
Abstract
Background:
The International Headache Society defines Occipital neuralgia as an unilateral or bilateral paroxysmal, shooting or stabbing pain in the posterior part of the scalp, in the distribution(s) of the greater, lesser and/or third occipital nerves. The most common pain trigger in this area result from chronically contracted muscles. Different aetiologies of headache with occipital neuralgia phenotype have been described.
Case:
We report four cases in which pain with occipital neuralgia phenotype was the initial symptom of a clivus chordoma; a para-pharyngeal carcinoma; a vertebral dissection; and a brachial plexitis due to zoster.
Conclusion:
A detailed anamnesis and physical examination should be performed in these patients. If during follow up atypical finding appears, we recommend head and neck gadolinium-enhanced MRI and biochemistry to exclude secondary causes.
Keywords
Introduction
The International Headache Society defines Occipital neuralgia as an unilateral or bilateral paroxysmal, shooting or stabbing pain in the posterior part of the scalp, in the distribution(s) of the greater (GON), lesser (LON) and/or third occipital nerves. 1 The most common pain trigger in this area result from chronically contracted muscles. Different aetiologies of headache with occipital neuralgia phenotype have been described. Abnormalities in general and/or neurological examination must raise the suspicion for underlying causes. Different aetiologies have been described 2 (Table 1). We report findings in four patients with secondary headache with occipital neuralgia phenotype evaluated between 2007 and 2018, at the Headache Clinic of FLENI, a tertiary neurological referral centre in Buenos Aires.
Occipital neuralgia: Secondary causes reported.
Case reports
Patient 1
A 73-year-old female without medical history of headache consulted for a severe paroxysmal burning pain in the right occipital region of 3 months of evolution. The attack lasted up to 2 min, occurred over five times a day and woke her up from sleep. She had been treated with different non-steroidal anti-inflammatory drugs without response. Physical examination revealed asymmetrical palate elevation with dysesthesia and pain in the GON and LON regions. Anesthesic occipital nerves block with 2% lidocaine were made with 80% reduction of pain. The abnormalities in physical examination raised de suspicion of a secondary aetiology. Magnetic Resonance Imaging (MRI) of the brain and neck revealed an expansive para-pharyngeal lesion infiltrating the clivus and petrous temporal bone, with heterogeneous contrast enhancement (Figure 1). Lesion biopsy was informed as a differentiated squamous cell carcinoma. Surgical resection was made and radiotherapy was started. Occipital pain was partially relived.

Axial gadolinium-enhanced cranial T1 weighted MRI showing expansive para-pharyngeal lesion infiltrating the clivus, showing heterogeneous contrast enhancement.
Patient 2
A 48-year-old female, without relevant medical history, presented to the hospital with a 3-week history of headache with paroxysmal exacerbations of burning pain in the right occipital region. A few days before the headache onset she had cough and nasal congestion. She had no previous history of headache. Hyperesthesia in right occipital area was present at physical examination. With the suspicion of secondary headache a brain MRI was performed
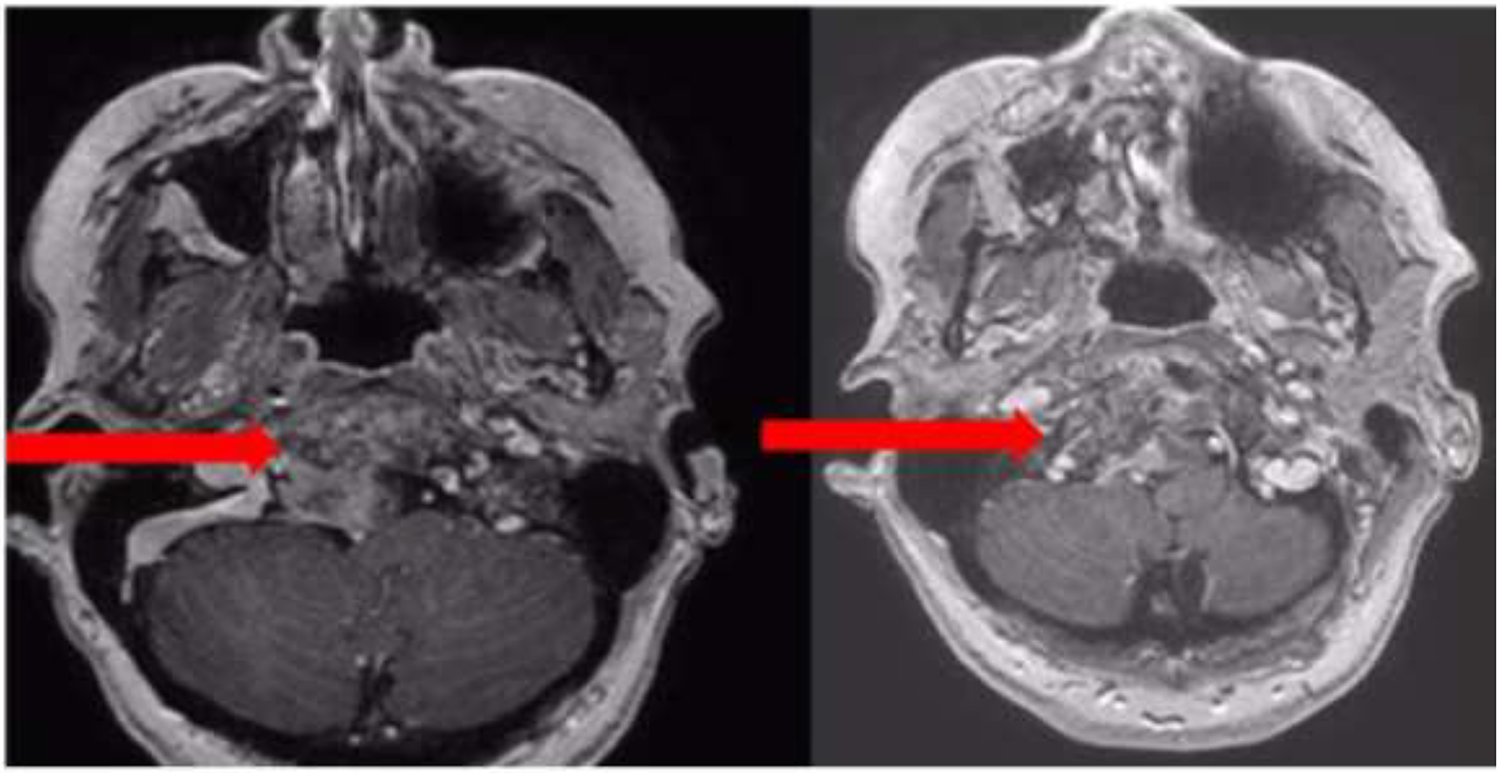
Brain MRI angiogram showed blood and narrowing in the arterial right vertebral wall suggesting dissection (Figure 2). She was treated with aspirin 100 mg/day, rosuvastatin 20 mg/day and enalapril 5 mg/day, with clinical improvement.

Left: Axial cranial T1 weighted MRI showing hematoma in the arterial wall. Right: MR angiography showing narrowing of the lumen of the right vertebral artery.
Patient 3
A 75-year-old female complained of a 6-day history of severe sharp, stabbing headache located in the left occipital region. Her past medical history included migraine, mild occipital headache which disappeared after menopause, glaucoma, thyroidectomy for a benign nodule and surgical resection of a melanoma on the right thigh, for which no chemotherapy was given. Patient was currently disease-free, receiving levothyroxine, calcium and vitamin D. Neurological examination showed pain could be elicited by pressure on the point of distribution areas of GON. Cranial MRI and intra-extracranial MR angiogram showed no abnormalities. GON and LON blockade with lidocaine was performed with partial relief. Occipital neuralgia was diagnosed at that moment.
In the following 5 days, she developed vesicular rash over the distribution of the fifth cervical nerve (C5). Five days later she experienced proximal weakness of the left arm and was admitted to hospital, where treatment with acyclovir was started.
Cerebrospinal fluid assay showed 3 cells/µl, protein level at 46.7 mg/dl and normal glucose concentration. PCR for Herpes Simplex Virus type I, II, VI and Varicella Zoster Virus were negative. New cranial and cervical MRI with gadolinium enhancement only showed degenerative disc disease. An electromyogram indicated proximal neurogenic defect on left fifth and sixth cervical nerve (C5-C6) metameres, suggestive of upper brachial plexus trunk lesion. Brachial plexus MRI revealed hyperintensity on T2-weighted sequences and homogeneous gadolinium enhancement in the right root of C5 and in the upper trunk of the brachial plexus (Figure 3). Plexitis due to Herpes zoster was diagnosed. Patient evolved with improvement in muscle strength, but persistence of pain and local paresthesias, and was treated with pregabaline.

Brachial plexus MRI revealed hyperintensity on T2-weighted sequences (left) and homogeneous gadolinium enhancement (right) of the right C5 nerve root and the upper trunk of the brachial plexus.
Patient 4
The patient, a 64-year-old female with rheumatoid arthritis treated with methotrexate and folic acid for 10 years, dyslipidemia, arterial hypertension, and no headache history, presented with dysesthesias and paroxysmal pain in the right occipital region during the last 2 months. She also referred episodes of dysarthria lasting 3 minutes while brushing her teeth in the last week.
Examination revealed deviation of the tongue to the right and allodynia along the distribution of the GON; and LON on right side also. Forward flexion of the neck triggered dysarthria lasting under 5 min.
Brain MRI revealed a mass on FLAIR sequence involving the clivus with heterogeneous gadolinium enhancement, extending to the right prepontine cistern, suggestive of chordoma (Figure 4).
Axial gadolinium-enhanced cranial T1 weighted MRI showing a heterogeneous mass involving the clivus with occupation of the right peribulbar cistern and mass effect with displacement of the medulla oblongata to the left in a posterolateral direction.
She got positive response to GON and LON blocks. Diagnosis of secondary neck-tongue syndrome and pain with occipital neuralgia phenotype were made.
Surgery was performed and chordoma was confirmed on the specimen pathology report.
Discussion
Occipital neuralgia is defined as an unilateral or bilateral severe, paroxysmal pain in the distribution(s) of the greater, lesser and/or third occipital nerves. It can be shooting, stabbing or sharp in quality and is associated with dysaesthesia, allodynia or tenderness of the scalp and/or hair. There can be trigger points at the emergence of GON and pain is eased temporarily by local anaesthetic block of the affected nerve(s). The International Headache Society defined diagnostic criteria for Occipital neuralgia. 1
Occipital pain may result from multiple causes. Several occipital and suboccipital structures such as vessels, dura mater of the posterior fossa, deep paraspinal neck muscle, and zygapophyseal joints are recognized as sources of head and neck pain. 2 Nociceptive inflow from these suboccipital structures is mediated by afferent fibres in the upper cervical roots terminating in the dorsal horn of the cervical spine extending from the C2 segment up to medullary dorsal horn. 3
In these four cases, pain with occipital neuralgia phenotype was the main initial symptom.
The pain in the first patient had similar characteristics to occipital neuralgia, but had an abnormal physical examination. An MRI showed a pharyngeal carcinoma probably not expected by the pain localization and not fulfilling diagnostic criteria of Headache or facial pain attributed to disorder of the cranium, neck, eyes, ears, nose, sinuses, teeth, mouth or other facial or cervical structure of ICHD-3. 1 The literature describes several cases of infiltrative cervical lesions causing symptomatic occipital neuralgia, either with or without atypical findings in physical examination. 2
The second one had an artery dissection in which the only manifestation was paroxysmal occipital pain instead of a characteristic continuous cervical pain that has been describe in the criteria Headache or facial or neck pain attributed to cervical carotid or vertebral dissection in the ICHD-3 criteria. 4 Most of the cases of vertebral dissection have another symptoms apart from pain. Only 10.8% of vertebral dissection have headache as the only manifestation. 4
The pain in the third patient fulfilled diagnostic criteria of occipital neuralgia, at the beginning. The development in the following days of an extensive zoster infection with included C5 branches lead to another final diagnostic. The case shows the importance of the close follow up of patients with pain in the occipital area. To our knowledge only a few cases of Occipital neuralgia as manifestation of herpes zoster infection have been described. 5
The last case was paroxistic occipital pain, with combination of neck-tongue syndrome. Thirty-nine cases were reported with neck sensory symptoms and in the ipsilateral tongue, as moving the head, and atlanto-axoid joint luxation was pointed as one possible aetiology. 6
Finally to mention that some occipital neuralgias are sometimes superposed in real life patient, despite International Classification of Headache Disorder third edition, even in experimented Tertiary Headache Centers. Probably most of these cases will undergo nerve blocks at first attempt.
Conclusions/final considerations
In patients who refer paroxistic or excruciating pain in the occipital region, detailed anamnesis and complete physical examination are strongly recommended, although the first clinical impression may be an occipital neuralgia. In case any of these are abnormal, we recommend performing gadolinium-enhanced MRI of the head and neck and complete blood analysis, even if peripheral nerve block gives some relief.
These patients should be controlled periodically in search of any atypical pain feature and/or physical examination abnormalities, which when present, should raise suspicion of an underlying aetiology other than muscle contraction.
Clinical implications
In patients who refer new paroxistic pain in the occipital region, a detailed anamnesis and complete physical examination is mandatory.
Even when paroxistic occipital pain has a good response to anesthesic occipital nerve block close follow up is recomended
In case of atypical presentation, we recommend performing gadolinium-enhanced MRI of the head and neck and complete blood analysis, even if peripheral nerve block gives some relief.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics or institutional review board approval
The study obtained appropriate approval of the ethics committee review board of our institution
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.