.
Declarations of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SA-K has received honoraria from Allergan and Teva and consultant fees from Amgen and Allergan. SA-K received honoraria for lecturing from Allergan and Avanir Pharmaceuticals. FMA received honoraria as an advisory board member and speaker for Lundbeck, Novartis, Eli Lilly and Teva. FMA serves a member of the national headache guidelines committee in Denmark. RBL receives research support from the NIH, FDA as well as the National Headache Foundation and the Marx Foundation. He also receives research support from Allergan/Abbvie, Amgen, Eli Lilly and Electrocore. He receives personal fees as a consultant or advisor from Allergan/Abbvie, Amgen, Biohaven Holdings, Dr. Reddy’s, GlaxoSmithKline, Grifols, Impel NeuroPharma, Novartis, Lundbeck, Merck, and Teva Pharmaceuticals. He holds stock or options in Biohaven Holdings and CtrlM Health. HA reports personal fees from Teva. The other authors declare no potential conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.