
Abstract
Objectives:
The main objective of this study was to compare the effectiveness of aerobic exercise with physiotherapy. A second objective was to evaluate whether patients with pain referred to the head during manual palpation will benefit more from physiotherapy than patients with local or no pain.
Methods:
A total of 103 patients with migraine received physiotherapy (n = 79) or supervised aerobic exercise (n = 24) according to their preference as an add-on treatment. Both groups had the same contact time with a specialized physiotherapist. The primary outcome measure was headache frequency during the 4 weeks after the intervention. Eighty-seven patients were analyzed at the primary end point (n = 69 in the physiotherapy group; n = 18 in the aerobic exercise group). A follow-up assessment was conducted 3 months after the final intervention.
Results:
During the initial assessment of the upper cervical spine, 17 patients reported no pain, 45 local pain, and 25 referred pain to the head. Patients in the physiotherapy group had a mean reduction of 1.8 days (standard deviation (SD) 6.07), while patients in the aerobic exercise group had a mean reduction of 1.2 days (SD 4.27) at the primary end point. This difference was not statistically significant (p = 0.8). The largest improvement was noted in the group that showed referred pain to the head and received physiotherapy (2.13 days (SD 7.82)). Only patients in the physiotherapy group reported a subjectively perceived general improvement.
Conclusions:
Patients had a strong preference for physiotherapy. Both groups showed small reductions in headache frequency. Effects were superior after physiotherapy but not statistically significant. Patients with pain referred to the head responded best to a physiotherapy intervention.
Introduction
The Global Burden of Disease Study reported migraine worldwide as the sixth most prevalent out of 328 diseases and ranked migraine as the second cause of years lived with disability after low back pain. 1 Up to 4% of episodic migraine sufferers experience a transition to chronic migraine. 2,3 Migraine compromises the quality of life, 3,4 reduces the functional capacity in work and leisure, and results in high socioeconomic costs, mainly due to absence from work on migraine days. 5,6
According to international guidelines, the treatment for migraine is primarily pharmacological. 7 –10 However, acute as well as preventive medication is associated with side effects, for example, weight gain and adverse events such as cardiovascular disease. 11 Patients therefore wish to reduce their medication intake by using non-pharmacological interventions such as physiotherapy. 12 The only non-pharmacological interventions recommended in national and international guidelines are relaxation, behavioral therapy, and aerobic exercise. The guideline published by the British Association for the Study of Headaches 13 adds that manual therapy may be tried in patients with a cervical musculoskeletal dysfunction. Recent work by our group showed that more than 90% of migraine patients have such cervical dysfunctions. 14 It is therefore surprising that there is hardly any evidence for physiotherapy including manual therapy and exercises for patients with migraine. A systematic review from 2016 investigating the effectiveness of non-pharmacological interventions for different headache types indicated that trials on migraine employed either aerobic exercise or a multidisciplinary intervention. 15 No studies were identified evaluating the effect of physiotherapy including mobilization and/or specific exercises. Studies published after the cutoff date of the systematic review have shown that physiotherapy interventions such as myofascial treatments 16,17 or a combination of manual therapy and exercises 18 also seem to be effective for migraine. Aerobic endurance training has also been reinvestigated in recent trials 19,20 reporting an effectiveness for migraine frequency reduction. However, contradictory evidence also exists for both types of intervention. 21,22
In the absence of controlled trials confirming the effectiveness of physiotherapy for the reduction of headache frequency, physiotherapy should not be recommended as an evidence-based intervention for migraine. Nevertheless, 30% of primary care physicians refer migraine patients to physiotherapy 23 and patients report that manual therapy is the most common non-pharmaceutical strategy used to treat pain relief in recurrent headaches. 24 This corresponds with publications that report a high prevalence of neck pain premonitory or during migraine attacks. 25 –29 One could therefore reason that improving musculoskeletal dysfunctions in the neck using physiotherapy techniques such as mobilization and specific exercise might reduce the number of migraine attacks and prevent its chronification.
A general problem in randomized controlled trials on non-pharmacological interventions, where patient blinding is not feasible, is the bias introduced by patient preference. If patients are randomized to the non-desired intervention they might not perform as well as they would in their preferred treatment group. This is a frequent threat for the validity of a trial. A meta-analysis on 11 randomized trials indicated that patients who received their preferred intervention had greater effect sizes than patients who were indifferent or received the undesired treatment. 30
The aim of this study was therefore to investigate the effectiveness of physiotherapy for the reduction of headache frequency in comparison to guideline-based aerobic exercise in patients with chronic and frequent episodic migraine in a modern and pragmatic study design allowing patients to choose their preferred intervention. A second objective was to evaluate whether patients with referred pain during manual palpation of the upper cervical spine respond more to either of the interventions.
Methods
All procedures including informed consent as well as data protection and handling followed international guidelines on good scientific practice (Declaration of Helsinki, ICH-GCP E6(R1)). Ethical approval was obtained from the local ethics committee (Ärztekammer Hamburg PV5011). The study was registered a priori at the German Clinical Trials Register (DRKS00009618).
Patients were recruited at a university outpatient clinic specialized in the diagnosis and management of headaches. Inclusion criteria were a diagnosis of chronic or frequent episodic migraine (IHS classification version III, 31 age ≥18 years, duration of the disease for a minimum of 2 years, minimum average frequency of 6 headache days in 4 weeks confirmed by a headache diary, and written informed consent. A headache diary had to be kept for a minimum of 4 weeks prior to the first day of the intervention.
Exclusion criteria were diagnosed cervical pathology (e.g. disc disease), cervical trauma within the past 2 years (e.g. whiplash-associated disorder), rheumatoid disease, craniomandibular dysfunction (self-report), diagnosed neurological or psychiatric disease, >10 days of analgesic medication per month (to exclude medication overuse headache), currently receiving physiotherapy or a comparable treatment for the reduction of migraine or currently exercising more than once a week for more than 30 min at an aerobic level.
The interventions were offered as an add-on to the usual outpatient headache clinic care including acute and preventive medication. However, to disentangle the effect of medication and the additional intervention, medication had to be unchanged in the past 3 months and had to be maintained stable over the entire study period. This pragmatic approach was chosen to reflect clinical practice and also for ethical reasons preventing that patients had to withdraw drugs prior to inclusion.
Interventions
Physiotherapy was scheduled as 10 sessions of a 30-min duration, each provided by a physiotherapist with additional manual therapy training and >10 years of clinical experience over a period of 5 weeks. This mode and duration reflects current prescription standards. To allow a generalizability of the results to clinical practice and to reflect the clinical reasoning described by the World Organization of Physical Therapy, 32 participating physiotherapists based their treatment approach on the findings from a physical examination on the first day following an international consensus on physical examination tests recently published by our work group. 33 These included head posture, cervical range of motion, combined cervical movements, screening of the thoracic spine, shoulder girdle muscle testing, manual testing of the upper cervical spine, reproduction and resolution of headaches during sustained palpation, trigger point palpation of the neck and face muscles, passive physiological cervical movements, flexion–rotation test, and craniocervical flexion test. Details about the tests are available in the literature. 14,33,34 For the transferability of the results, only standard physiotherapy approaches were used, and all applied techniques were documented after each treatment session.
Aerobic exercise was chosen as an active control intervention, because this is the only non-pharmacological, active intervention recommended in headache guidelines. 2,35,36 Following the treatment protocol of a recently published aerobic exercise program, each exercise session included 5–10 min warm-up, 30 min aerobic training, and 5–10 cooldown, preceded by a cardiovascular test. 37 One session each week was supervised by a physiotherapist with equal qualifications to the physiotherapist treating the physiotherapy group to ensure the same amount and quality of contact time with a health professional in both groups. A second unsupervised session was compulsory and had to be documented by the patient. To ensure that patients exercised within the aerobic range, the Borg Scale was used to measure an exertion value of 11–13 for untrained participants and 13–15 for trained participants. 38,39
To eliminate the bias introduced by randomization to a preferred versus unpreferred treatment group, patients were informed that aerobic exercise is a guideline-based treatment, while physiotherapy is not and that they are free to choose their preferred intervention.
Outcome parameters
The primary outcome measure following the recommendation of the International Headache Association 40 and a recently conducted Delphi survey was headache frequency (measured using a headache diary over a period of 4 weeks). To record headache frequency prior to the intervention, a 4-week run-in period was required. The primary end point was the 4-week period following the final day of the intervention. Secondary outcome measures were the Migraine Disability Assessment Scale (MIDAS), 41 global rating of self-perceived improvement (scale from −7 to +7), 42 the Neck Disability Index (NDI), 43 and the Personal Health Questionnaire (PHQ). 44
Based on an international consensus study 33 and a stratification according to the symptom response to upper cervical manual palpation, 14 all patients were assessed by an experienced physiotherapist, not involved in the treatment and blinded toward the group allocation prior to the first and immediately after the final intervention.
Analyses
In the absence of trials comparing physiotherapy with exercise and without recommendations for preference-based trials, the sample size calculation was based on a medium effect size, 80% power, and an α value of 0.05, resulting in a total sample size of 102 patients. The Statistical Package for Social Sciences (SPSS, version 24) was used for all statistical analyses. For parametric data, the Kolmogorov–Smirnov test was used to confirm normal distribution. Unless otherwise described, the data are presented as mean values with standard deviations (SDs). Baseline characteristics across intervention groups were compared with independent t-tests (Table 1). The difference between the two intervention groups for the primary outcome measure (headache frequency) at the primary end point (4 weeks after the final day of the intervention) was calculated using repeated-measures analysis of variance (ANOVA) with the factors Time and Group. Secondary analyses to evaluate whether patients benefited more when they showed cervical musculoskeletal dysfunction at baseline were analyzed using a multivariate ANOVA based on the difference in headache days before and after the intervention and the groups “no pain on palpation,” “local pain,” and “referred pain” as well as treatment group as factors. Post hoc analyses were performed with Bonferroni correction if ANOVA results showed statistical significance. Global perceived change rating is a categorical measure and was therefore analyzed with nonparametric tests (Mann–Whitney U). The value of p < 0.05 was assumed to be statistically significant.
Baseline characteristics across intervention groups.
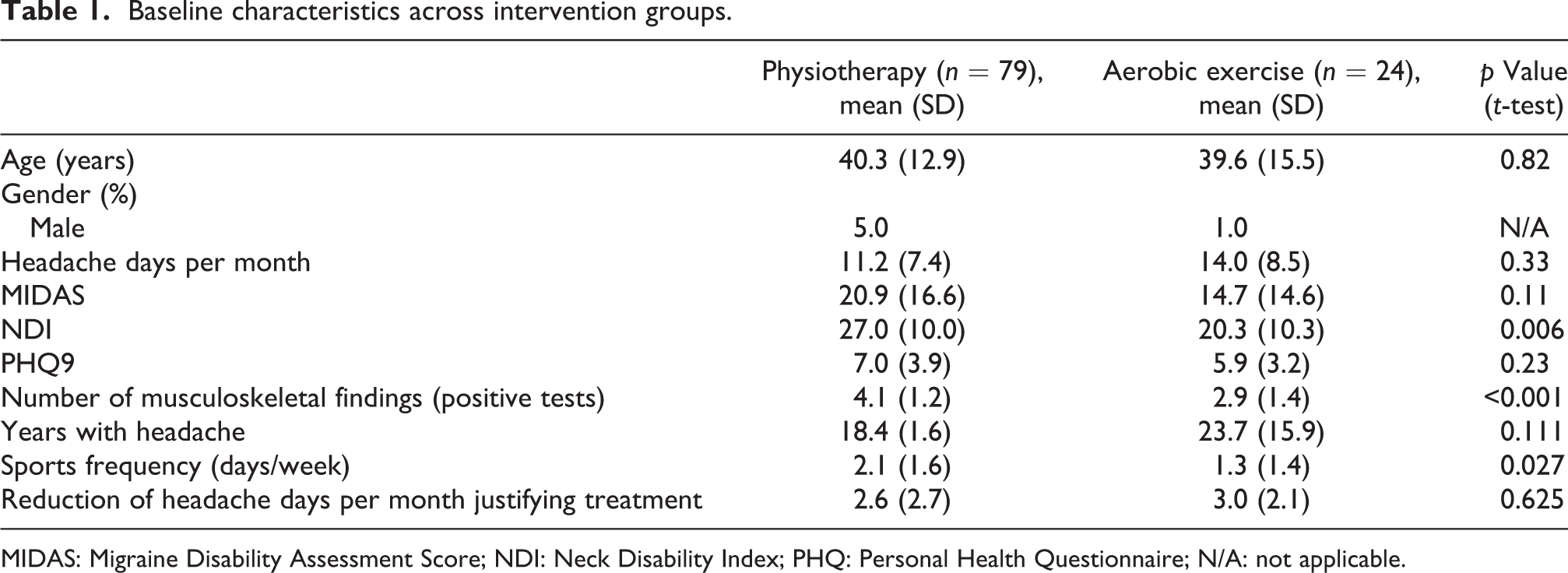
MIDAS: Migraine Disability Assessment Score; NDI: Neck Disability Index; PHQ: Personal Health Questionnaire; N/A: not applicable.
Results
This study included 103 patients with migraine. Of these, 79 chose physiotherapy and 24 chose aerobic exercise. There was no statistically significant difference between the two groups regarding age and gender as well as all other measured parameters, except for NDI, number of positive musculoskeletal examination tests and sport frequency, which were higher in the physiotherapy group. Baseline data for both groups are presented in Table 1. Six participants (7.6%) discontinued the physiotherapy intervention, and four patients discontinued (16.7%) the aerobic exercise. Reasons given were time and distance to treatment location and in two cases an increase in headache intensity in the aerobic exercise group. Eighty-seven patients completed the assessment at the primary end point 4 weeks after the final intervention (Figure 1).

Flow-diagram of patient inclusion.
The percentage of time used within one physiotherapy treatment session was on average 56% manual therapy mobilization, 21% myofascial treatment and 19% exercises, as well as 4% education. During the supervised aerobic training, patients could choose as well as switch between cycling ergometer, treadmill, and cross-trainer. Various endurance training methods were chosen for the second compulsory home-based training session. These included nordic walking or slow running (chosen by 44% of the participants), outdoor cycling (38%), swimming (31%), cycling ergometer training (19%), or other activities (25%).
The primary outcome measure “reduction in headache days in the past 4 weeks” was not significantly different between the intervention groups at the primary end point (4 weeks following the last day of treatment): Patients in the physiotherapy group had a mean reduction of 1.8 days (SD 6.07), while patients in the aerobic exercise group had a mean reduction of 1.2 days (SD 4.27). The repeated-measures ANOVA showed no significant interaction of the factors group and time (F = 0.257; p = 0.8). Including the parameters which were significantly different between groups at baseline (NDI, number of positive tests, sports frequency) into an analysis of covariance model, this effect remained stable with F = 0.404; p = 0.7.
At the primary end point (4 weeks following the final day of the intervention), the secondary outcome measures MIDAS (p = 0.198; 95% confidence interval (CI) −10.7008 to 2.2481) and PHQ (p = 0.70; 95% CI −2.553 to 1.727) were not statistically significant, and patients in the physiotherapy group still had more disability due to neck pain measured by the NDI (p = 0.045; 95% CI 0.135 to 11.796) (Figure 2, Table 2). The global rating of change score was significantly higher in the physiotherapy group compared to the aerobic exercise group at 4 weeks posttreatment (p = 0.002; Mann–Whitney U test) and at 3 months post intervention (p = 0.024). The grouped median for global rating of change was 3 points on a scale ranging from −7 (extremely worse) to +7 (extremely better) in the physiotherapy group and 1 point in the aerobic exercise group at both time points.
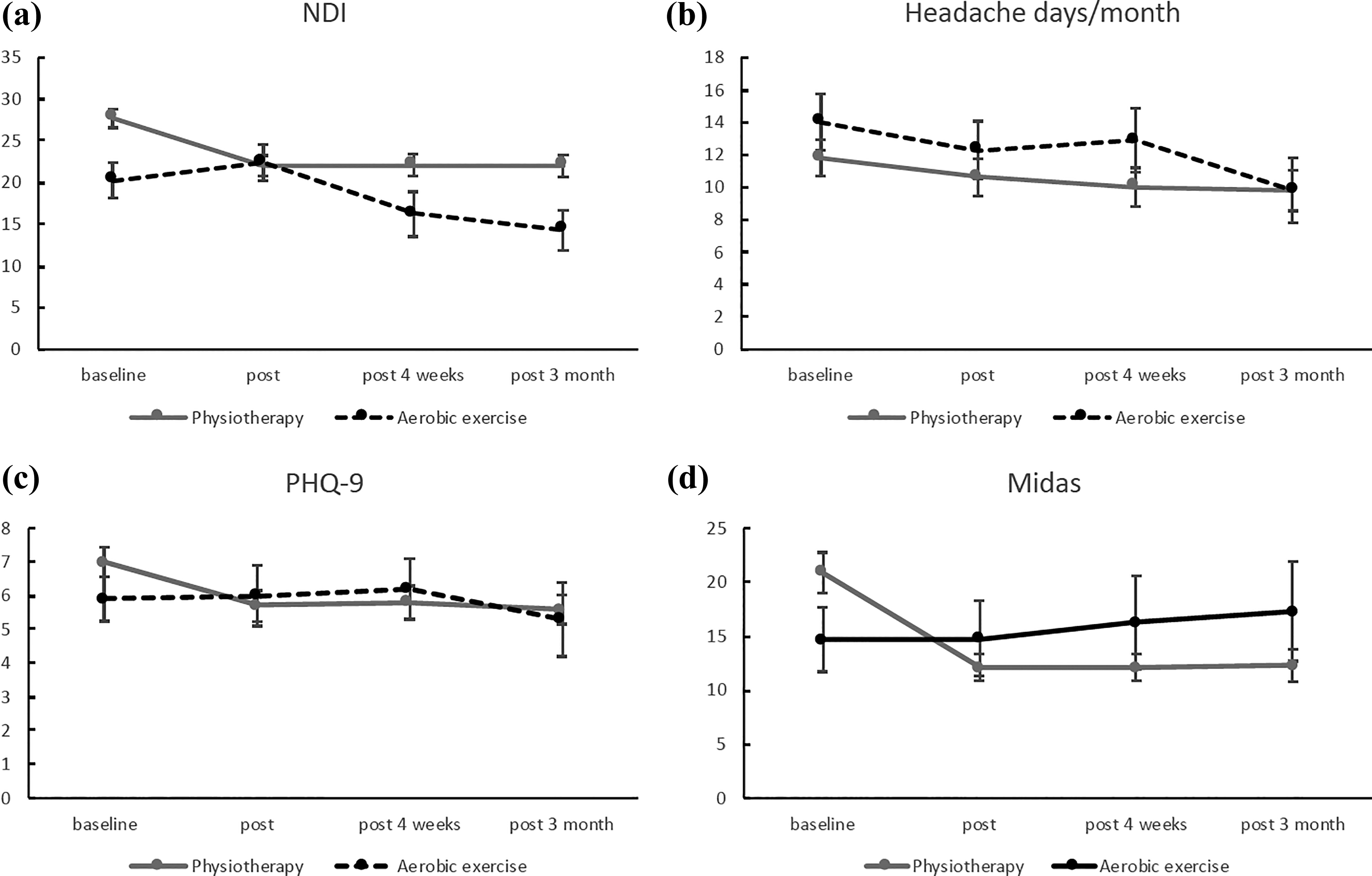
Primary and secondary outcomes for all time points: (a) NDI, (b) headaches days/month, (c) PHQ-9, and (d) MIDAS. Figures display means (SEM). NDI: Neck Disability Index; PHQ: Personal Health Questionnaire; MIDAS: Migraine Disability Assessment Score.
Primary and secondary outcomes for all time points.

MIDAS: Migraine Disability Assessment Score; NDI: Neck Disability Index; PHQ: Personal Health Questionnaire; GROC: Global Rating of Change; SD: standard deviation; IQR: interquartile range.
The secondary analysis showed that patients with referred pain during baseline evaluation of the upper cervical spine had the largest reduction in headache days (1.91 days (SD 6.64)) with more reduction in the physiotherapy group (2.13 days (SD 7.82)) than in the aerobic exercise group (1.91 days (SD 6.64)) (Figure 3). This was also not significant.
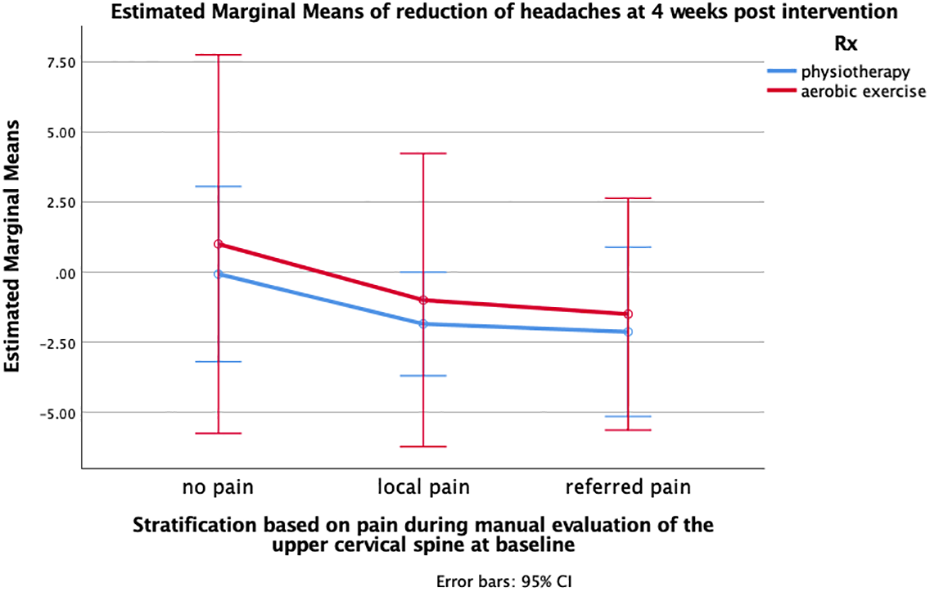
Reduction in headache days according to stratification based on palpation of the upper cervical spine at baseline.
Discussion
Both interventions showed a slight improvement in headache frequency as an add-on intervention to specialized neurological headache clinic care. This ranged from 1.2 days in the aerobic exercise group to 1.8 days in the physiotherapy group and more than 2 days in the group that showed referred pain to the head during baseline assessment and received physiotherapy as an intervention. The reduction in headache days was still reported 3 months after the intervention and continued to decrease in the aerobic exercise group, pointing toward a better effect if patients continue to exercise.
The secondary outcome measure “self-rated perceived change” was significantly different between intervention groups at all post intervention time points and ranged around 3 points on a −7 to +7 scale in the physiotherapy group, indicating perceived clinically relevant improvement, 42 which was not reported by the aerobic exercise group although both interventions involved equal hours of contact time with a specialized physiotherapist. This was also reflected by the MIDAS with significant reductions in the physiotherapy group, but, in contrast to the headache days, increased with time rather than decreased in the aerobic exercise group. MIDAS measures the number of days, when activities were reduced or impossible due to migraine and is therefore more subjective than the headache diary. Increased values at 3 months might be carefully interpreted as either frustration that despite the exercise, migraine still reduces the activity levels on some days or that vice versa in the physiotherapy group more time was spent on education, reducing the threat value of symptoms and possibly encouraging patients to normal activity levels on days with mild symptoms.
An interesting aspect of this study was the clear patient preference for physiotherapy when given the choice. This might partially be due to the study sample of patients who attended a specialized headache clinic. Most of them were aware of guideline recommendations and may have tried aerobic exercise (as well as relaxation exercises in previous treatment attempts). Verbal communication during the recruitment period provided additional insight into patient choice: some patients stated that they were afraid of aerobic exercise, since they had previously experienced an exacerbation of headaches during physical activity or were even convinced that aerobic exercise would trigger their migraine attacks. An additional explanation was that patients, although not exceeding the eligibility criterion of a maximum of 30 min of aerobic exercise per week, already perceived themselves as physically active. The two groups would certainly have shown more drop outs if patients were randomized into treatment groups.
Another explanation was the reported high level of neck pain that migraine patients experienced before during or after their attacks, which is in line with the literature. 25 –27 In the current data, neck pain was reflected by the high levels of neck disability and neck dysfunctions during the physical examination tests. The number of detected dysfunctions was similar to the data previously reported on neck dysfunctions in migraine patients. 14,34 Patients who opted for the physiotherapy intervention showed significantly more neck-associated disability and dysfunctions at baseline, thereby explaining why this subgroup expected better results from the physiotherapy treatment.
Musculoskeletal changes were reduced after the physiotherapy intervention and patients reported a significantly better global perception of improvement in the physiotherapy group. However, the primary outcome “reduction of headache days per month” was only slightly higher in the physiotherapy group and most pronounced in the group that showed referred pain during upper cervical spine palpation at baseline.
The small effects measured in both groups indicate that non-pharmacological interventions have little room for additional improvement as an add-on to pharmacological treatment: We note that we did not test these interventions in the absence of medication. It was neither feasible to treat only patients without preventive medication nor ethically possible to remove preventive medication prior to the treatment. One could argue that the presence of preventative medication increased the difficulty to add any improvement on top of the effect of such medication. However, the small effect was in line with a recent systematic review and meta-analysis of aerobic exercise for the reduction of migraine symptoms which reported a combined effect of 0.6 (SD 0.3) migraine days per month. 45 We note that each patient was asked prior to the intervention how many days reduction would be perceived as clinically relevant and the majority of patients answered that each day less would be worth the time and effort spent on the treatment. One day improvement per month is however not clinically relevant when compared to pharmaceutical or electroceutical trials, 46 a definite number of days that can be considered clinically relevant change has never been defined but the 2-day difference as reported by patients in the physiotherapy group who had a detectable cervical dysfunction at baseline was, however, perceived as meaningful by this study’s sample .
A limitation of this study might be the chosen intensity of the aerobic exercise intervention, since a recent study showed that high-intensity aerobic endurance training program was superior to moderate training to reduce migraine days. 19 The current trial used a moderate intensity and possibly a training period which was not long enough to induce change in cardiovascular fitness. However, patients in the aerobic training group continued to exercise after the intervention period and were reevaluated 3 months after the final intervention. If the intervention period had played a role, data at 3-month post intervention would have indicated this effect.
The study approach to include patient preference rather than randomization for treatment group allocation has until now not been used in many previous publications. This is somewhat surprising, since a systematic review and meta-analysis showed that patient preference significantly influences treatment effects in randomized controlled trials of musculoskeletal medicine. 30 This powerful influence could bias results from any RCT and should be considered more in future RCTs. While this is a relatively new approach and not reflecting current methodological recommendations for effectiveness studies, it does reflect clinical daily practice and has started to occur more often in research, recently, possibly indicating the need to revise recommendations for studies where a placebo or sham control is not feasible. 47 –51 Nevertheless, this has led to an unbalanced distribution of patients in both groups. This is a limitation of the study reducing the power of the effect but also a result, because it shows how the patient preference was biased toward the manual therapy intervention. Additionally, it has to be pointed out that the population was almost exclusively female. This distribution is typical for migraine trials and reflects the higher percentage of migraine in women.
Conclusion
Physiotherapy is not significantly more effective than aerobic exercise but preferred by migraine patients, especially by those with a high level of neck associated disability and neck dysfunctions as shown by physical examination. An initial assessment of the upper cervical spine can support the decision toward a physiotherapy intervention since patients with referred pain responded with the largest reduction in headache days after a physiotherapy intervention.
Clinical implications
Migraine patients had a strong preference for manual therapy over aerobic exercise. Both interventions had a comparable reduction in headache days per month. Improvements in headache days per month were not significant or either intervention.
Footnotes
Author contributions
KL planned and designed the trial, analyzed data and provided first draft of manuscript in collaboration with TS; WS, KvK and TS examined and treated patients and contributed to the trial design; TS contributed to the trial design, supported the statistical analysis of the data, and drafted the manuscript; and AM who is the senior author helped in trial design and contributed to final draft of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.