
Abstract
Introduction: Infiltration of the greater occipital nerve (GON) with local anaesthetics and corticosteroids is a treatment option for cluster headache.
Methods: We retrospectively analysed the efficacy and safety of 121 GON injections in 60 patients with episodic or chronic cluster headache over a period of 4 years.
Results: Almost 80% of the infiltrations were at least partially effective (reduction of attack frequency, duration or severity) and 45% resulted in a complete response (no further attacks). The effect was maintained for 3.5 weeks on average in chronic cluster headache. In episodic cluster headache, the effect lasted for most of the bout. In 18 infiltrations, transient side effects were reported, such as local pain, steroid effects (facial oedema, sleeping disorders, acne), bradycardia or syncope.
Conclusion: Our data show that GON infiltration is a valuable and safe option in the clinical setting to treat patients suffering from cluster headache, especially for the episodic form of the disorder.
Keywords
Introduction
Cluster headache (CH) is a primary headache disorder with very severe unilateral head or facial pain, typically in the periorbital region, and is associated with ipsilateral trigeminal autonomic symptoms. The revised International Classification of Headache Disorders, 2nd edition (ICHD-II) of the International Headache Society (1) distinguishes an episodic (ECH) form, usually occurring in bouts lasting 6–12 weeks, and a chronic (CCH) form (regular attacks > 1 year, remissions < 1 month). There are several options for acute (e.g. oxygen, triptans) and prophylactic treatment (e.g. calcium antagonists, antiepileptics). Several studies (2–4) have demonstrated the efficacy of infiltration of the greater occipital nerve (GON).
In all studies no serious adverse events have been reported, but side effects such as transient local pain, syncopal events, transient dizziness, local alopecia or cutaneous atrophy (5–7) have been described.
In this retrospective, open-label study we describe the efficacy and safety outcomes of GON injections in the daily clinical setting.
Methods
We searched all clinical electronic records from the 1 January 2006 to the 31 December 2009 for patients who had received at least one GON infiltration. The following data was collected:
diagnosis according to the ICHD-II (1); demographics and headache characteristics; basic treatment; response to the injection (no response or partial response: reduction of attack frequency, duration or severity of attack > 25%; complete response: no further attacks within 24 h); duration of response; adverse events.
The infiltrations were applied uni- or bilaterally, according to in-house practice, where bilateral infiltration is usually used as an escalation. The injection was performed by three of the authors (AG, FR, PS), according to the description by Ambrosini (2), 1–2 cm beneath the midpoint between the mastoid process and the occipital protuberance. All patients were injected with 3 ml of betamethasone (21 mg betamethasone; a mixture of 6 mg short-acting sodium phosphate and 15 mg long-acting dipropionate) and 2 ml of lignocaine 2%.
The collected data were transcribed into a chart-processing program (Microsoft Excel, version 2003; Microsoft Corporation, Redmond, Washington, USA) and statistical calculations were made using IBM SPSS Statistics, version 19 (IBM, New York, USA). To calculate efficacy, we analysed the first GON injection of all patients with sufficient data from the long-term follow-up visits (range: > 1 month to > 1 year), and all injections together. The value representing the duration of the effect was taken into analysis, when there was a reoccurrence of attacks described at one of the next follow-up visits. To calculate safety, we took all the injections (with short-term follow-up) into account. The Chi-square test was used to compare the categorical variables and the Student’s t-test was used for comparing the means. Figure 1 shows the number of patients and infiltrations (total and per patient group). The study was approved by the local ethics committee.
Flow chart showing the number of patients and infiltrations (total and per patient group). CH: cluster headache; GON: greater occipital nerve; ECH: episodic cluster headache; CCH: chronic cluster headache.
Results
Demographics
A total of 60 cluster headache patients received 127 GON infiltrations, of which 121 had sufficient long-term follow-up data (ECH: 31 patient, 57 infiltrations, 54 with data; CCH: 29 patients, 70 infiltrations, 67 with data). Fifty-two (86.7%) patients were male, eight (12.6%) were female. The mean age was 41.8 years (ECH 41.6 ± 12.1 years, CCH 42.0 ± 11.9 years). For the ECH patients the bout started on average 34.2 ± 44.1 days (median = 14, n = 38) before the injection. The mean attack frequency was 2.9 ± 1.8 per day (median = 2/d, n = 43). For the CCH patients, the baseline frequency was 3.2 ± 2.8 per day (median = 2/d, n = 29).
Efficacy
Response rates of all first injections (A) and the total of all injections (B). Twenty-four patients had two or more GON injections. Panel (C) shows the response rate of the second injection depending on the outcome of the first

GON: great occipital nerve; ECH: episodic cluster headache; CCH: chronic cluster headache.
Of all the infiltrations (n = 121), 54 (44.6%) produced a complete response, 42 (34.7%) a partial response and 25 (20.7%) did not benefit the patients at all. In the ECH group, of all the infiltrations (n = 54), 47 (87.0%) showed a response, 34 (63.0%) a complete response and 13 (24.1%) a partial response; in the CCH group, of all the infiltrations (n = 67) 49 (73.1%) showed a response, 20 (29.9%) a complete response and 29 (43.2%) a partial response.
Duration
In the ECH group (n = 54) the effect lasted on average for 101.9 ± 152.6 days (median = 25 days), 129.5 ± 166.6 days for a complete response (median = 60 days) and 16.5 ± 12.2 days for a partial response (median = 14 days). The mean duration of pain relief in CCH (n = 67) was 24.6 ± 27.8 days (median = 14 days), 17.2 ± 20.7 days for a complete response (median 10 days) and 31.6 ± 32.2 days for partial relief (median = 17.5 days).
Injection site
Overall, there was a complete response in 57.1% patients when infiltrations were made bilaterally compared to only 38.0% patients with unilateral infiltration. Partial response was found in 26.2% of all bilateral infiltrations and in 39.2% of all unilateral infiltrations (Table 1).
Analysis of all GON injections did not show any significant difference between bilateral and unilateral infiltrations. CCH patients had a tendency to a higher rate of complete response after bilateral infiltrations (p = 0.066; Figure 2).
Bilateral versus unilateral infiltrations (n = 67) in patients with chronic cluster headache, indicating better response rates for bilateral injections. (n = number of patients).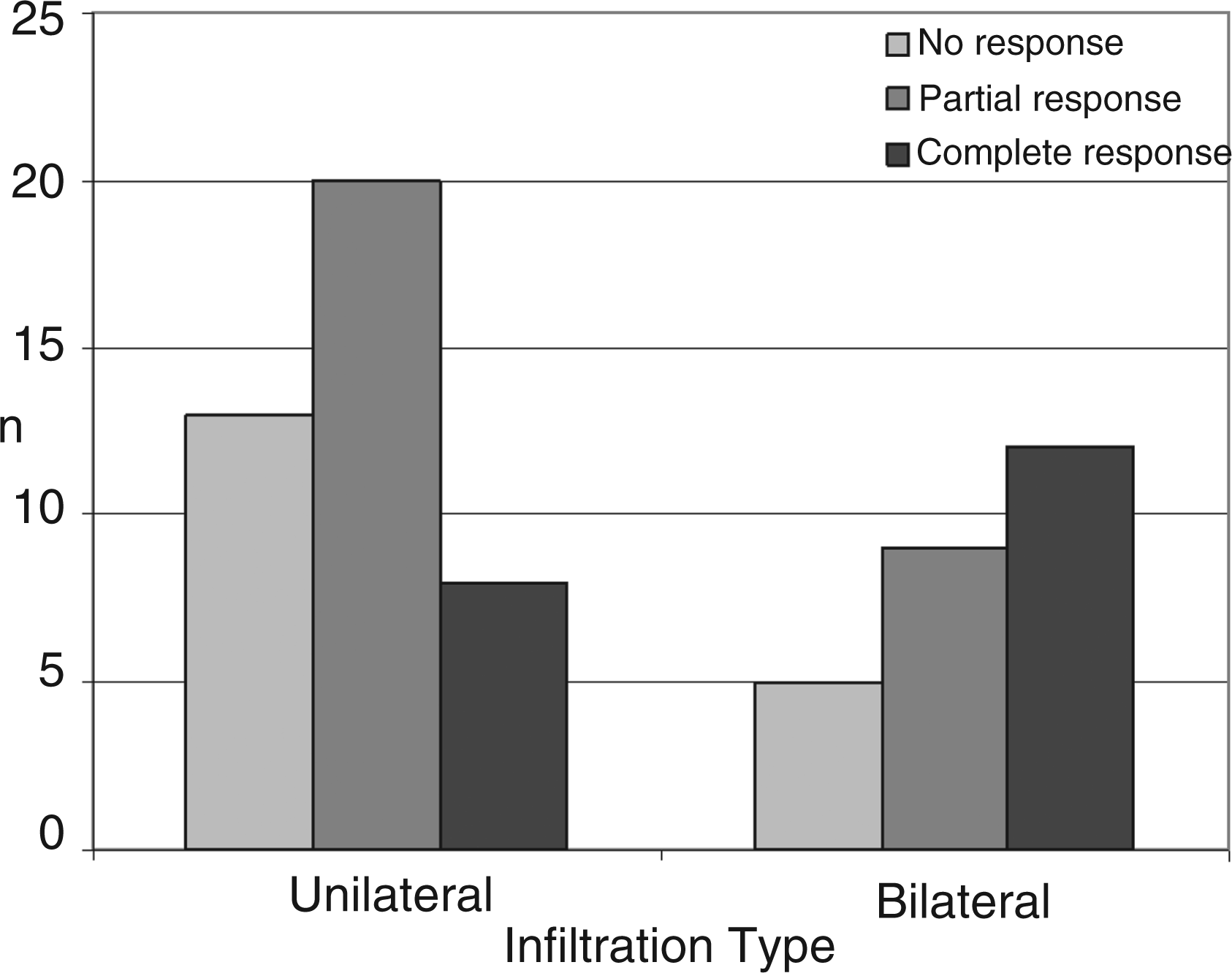
Side effects
Sixteen patients reported side effects for 18 of the 127 injections (14.2%). The following adverse events were reported (more than one adverse event per injection possible):
facial oedema (x 4); sleeping disturbances (x 4); steroid acne (x 3); local/neck pain (x 3); ipsilateral transient eye dysaesthesia (x 1); oral candidiasis (x 2); heartburn (x 2); transient and self-limiting bradycardia (x 1), palpitations (x 1); syncopal attack (x 1).
Nine patients reported side effects after the first injection (15% of total 60).
Baseline treatment
Of the 31 ECH patients (57 injections), 22 were taking additional prophylactic medication (17 verapamil, one methysergide, two carbamazepine, one valproate, one lithium), with some of the medication having been started after the injection. Of the 29 CCH patients (70 injections) 19 were on additional prophylactic treatment (12 verapamil, four topiramate, five valproate, four methysergide, two lithium and two lamotrigine), with all 19 having been on the medication before the GON injection.
Discussion
Our results confirm the good efficacy of GON infiltration in ECH and CCH. Nearly 80% of all infiltrations showed a complete or partial response. These findings are in accordance with previous studies (2,5,8).
Ambrosini et al. (2) studied single injections in a double-blind design with a cohort of 23 patients, 16 ECH and seven CCH (verum: 2.5 ml betamethasone; placebo: saline; both with 0.5 ml of the local anaesthetic xylocaine 2%). The steroids suppressed the pain in more than 80% of patients, whereas there was no benefit in the placebo group. Peres et al. (3) treated 14 CH patients with occipital nerve block, injecting a mixture of lignocaine 1% and triamcinolone 40 mg, and found a good to moderate response in 64% of the patients, with no significant difference in efficacy between ECH and CCH. Afridi et al. (5) showed in a retrospective analysis the best efficacy for CCH patients of GON injections in trigemino-autonomic and other headaches. Tobin and Flitman (9) recently compared several studies of GON infiltrations and found the intervention to be most effective in cervicogenic headache, CH and occipital neuralgia. In a controlled trial, Leroux at al. (4) found a response in 20/21 patients treated with repetitive suboccipital injections of cortivazol, while only 12/22 responded in the placebo group.
Treatment response was good for both ECH and CCH, but the outcome was significantly better for ECH (p = 0.004). Treatment response and effect duration in ECH may well have been overestimated by the fact that some of the infiltrations could have been administered near the end of the bout; therefore, according to our definition for effect duration, the time until the occurrence of the next bout would bias the results for complete responses. If the patient only partially responded, then we would know that they are still in the same bout, and the duration of the effect of the intervention may be evaluated more accurately. However, in all of the effective cases the response was within 24 h, which would support the efficacy of GON infiltration rather than an effect of the natural course. The same is true for the patients who were taking baseline treatment at the time of the infiltration. Even if other prophylactic treatments were started shortly after the consultation, it is highly unlikely that they would be immediately effective.
Limitations of this retrospective analysis include the fact that the records were not strictly standardised and that patients were followed up at different intervals (from > 1 month to > 1 year), and, occasionally, not by the authors. However, as described in the ‘Methods’ section of this paper, effect duration was calculated only when clear description was available from the files. In view of the general advice given to each patient to return if something bad happened or if the headache had come back, the findings may even be underestimated.
In CCH we found a trend for better response with bilateral infiltrations. Whether this is a dose effect or due to bilateral application is open to speculation. In our institution, the dosage of both steroid and local anaesthetic is doubled.
Side effects were noted after 18 injections. Some of the side effects can be clearly attributed to the steroid, while others may be due to the procedure itself or may be interpreted as vasovagal effects. However, this is clearly less than in the study where repetitive injections were used (4), where 74% (18/21 patients and 14/22 controls) had mild transient side effects.
Conclusion
Infiltration of the GON with steroids and lignocaine seems to be an effective method to alleviate the pain of CH patients, and especially ECH patients. Nearly 80% of all infiltrations resulted in an at least a partial effect and 43.7% in the complete relief of pain. The effect lasted on average 3.5 weeks. Our data suggest that CCH patients may benefit more from bilateral infiltration, whereas ECH patients may also benefit from ipsilateral infiltration. Although local infiltration of steroids seems to be a much safer option compared to oral administration, systemic side effects still have to be considered. Only a few, transient and mild side effects were observed in our patient group.
Our retrospective, uncontrolled, open-label study is fighting with the typical weaknesses of this type of study. However, the analysis of a high number of consecutive GON injections is a clear strength and demonstrates the value and safety of the technique in the daily clinical setting.
Footnotes
*
These authors contributed equally to this article
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.