
Abstract
Background
Health-related quality of life (HRQoL) is emerging as an important element of clinical research in primary headache disorders, allowing a measure of the impact of headache on patients’ well-being and daily life. A better understanding of this may contribute to improved resource allocations and treatment approaches.
Objective
The objective of this study is to review available data on HRQoL in primary headache disorders and identify any influencing factors.
Methods
Database searches including MEDLINE, PsycINFO and EMBASE were performed. Studies that investigated HRQoL in patients with primary headache disorders were included and reviewed. Trials that evaluated the efficacy of medications or interventions were excluded.
Results
A total of 80 articles were included in the review. Both physical and emotional/mental aspects of HRQoL were impaired across headache subtypes, although the extent varied depending on headache type. A number of factors influencing HRQoL were also identified.
Conclusion
This narrative review suggests that headache, particularly in its chronic form, has a great impact on HRQoL. Clinical practice should not solely focus on pain alleviation but rather adopt routine assessment of HRQoL. Furthermore, identification and management of associated psychological comorbidities, which can significantly influence HRQoL in headache sufferers, are essential for optimal clinical management.
Keywords
Introduction
Health-related quality of life (HRQoL) measures the impact of an illness on the patients’ physical, emotional and social functioning (1). The importance of measuring HRQoL in patients with chronic disorders has become an area of interest in clinical practice, as it provides the patient’s subjective experience of the impact of his or her disorder (2). Various generic instruments have been developed to evaluate HRQoL, which can be used across different disorders, allowing comparisons with other medical conditions and with healthy controls (3,4).
Within the headache field, much of the work relating to HRQoL has focused mainly on migraine, as it is one of the most frequent primary headache diagnoses. Despite the lack of any physical abnormality, the nature of the attacks with their recurring pain and associated symptoms often influences the patients’ ability to function normally. The World Health Organization (WHO) in its Global Burden of Disease study conducted in 2000 reported that migraine is in the top 20 causes of disability worldwide (5). Migraine-specific HRQoL scales have thus been developed to measure the areas of life that may be affected in this patient group. This includes the Migraine-Specific Quality of Life measure (MSQoL) (6), the Migraine-Specific Quality of Life Questionnaire (MSQ) (7,8), and the 24-hour Migraine Quality of Life Questionnaire (24-hr-MQoLQ) (9). Furthermore, a number of headache disability scales that assess disability due to headaches are available, including the Migraine Disability Assessment Scale (MIDAS), the Headache Impact Test (HIT-6) and the Henry Ford Headache Disability Inventory (HDI). Although disability and HRQoL are independent constructs, they are closely related and assessment of disability is often included as part of HRQoL measures (10).
Meanwhile, HRQoL in other primary headache disorders such as tension-type headache (TTH) and cluster headache (CH) have been less studied and disease-specific measures for them are currently unavailable. We reviewed the literature with two main objectives: 1) to assess HRQoL in primary headache disorders, and 2) to identify factors that may influence HRQoL in these disorders.
Methods
Search strategies and data sources
An electronic search of MEDLINE (1950–present), PsycINFO (1974–present), EMBASE (1974–present) and the Cochrane Library databases was carried out using the following terms: (“quality of life” OR “disability” OR “functioning”) AND (“headache” OR “primary headache disorders” OR “primary headache” OR “migraine” OR “tension-type headache” OR “tension headache” OR “cluster headache” OR “trigeminal autonomic cephalalgias” OR “chronic headache” OR “chronic daily headache”) for relevant published literature up to the end of September 2013. Selection criteria were studies that: assessed HRQoL or disability in primary headache disorders or chronic daily headache (CDH) as either the primary or secondary outcome, used the International Headache Society (IHS) criteria for definition of primary headache disorders and articles published in English. We excluded studies that recruited patients with medication-overuse headache (MOH) and those evaluating the efficacy of medications or non-medication interventions, as our aim was to assess HRQoL in the different primary headache disorders per se, and not the changes to it following treatment. The quality of the included studies was assessed using the Newcastle-Ottawa Scale (NOS), which evaluates for quality of study design in three aspects: participant selection (four questions), participant comparability (one question) and outcome of studies (three questions). A maximum of four points can be awarded for selection, two for comparability and three for outcome, with a possible total score of nine points. Studies scoring more than five points are considered to be of moderate quality, whereas those scoring eight and above are deemed to be of good quality (11). The two primary authors (NAB and ST) reviewed the retrieved studies and any disputes were resolved by the final author (MM). Results are presented with a narrative approach.
Results
In total 422 citations were identified from the database and 288 were excluded after abstract screening, as they did not meet the selection criteria, were not available in full text or were duplicate publications. A further 59 were excluded after the full articles were analyzed, as they did not meet the inclusion criteria or included patients with MOH. Five additional articles identified from the references were included. Following this, 80 articles were eligible for the final review (Figure 1), which looked at various primary headache subtypes. Using the NOS, 68 studies were found to be of moderate to good quality. Of those studies that were deemed to be of poor quality, scoring four points or less on the NOS, seven were assessing HRQoL in migraineurs, three studies were comparing HRQoL in patients with migraine and TTH and one study each were conducted on CH and CDH patients. One of the reasons for the low scores in these studies was the small sample sizes of the study groups.
Flow diagram showing the results of the literature search.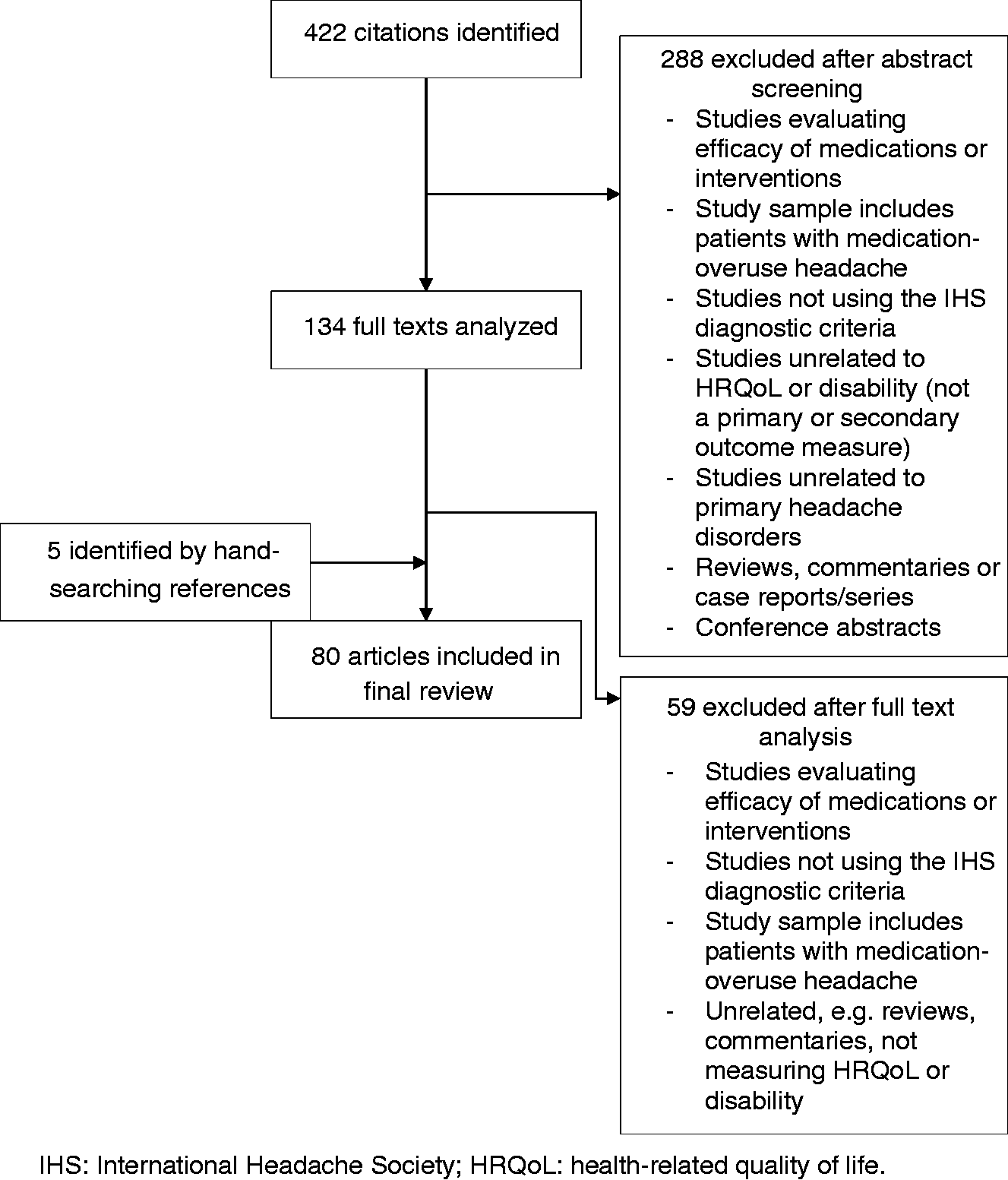
We decided to include all the studies in our narrative synthesis, as we wanted an overall overview of the published literature in this field to date, especially considering the limited number of studies in some headache subtypes, notably TTH and CH. Most of the studies reviewed assessed HRQoL on patients with migraine (73 studies), with comparatively fewer studies performed on patients with TTH (26 studies) and CDH (23 studies), and even fewer in CH patients (nine studies) (Figure 2). Furthermore, most studies used generic instruments (30 studies) and headache disability scales (39 studies) (12–36) as their measure. The most widely used generic scale was the Short Form 36 (SF-36) (22 studies) (12–18,37–52). Migraine-specific HRQoL scales were used in only 14 studies, the majority of which were assessing HRQoL in migraineurs (12,13,19–21,37,39,49,53–59).
The pie chart shows the headache types included in the 80 studies reviewed.
HRQoL by headache diagnoses
Migraine
Studies of quality of life in migraine.

These are studies that have focused specifically on migraine; however, our overall migraine group (73 in total) also took into account studies from the combination headache group (Table 4) where health-related quality of life (HRQoL) was assessed in migraineurs.
Newcastle-Ottawa Scale: S: selection; C: comparability; O: outcome; T: total.
QoL: quality of life; EM: episodic migraine; CM: chronic migraine; HIT-6: Headache Impact Test; MIDAS: Migraine Disability Assessment Scale; SF-36: Short Form 36; TAS-20: Toronto Alexithymia Scale-20; STAI: State and Trait Anxiety Scale; BDI: Beck Depression Inventory; FSS: Fatigue Severity Scale; EDSS: Expanded Disability Status Scale; MSQol-54: Multiple Sclerosis Quality of Life 54; CDI: Children’s Depression Inventory; ASI: Adolescent Symptom Inventory; PedsQL: Pediatric Quality of Life Inventory version 4.0; MIGSEV: Migraine Severity Scale; QVM: Qualité de Vie et Migraine; HADS: Hospital Anxiety and Depression Scale; WHO-DAS II: World Health Organization Disability Assessment Schedule; ICF: International Classification of Functioning, Disability and Health; MINI: Mini International Neuropsychiatric Interview; EDI-II: Eating Disorder Inventory; MSQ: Migraine Specific Quality of Life Questionnaire; PGWB: Psychological General Well-being schedule; SSAP: Subjective Symptom Assessment Profile; MSEP: Minor Symptom Evaluation Profile; SDS: Self-Rating Depression Scale; HANA: Headache Needs Assessment; PHQ-4: Patient Health Questionnaire 4-items; RAND-36: RAND-36 Item Health Survey questionnaire; PRIME-MD: Primary Care Evaluation for Mental Disorders; CES-D: Center for Epidemiologic Studies-Depression Scale; CSQ: Coping Strategies Questionnaire; CPEI-H: Chronic Pain Experience Instrument-Headache; MPQ-SF: McGill Pain Questionnaire-Short Form; HDI: Henry Ford Headache Disability Inventory; BAI: Beck Anxiety Inventory; PCS: Pain Catastrophizing Scale.
Comparisons of HRQoL to asthmatics showed that migraineurs scored significantly lower on social functioning, role emotional, mental health, bodily pain and vitality domains of the SF-36 scale. However, compared to patients with chronic musculoskeletal pain and juvenile fibromyalgia, migraineurs had better overall HRQoL (42,70). Similarly, children with primary headache disorders scored significantly worse on all aspects of HRQoL, except physical functioning and general health perception subscales of the SF-36 scale, when compared to children with asthma, and had generally worse HRQoL than children with attention deficit hyperactivity disorder (ADHD) (72). In comparison to hypertension, diabetes and osteoarthritis, migraineurs scored lower in most SF-36 domains, particularly those measuring well-being (mental health, emotional and social functioning) (46,73).
This impairment in HRQoL is also reflected in studies using migraine-specific HRQoL and headache disability scales. There was a decrease of more than 20 points in all three domains of the MSQ scale (role restrictive, role preventive and emotional functioning) between migraineurs and controls (37). Twenty-eight studies used the MIDAS questionnaire, and eight of 13 studies that reported MIDAS grades found that more than half of migraineurs (14,23,25–28,34,67,71) were moderately to severely disabled by their headaches (MIDAS grades III and IV). This was also seen in two of six studies assessing headache disability using the HIT-6 scale (19,35). However, migraineurs tend to attend school or paid work despite their headache, with more days of reduced productivity at school or work than actual days of missed activity (14,16,25,47,62,65,67,68,71,74). There was also a trend of more missed days reported for household work, followed in order by family, social and leisure activities and school or paid work, respectively. Days of reduced productivity by at least half in household chores were also greater than in school or paid work (14,16,25,47,55,62,67,68,71,74).
Two studies evaluated HRQoL impairment in groups of employed individuals with migraine, namely nurses and French workers. The nurses suffering from migraine showed lower HRQoL compared with non-headache participants, especially in the physical role and bodily pain subscales of the SF-36 scale, which are sensitive to headache severity. Consequently, this affected their work, leading to missed workdays, arriving late, and reduced function and productivity at work (38). Conversely, a comparative study among French workers showed that absenteeism among migraine sufferers was not statistically different from controls, although performance was greatly reduced, which was in agreement with the findings from the above studies (40).
The tendency of missing family time over paid work can lead to disruption in family relationships. This was found to be a central issue raised by patients and relatives in a study, whereby both viewed that family environment was the area most affected by migraines (65). Patients and their spouses also expressed their concern regarding the impact of migraines on the emotional development of their children (65). Indeed, a study exploring the relationship between maternal migraine and child functioning found that migraine may be related to dysfunctional parenting patterns, with the risk of parent-child reversal roles and inappropriate parents’ expectation of their children increasing as a mother’s migraine becomes disabling (56).
With regards to migraine among the pediatric and adolescent population (48,54,70,66), there was an overall impairment in HRQoL domains. Adolescents reported more impairment in school functioning, whereas social functioning was reportedly more impaired in younger children (aged 5–7 years) (66,70). Adolescent autonomy and coping mechanisms play a significant role in determining HRQoL; the more able a child is in coping with pain, the better the HRQoL. Moreover, having a successful adaptive family routine, whereby families adapt and organize their daily activities in a positive way for all members, predicts a better outcome for HRQoL (75,76).
In view of the emotional and mental impairments associated with migraine, much attention has been focused on the association between psychological well-being and HRQoL (13,18,20,22,48,50,53,60,61,64,70,77). These studies showed that most migraineurs exhibited anxiety and/or depressive symptoms, and comorbidity with both anxiety and depression was positively correlated to headache-related disability (22,77). These psychiatric disorders have a negative influence on HRQoL independent of each other; however, migraineurs with combined anxiety and depression have significantly poorer HRQoL scores, with the greatest impact being on the mental health domains of the SF-36 scale (22,48,60). The presence of these affective disorders also affects perceived migraine, treatment satisfaction and efficacy (22). Conversely, no differences were reported in HRQoL scores between migraineurs with and without comorbid psychiatric disorders (53). Moreover, it has been suggested that the psychological response to severe migraine, particularly catastrophizing, has a greater impact on HRQoL impairment than the mere presence of comorbid anxiety and/or depression (13).
TTH
Studies of quality of life in tension-type headache.

These are studies that have focused specifically on tension-type headache; however, our overall tension type headache group (26 in total) also took into account studies from the combination headache group (Table 4) where health-related quality of life (HRQoL) was assessed in tension-type headache.
Newcastle-Ottawa Scale: S: selection; C: comparability; O: outcome; T: total.
QoL: quality of life; ETTH: episodic tension-type headache; VAS: visual analog scale; CTTH: chronic tension-type headache; MOS: Medical Outcomes Study; SF-36: Short Form 36; SF-20: Short Form 20; BDI: Beck Depression Inventory; STAI: State and Trait Anxiety Scale; PRIME-MD: Primary Care Evaluation for Mental Disorders; RIIR: Recurrent Illness Impact Recording; MIDAS: Migraine Disability Assessment Scale.
This is in line with the finding that even though the majority of CTTH patients had a generalized impairment in functioning, which persists even outside of attacks (12), this was usually of moderate severity, without necessarily forcing cancellations of work or social commitments. Only a minority (up to 6%) rated their work performance as severely impaired and only 9% reported severe impairment in social functioning (19,76). The greatest impairment was related to sleep, energy levels and emotional well-being (76). The degree of impairment in TTH is comparable to or greater than those with back problems or arthritis (76).
Anxiety or mood disorders were found to be three to 15 times as frequent in CTTH patients as controls (76). The observed depression was mild to moderate in severity; however, anxiety was sufficiently high to impair functioning (76). The association between anxiety/depression and HRQoL in CTTH was investigated in one study, which suggested that anxiety has a mediating effect between headache frequency and vitality, social functioning and mental health, while depression had a modulatory effect on these same domains (45).
CH
Studies of quality of life in cluster headache.

These are studies that have focused specifically on cluster headache; however, our overall cluster headache group (nine in total) also took into account studies from the combination headache group (Table 4) where health-related quality of life (HRQoL) was assessed in cluster headache.
Newcastle-Ottawa Scale: S: selection; C: comparability; O: outcome; T: total.
QoL: quality of life; CH: cluster headache; ECH: episodic cluster headache; CCH: chronic cluster headache; SF-36: Short Form 36; HIT: Headache Impact Test; HADS: Headache Anxiety and Depression Scale.
Combination headache types.

Newcastle-Ottawa Scale: S: selection; C: comparability; O: outcome; T: total.
QoL: quality of life; HRQoL: health-related quality of life; CCH: chronic cluster headache; ECH: episodic cluster headache; TTH: tension-type headache; ETTH: episodic tension-type headache; CTTH: chronic tension-type headache; CDH: chronic daily headache; CH: cluster headache; EM: episodic migraine; CM: chronic migraine; RCMAS: Revised Children’s Manifest Anxiety Scale; HIT-6: Headache Impact Test; MIDAS: Migraine Disability Assessment Scale; SF-36: Short Form 36; TAS-20: Toronto Alexithymia Scale-20; RCADS: Revised Child Anxiety and Depression Scale; MOS: Medical Outcomes Study; CALI: Child Activity Limitations Interview; STAI: State and Trait Anxiety Scale; ARCS: Adults’ Response to Children’s Symptoms; BDI: Beck Depression Inventory; FAD: The McMaster Family Assessment Device; PADM: Perspectives on Adolescent Decision-making Questionnaire; FSS: Fatigue Severity Scale; EDSS: Expanded Disability Status Scale; MSQol-54: Multiple Sclerosis Quality of Life 54; CDI: Children’s Depression Inventory; ASI: Adolescent Symptom Inventory; PedsQL: Pediatric Quality of Life Inventory version 4.0; MIGSEV: Migraine Severity Scale; QVM: Qualité de Vie et Migraine; HADS: Hospital Anxiety and Depression Scale; GDS-S: Geriatric Depression Scale-Short Form; WHO-DAS II: World Health Organization Disability Assessment Schedule; ICF: International Classification of Functioning, Disability and Health; MINI: Mini International Neuropsychiatric Interview; EDI-II: Eating Disorder Inventory; MSQ: Migraine Specific Quality of Life Questionnaire; PGWB: Psychological General Well-being schedule; SSAP: Subjective Symptom Assessment Profile; MSEP: Minor Symptom Evaluation Profile; SDS: Self-Rating Depression Scale; HANA: Headache Needs Assessment; PHQ-4: Patient Health Questionnaire 4-items; RAND-36: RAND-36 Item Health Survey questionnaire; PRIME-MD: Primary Care Evaluation for Mental Disorders; CES-D: Center for Epidemiologic Studies-Depression Scale; CSQ: Coping Strategies Questionnaire; CPEI-H: Chronic Pain Experience Instrument-Headache; MPQ-SF: McGill Pain Questionnaire-Short Form; HDI: Henry Ford Headache Disability Inventory; BAI: Beck Anxiety Inventory; PCS: Pain Catastrophizing Scale; KINDL-R: Revidierter Kinder Lebensqualitatsfragebogen score; SOPA-35: Survey of Pain Attitudes; NDI: Neck Disability Index; YSR: Youth Self-Report; ADI: Assessment of Depression Inventory; CHQ-PF50 Dutch version; Dutch version of the Child Health Questionnaire; NHP: Nottingham Health Profile; CHQQ: Comprehensive Headache-related Quality of life Questionnaire.
Abbreviations
BDI: The Beck Depression Inventory; CES-D: Center for Epidemiologic Studies-Depression Scale; CHQ-PF50 Dutch version: Dutch version of the Child Health Questionnaire; CIRS: Cumulative Illness Rating Scale; CPEI-H: Chronic Pain Experience Instrument-Headache; CSQ: Coping Strategies Questionnaire; EDI: Eating Disorder Inventory; HAMA: Hamilton Anxiety Scale; HANA: Headache Needs Assessment; HDI: Henry Ford Headache Disability Inventory; ISSL: Lipp’s Inventory of Stress Symptoms for Adults; MADRS: Montgomery and Asberg Depression Scale; MIDAS: Migraine Disability Assessment Questionnaire; MPQ-SF: McGill Pain Questionnaire-Short Form; MRQoL: Migraine-Related Quality of Life Questionnaire; MSEP: Minor Symptom Evaluation Profile; MSQ: Migraine Specific Quality of Life Questionnaire; SSAP: The Subjective Symptom Assessment Profile; MSQ v.2.1: Migraine Specific Quality of Life Questionnaire version 2.1; NDI: Neck Disability Index; PGWB: Psychological General Well-being schedule; PRI = Pain Response Inventory; QVM: Qualité de Vie et Migraine; PCS: Pain Catastrophizing Scale; PRIME-MD: Primary Care Evaluation for Mental Disorders; HAMD: The Higher Hamilton Depression Rating Scale; HADS: Hospital Anxiety and Depression Scale; KINDL-R: Revidierter Kinder Lebensqualitatsfragebogen score; MINI: The Mini International Neuropsychiatric Interview; QLH-Y: The Quality of Life Headache-Youth; NHP: Nottingham Health Profile; VAS: Visual Analog Scale; PedsQL 4.0: The Pediatric Quality of Life Inventory version 4.0; STAI: State and Trait Anxiety Scale; QWB: The Quality Well-being scale; RAND-36: RAND-36 Item Health Survey questionnaire; GDS-S: Geriatric Depression Scale-Short Form; SOPA-35: Survey of Pain Attitudes; PAQ: Patient Assessment Questionnaire; SF-20: Short Form 20-item Health Survey; MIGSEV: Migraine Severity Scale; CSEI: Coopersmith Self-Esteem Inventory; SDS: Self-Rating Depression Scale; BAI: Beck Anxiety Inventory; HIT-6: Headache Impact Test; SF-36: Short Form 36-item Health Survey; CFH: Chronic frequent headache; IH: intermittent headache; MDD: major depressive disorder; EM: episodic migraine; CM: chronic migraine; ETTH: episodic tension-type headache; CTTH: chronic tension-type headache; CH: cluster headache; ECH: episodic cluster headache; CCH: chronic cluster headache; CDH: chronic daily headache; PHQ: Patient Health Questionnaire 4-items; BHS: Brief Headache Screen; PHQ-9: Patient Health Questionnaire Depression Scale; GAD-7: Generalized Anxiety Disorder 7-item Scale; WHO-DAS II: World Health Organization Disability Assessment Schedule; EFI: Ecocultural Family Interview; RIIR: Recurrent Illness Impact Recording; ICF: International Classification of Functioning, Disability and Health; ASI-4: Adolescent Symptom Inventory; CDI: Children’s Depression Inventory; HDHCQ: Headache Disability and Health Care Questionnaire; CPCI: Chronic Pain Coping Inventory; MOS: Medical Outcomes Study; RCADS: Revised Child Anxiety and Depression Scale; CALI: Child Activity Limitations Interview; FAD: The McMaster Family Assessment Device; ARCS: Adults’ Response to Children’s Symptoms; PADM: Perspectives on Adolescent Decision-making Questionnaire.
Comparing the different forms of CH, there was no significant difference in HRQoL between ECH patients during a bout and CCH patients (51, 79). During the remission period of ECH patients, their HRQoL score tended to improve and became similar to headache-free groups (39). Conversely, Jürgens et al. (2010) (80) found that disability remained high in ECH patients outside the bout, despite the absence of pain, which they speculate may have arisen due to the lack of a specified time frame in the questionnaire used (HDI). Thus patients may have actually completed the questionnaire with their past bout in mind, rather than in their current headache-free condition. However, 13% of patients in another study also reported inhibition outside the cluster bout (81), therefore raising the possibility that there is indeed a degree of impairment that continues beyond the cluster bout that could be attributed to unpredictability of the next bout, though further studies are required to confirm this.
Evaluation of the functional impact of CH showed that 74% were severely affected (HIT-6 grade IV disability) (36), with 78% reporting restrictions in daily living and 96% having to make some form of lifestyle change (81). Social and leisure activities, family life and housework were disrupted, with a high dependence placed on family and friends. In terms of paid work, 82% reported reduced ability to work, 16% lost their job and 8% had to retire early because of their headaches. Moreover, up to a third found that the disorder limited their career (80,81). Taking into account this significant disability and the pain severity, it is therefore not surprising that agoraphobic and depressive symptoms, and suicidal tendencies are more prevalent in CCH (36,80), with 33% reporting agoraphobia, 56% reporting depression and 22% having suicidal tendencies (36,80).
CDH
CDH is not a specific headache entity but is a term often used to describe any headaches that occur on 15 or more days per month, for at least three months. The most common types of CDH are chronic migraine (CM) and CTTH (5). Twenty-three studies were identified that evaluated HRQoL in CDH (12,36,45,51,52,72,76,77,78,80–85).
These studies demonstrate that patients with CDH have poorer HRQoL compared to the general population and patients suffering from severe episodic headache disorders (12,20,21,48–50,83). Studies using the SF-36 scale reported that mental health was markedly impaired, with reports of feeling irritated, fed up, frustrated and a tendency to give up (83). Role physical, social functioning, role emotional, general health and vitality domains in CM were significantly reduced compared to EM, with higher levels of depressive symptomatology exhibited (48). Three studies used the MSQ scale to compare EM and CM and two of three studies reported a decrease of more than six points in all domains (20,21). This impaired functioning correlates with the greater disability reported in CDH compared to their episodic counterpart, with reduced productivity at school and home (20,52,59). Headache frequency and comorbid depression has been found to have an independent and additive influence on HRQoL in CDH (50).
HRQoL across headache diagnoses
Sixteen studies compared HRQoL between primary headache types as shown in Table 4. These studies showed no significant differences in HRQoL between migraine and TTH (43,72,84,85), suggesting that the greater pain intensity of EM is counterbalanced with the greater frequency of CTTH (84). Although there is little variation in HRQoL between these headache groups, migraineurs report greater disability due to their headaches compared to TTH (19,31–33,40), especially in work or school functioning (37). More missed days at school or work were reported by migraineurs, whereas reduced productivity at school or work was more prevalent among TTH patients (38,59,82,84).
Solomon and colleagues (1994) used the SF health survey and found that CH patients had significantly worse pain scores with limited social functioning compared to the other groups, although physical functioning was preserved. On the other hand, migraineurs had the least pain with greatest impairment in role functioning. Meanwhile patients with CTTH had reduced mental health scores with a generalized impairment in functioning (78). Furthermore, although HRQoL is lower in patients with CH compared to healthy controls, in comparison to migraineurs, their HRQoL is lower in two SF-36 domains only; bodily pain and social functioning (39). Nonetheless CCH patients and ECH patients in a bout were found to be more disabled and incapacitated than migraineurs (80).
Factors that may influence HRQoL
Understanding the factors that influences HRQoL may enable us to manage and improve patients’ symptoms and subsequently their HRQoL. Headache characteristics such as pain intensity (19,24,28,32,35,55,57,63), duration (75,90) and (32,90) frequency (29,32,35,42,50,59,60,75) were found to be significant predictors of HRQoL. Likewise, presence of migrainous symptoms, particularly nausea, were also found to be important predictors in HRQoL (16,36,47,51,58), whereas combined photophobia and phonophobia are predictors of missed activity due to a headache (54). Greater headache-related disability was also a significant predictor of poor HRQoL (15). Comorbidity with other pain conditions negatively influences HRQoL (30,91). Furthermore, the patients’ psychological response to the pain experience and their coping mechanism has a great influence on HRQoL, and potentially may have a role in headache progression (13,35,75). Psychiatric comorbidity is associated with poorer HRQoL, with comorbid depression shown to have an independent and additive influence on headache-related disability (50). In CH, impairment worsened with increasing clinical severity and refractoriness of the headaches (80). However, it is important to note that even though all these factors can affect HRQoL, there is a marked individual impact, thus each patient will respond uniquely to these predicted factors.
Discussion
This review summarizes the results of 80 papers on HRQoL of the major primary headache disorders, namely migraine, TTH, CH and CDH. Most of the studies have focused on patients with migraine, with comparatively fewer studies performed on TTH and even less so on CH. Several studies conducted on migraineurs were deemed to be of good quality, with the remaining studies being mostly of moderate quality. In comparison, studies conducted on the other headache disorders were mainly of moderate quality only. Primary headache disorders and their effect on one’s ability to function in school, work or daily life in general, impose a burden not only on the sufferers’ themselves, but also on society, notably in terms of economic productivity and health care costs. Absenteeism and reduced work productivity, together with family and social restraints, can lead to disruptions in occupational and personal domains, potentially creating a vicious cycle with worsening of headache, thus increasing its negative impact on HRQoL.
This review found that patients with primary headache disorders have consistently diminished HRQoL across all headache categories, either compared with matched non-headache controls, or other chronic disorders. However, the degree and affected domains vary according to the headache type, frequency, associated symptoms and comorbidities. We also identified various factors that are associated with, and are likely to be predictors of, reduced HRQoL in headache sufferers.
The reduced HRQoL among migraineurs is a major concern, both because of its high prevalence in the general population and its prominent disabling nature, which can have a substantial economic impact (38,92–94). The greatest impairment reported was in role and social functioning, with reduced work productivity and absenteeism among migraineurs being well reported. Moreover, headache-related disability extends to household and family and social functioning, which can lead to disruption in social and family relationships.
With regards to TTH, although ETTH is the most prevalent headache disorder in the general population, most of the studies have focused on HRQoL in CTTH. This may be because the pain in ETTH is usually infrequent and mild, thus it is less likely to cause significant impairment. Even so, these studies indicate that TTH has a major impact on HRQoL, with a generalized impairment in functioning. HRQoL is significantly worse relative to healthy controls, and also relative to episodic migraine sufferers on some HRQoL domains. However, compared to migraineurs, patients with TTH report fewer missed days at school or work.
CH patients had reduced scores in most domains of the SF-36 scale and all domains of the MSQ scale compared to controls and patients outside a bout. Headache-related disability remained high even outside the cluster bout, with considerable impact on social and family life, having to frequently miss social events and family gatherings. Surprisingly, the effect of CH on HRQoL is less marked compared to migraineurs, though this should be treated with caution, as the sample sizes of these studies were small. Moreover, the lack of a specific CH HRQoL measure that can truly capture the inherent disabling and debilitating nature of this disorder may also account for the results seen. Nevertheless, this review found that their HRQoL is much more impaired compared to the general population. However, unlike migraine, this became comparable to healthy controls during remission periods (51).
Meanwhile, studies on CDH have mostly focused on CM and CTTH. To our knowledge, HRQoL in hemicrania continua and new daily persistent headache has not been assessed. There is significantly reduced HRQoL in patients with CDH compared to healthy controls and its episodic variant, suggesting that chronicity of the headache may contribute greatly to HRQoL.
Indeed, the frequency, duration and intensity of the headaches were found to be significant predictors of HRQoL. Moreover, a large proportion of the studies reviewed showed a high prevalence of anxiety and/or depressive symptoms in patients with primary headache disorders. A bidirectional association has been reported between first onset of migraine and major depression, and vice versa, although this relationship has not been found to extend to other types of severe headache (95). Thus, patients presenting with headaches should be evaluated for both their headache and any associated psychiatric comorbidity.
Review of the literature revealed that the majority of studies used generic HRQoL instruments. Although disease-specific instruments have been used to evaluate HRQoL in clinical trials, there were limited numbers in this review. This could be due to the exclusion of studies that tested the efficacy of medications. We were unable to interpret the data from these two measures separately as the general HRQoL measures may have been influenced by other comorbidities other than headaches, which were not specifically assessed in the studies. However, in general, studies showed there was moderate correlation (r > 0.4) between the generic and headache-specific HRQoL scales, indicating that there are measuring the same underlying construct i.e. HRQoL (69).
Some limitations that need to be considered with our interpretation are the greater number of studies with clinic population samples compared to community. Most of these were carried out in headache clinics, where patients seen were more likely to have severe and treatment-refractory headaches, which may have a greater impact on HRQoL. However similar findings were seen within the community sample. Secondly, studies on TTH and CH tended to have smaller sample sizes, which make comparisons across headache diagnosis difficult.
In conclusion, different types of headache affect different HRQoL domains. However, once it becomes chronic, the overall HRQoL significantly declines. Furthermore, there is an increased prevalence of psychological comorbidity in headache disorders that affects HRQoL and thus needs to be recognized. This highlights the importance of increasing clinical awareness, in an attempt to better manage these headaches earlier in its course, thereby preventing its transformation to a chronic variant. Although to date there have been a number of studies assessing HRQoL in headache disorders, there are several issues that require further exploration. Firstly, disease-specific HRQoL instruments have been developed only for migraine. As previously mentioned, TTH and CH have different headache characteristics compared to migraine, thus specific instruments need to be developed to truly capture the impact of these disorders. Secondly, there are only a handful of studies focusing on ETTH, which is the most common type of headache, and CH, which is considered to be one of the most painful conditions known to mankind. HRQoL and psychiatric morbidity in these disorders need to be explored further. Lastly, it is evident from the studies reviewed that any type of headache can impair HRQoL. A direct comparison of HRQoL across different headache types would be of interest in future studies.
Clinical implications
Primary headache disorders significantly diminish quality of life, with degree of impairment being dependent on headache type. There is a high prevalence of psychological comorbidity associated with headache disorders, which affects quality of life. Most of the studies have focused on migraine, with little attention to other types of primary headache disorders. Hence, disease-specific quality of life questionnaires have been developed only for migraine and may not be sensitive enough to capture the true effects of the other headache types. Further studies on the other headache types should be considered.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
ST, NAB, GL, MT and MJ have nothing to declare. MSM serves on the advisory board for Allergan and St Jude Medical, and has received payment for the development of educational presentations from Allergan, Merck Sharpe and Dohme Ltd and Medtronic.