
Abstract
Background: Greater occipital nerve stimulation (ONS) has been recently proposed to treat severe chronic cluster headache patients (CCH) refractory to medical treatment. We report the results of a French multidisciplinary cohort study.
Methods: Thirteen CCH patients were operated and data were collected prospectively. All of them suffered from CCH according to the International Headache Society classification, lasting for more than 2 years, refractory to pharmacological prophylactic treatment with adequate trials, with at least one daily attack. Chronic ONS was delivered through a subcutaneous occipital electrode connected to an implanted generator, in order to induce paraesthesias perceived locally in the lower occipital region.
Results: After surgery (mean follow-up 14,6 months), the mean attack frequency and intensity decreased by 68% and 49%, respectively. At last follow-up, 10/13 patients were considered as responders (improvement >50%). Prophylactic treatment could be stopped or reduced in 8/13 cases. Local infection occurred in one patient, leading to hardware removal.
Conclusions: Our data confirmed the results of the 36 similar cases reported in the literature, suggesting that ONS may act as a prophylactic treatment in chronic CH. Considering their respective risks, ONS should be proposed before deep brain stimulation in severe refractory CCH patients.
Introduction
Cluster headache (CH) is a primary headache and belongs to the group of the trigeminal autonomic cephalalgias in the International Classification of Headache Disorders (1). CH is characterized by strictly unilateral short-lasting pain attacks associated with prominent parasympathetic features. Chronic CH (CCH) is diagnosed after 1 year without remission or with remission periods lasting less than 1 month (1). CH is one of the most painful conditions in humans and is often referred to as ‘suicidal headache’. For patients with severe CCH refractory to medical prophylactic treatment, several lesioning procedures have been tried in the past, without satisfactory long-term relief of pain.
Deep brain stimulation (DBS) of the retro-hypothalamic region has been used by several teams, with a satisfactory reduction of attacks in about 60% of the cases (2,3). However, this procedure is invasive and exposes the patients to the risk of intra-cerebral haemorrhage. Greater occipital nerve stimulation (ONS) has been proposed since 1999 to treat some chronic headache and cervical pain (4), and since 2007 to treat severe CCH (5,6). However, few data are available, as only 36 cases have been reported so far for CCH (5–9). We report the experience of a French multidisciplinary network involved in primary headache management.
Methods
All the patients enrolled in the study fulfilled the criteria considered by a panel of international CH experts as mandatory for proposed DBS in CCH (10): chronic CH according to ICHD-II criteria (1); disease duration over 2 years; resistance to pharmacological prophylactic treatment with adequate trials; at least one daily attack. Patients were enrolled and operated on after complete information about the procedure. The patients were given implants on compassionate grounds and the study was an audit of outcome, and as such under French guidelines did not require ethics committee approval. Patients with alcohol abuse or abnormal findings on brain magnetic resonance imaging, which are considered as contra-indication for DBS, could be enrolled. Patients’ evaluation was common in the three centres participating in the study and data were collected prospectively. All the centres assigned a neurological team (belonging to the ‘Observatoire des Migraines et Céphalées’ set up by the French Headache Society (11)) to manage the recruitment and evaluation of the patients and a neurosurgical team highly qualified in the neuromodulation in charge of the hardware implantation and setting.
Operative techniques usually performed for ONS were not changed for this study and consequently differed slightly among the participating centres concerning the type of electrode and surgical approach. However, in all the cases, a quadripolar electrode (Resume electrode in four cases; Quad electrode in four cases, Medtronic, Minneapolis; and Lamitrode 44 St Jude-ANS in five cases) was introduced subcutaneously next to the great occipital nerve under general anaesthesia and then connected to a stimulator (Itrel III, Medtronic or Genesis St Jude-ANS). Stimulation parameters were adjusted individually in order to induce paraesthesias, which is usually considered to be mandatory to obtain the therapeutic effect. The paraesthesias induced by the chronic bilateral stimulation were perceived locally in the lower occipital region and upper neck in nine cases and expanded in the upper occipital region in 4 cases. Mean stimulation settings were the following: amplitude 3.5 volts (range 2.8–4.6), frequency 57.5 Hz (range 50–70), pulse width 247.5 μs (range 210–450).
Clinical evaluation was performed before and every 3 months after surgery, according to the data collected in a diary used by the patient during the month preceding the visit. At each evaluation, clinical data collected were: number of attacks during the past week (calculated from the individual patient’s diary), mean attack intensity according to a numeric rating scale, and occurrence of any adverse effects. At each visit after surgery, patients had to evaluate the percentage of global improvement compared with baseline and to answer the question ‘would you recommend the operation to a fellow cluster headache sufferer?’. Data were analysed using SPSS software (SPSS Inc, v11, Chicago). The frequencies of attacks before and after surgery (at months 3, 6 and 12) were compared using the Wilcoxon test for paired data. The same test was used to compare the mean intensities of attacks before and after the operation. The significance level was set at p = 0.05.
Results
Fourteen patients were enrolled and operated on between March 2008 and July 2010. One patient moved to another region and was lost to the study less than 3 months after surgery. Thirteen patients were followed for a mean duration of 14.6 months (range 3–34 months). Preoperative clinical characteristics of these 13 patients are shown in Table 1. Ten out of 13 patients experienced a significant improvement within a few days after surgery (Figure 1). In two patients, the improvement was delayed (by 1 and 5 months, respectively) and maintained over time. One patient never improved and was explanted 6 months after surgery but was followed regularly and has been considered in the results in ‘intention to treat’ analysis.
Box-and-whisker plot showing the distribution of weekly attack frequencies with time. The boxes indicate the inter-quartile range; the whiskers indicate the lowest and the highest datum. *p values for the differences from baseline (preoperative) using the Wilcoxon test for paired data. M, month. Preoperative clinical characteristics of the 13 patients L: left side, R: right side, B: bilateral related to changing sides.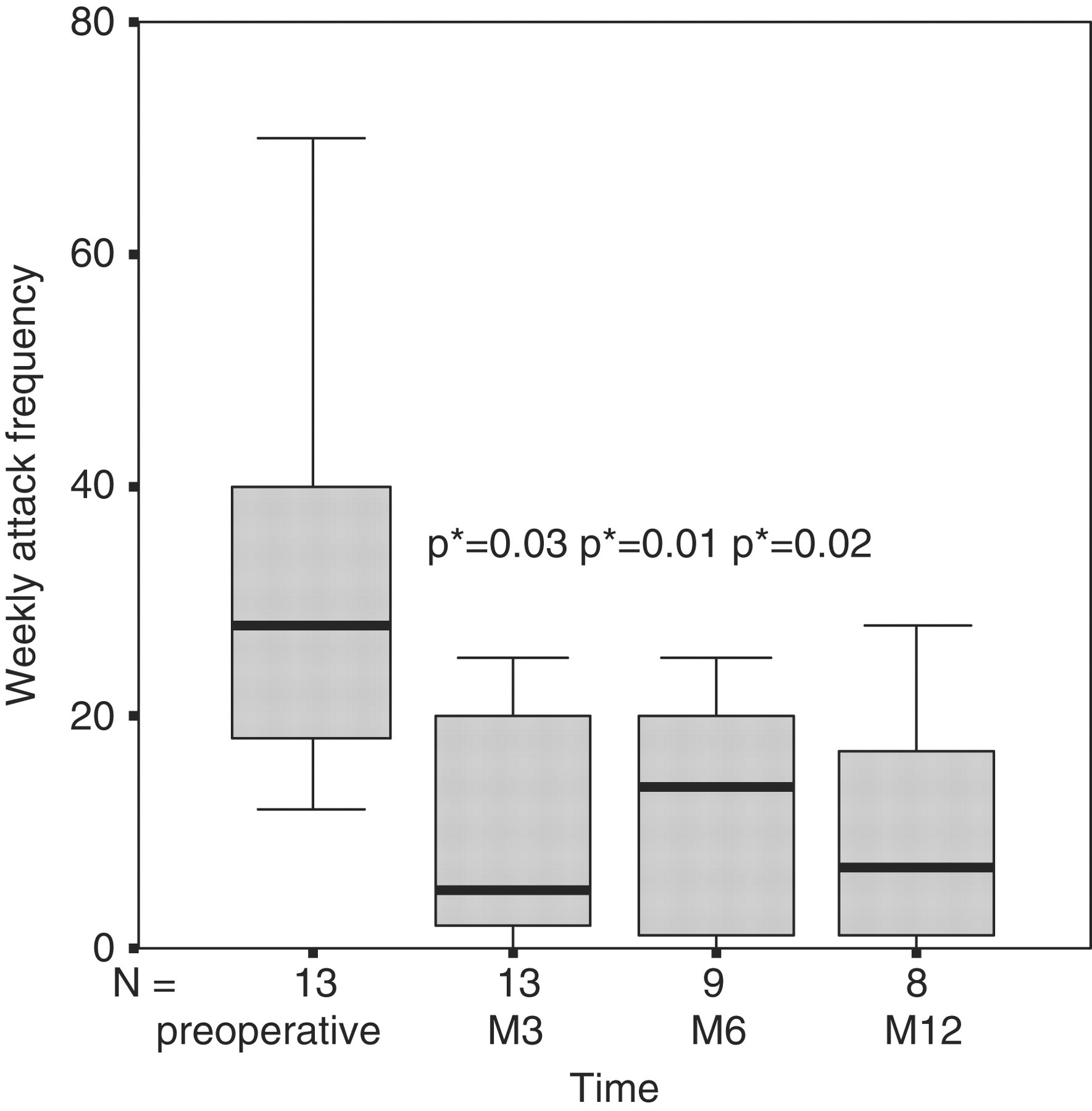

In the eight patients who achieved a 1 year follow-up, the mean attack frequency decreased by 68% after surgery (Table 2 and Figure 1). At last follow-up, the mean attack intensity on the numeric rating scale had decreased by 49% (Table 2 and Figure 2). Seven patients had a follow-up after 1 year and active stimulation. In two of these, we observed the recurrence of seasonal bouts of CH attacks despite the continuation of the stimulation, corresponding to the transformation of a chronic CH to an episodic form of the disease. One patient had a recurrence 16 months after surgery and became completely refractory to ONS. One patient had partial benefit. In three patients with dramatic initial improvement, the effect was maintained over time without any change.
Box-and-whisker plot showing the distribution of pre and post operative mean attack intensities among patients with surviving attacks (n = 12), evaluated on the numeric rating scale. The boxes indicate the inter-quartile range; the whiskers indicate the lowest and the highest datum. *p values for the differences between pre- and postoperative intensities using the Wilcoxon test for paired data. Clinical outcome in 13 chronic refractory cluster headache patients treated by occipital nerve stimulation The patient C3/P3 had no benefit from the ONS and the hardware was removed 6 months after surgery. However, this patient continued to be followed regularly and has been considered in results in ‘intention to treat’ analysis. †This patient initially improved and would recommend the operation to a fellow CH patient at M12, but the therapeutic effect disappeared 16 months after surgery. Consequently, her opinion changed at that time.

At last follow-up (Table 2), patient self-evaluation showed that the majority considered their outcome as excellent or good. Three patients were considered as non-responders (improvement 0–49%), four patients as responders (improvement 50–89%) and six as excellent responders (improvement 90–100%). One year after surgery, all the patients but one would recommend the operation to a fellow CH patient (Table 2). The prophylactic treatment could be stopped or reduced in 8/13 cases. Three patients with initial and long-lasting improvement reported that they did not need to perceive the stimulation-induced occipital paraesthesias to obtain the therapeutic effect.
Hardware infection occurred 6 months after surgery in one patient who had experienced no initial benefit from the procedure. The hardware were removed and not replaced. One patient had a wound issue without infection needing re-operation. One patient perceived the stimulation-induced paraesthesias as unpleasant.
Discussion
Global results of occipital nerve stimulation in patients with refractory cluster headache reported in the literature

No range given.
ONS carries a low risk of minor surgical complications. Early studies reported a high rate of electrode migration due to neck movements. To reduce this risk, we have improved the surgical sub-cutaneous anchoring of the lead and none of our patients experienced electrode migration. ONS seems to be efficient in case series of refractory CCH patients. However, it will be difficult to show its efficacy in controlled and blinded conditions, because the patients perceive ONS-induced paraesthesias. Moreover, most of the published studies have a short follow-up (from 6 to 17.5 months), and details of the long-term outcome are available for only very few patients. One of our patients, initially dramatically improved, completely lost the therapeutic benefit 16 months after the surgery, despite adjustments of the stimulation parameters. Long-term studies are needed to evaluate the place of ONS in the management of CCH patients. However, considering their respective risks of complications, ONS should be proposed before DBS in refractory CCH patients.
The exact mechanisms of action of ONS in CH are still unknown. Several arguments suggest that ONS could act through modulation of convergent nociceptive inputs in the trigemino-cervical complex, involving a ‘gate control theory-like’ mechanism (13). The rapid improvement in CH attack intensity observed in most of our patients is in accordance with this hypothesis. Up to now, the perception of the ONS induced-paraesthesias was considered as the most crucial variable related to the efficacy of ONS, reinforcing this hypothesis. However, in 3 out of our 13 patients, the perception of the paraesthesias was not necessary to obtain a therapeutic effect, suggesting a more complex mechanism. Moreover, the transformation of a chronic CH to an episodic form of the disease, observed in two patients, suggests that ONS could also modulate a central CH generator. However, a recent functional imaging study performed in ONS responders has shown the persistence of an ipsilateral hypothalamic activation, suggesting that ONS does not act on the CH hypothalamic generator (12).