
Abstract
Aim
To evaluate aerobic exercise in migraine and co-existing tension-type headache and neck pain.
Methods
Consecutively recruited persons with migraine and co-existing tension-type headache and neck pain were randomized into an exercise group or control group. Aerobic exercise consisted of bike/cross-trainer/brisk walking for 45 minutes, three times/week. Controls continued usual daily activities. Pain frequency, intensity, and duration; physical fitness, level of physical activity, well-being and ability to engage in daily activities were assessed at baseline, after treatment and at follow-up.
Results
Fifty-two persons completed the study. Significant between-group improvements for the exercise group were found for physical fitness, level of physical activity, migraine burden and the ability to engage in physical activity because of reduced impact of tension-type headache and neck pain. Within the exercise group, significant reduction was found for migraine frequency, pain intensity and duration, neck pain intensity, and burden of migraine; an increase in physical fitness and well-being.
Conclusions
Exercise significantly reduced the burden of migraine and the ability to engage in physical activity because of reduced impact of tension-type headache and neck pain. Exercise also reduced migraine frequency, pain intensity and duration, although this was not significant compared to controls. These results emphasize the importance of regular aerobic exercise for reduction of migraine burden.
Introduction
A clinic-based study has shown that a large proportion (67%) of persons with migraine suffer from co-existing tension-type headache (TTH) and neck pain (NP) (1). This recent study also showed that persons with migraine and co-existing TTH and NP suffered from lower psychological wellbeing and had a much lower level of physical activity compared to healthy controls. Their ability to perform physical activity was also reduced owing both to migraine and TTH, and to a lesser degree, owing to NP (1).
Exercise is a recommended non-pharmacological treatment for persons with migraine (2). There is increasing evidence that physical activity reduces migraine frequency, pain intensity and pain duration (3–10), and also improves quality of life (4,7,11). These clinical findings were supported by population-based studies, which reported that low physical activity was associated with a higher prevalence of migraine (12), and that there was an inverse relationship between migraine and physical fitness (13).
Physical activity has a positive effect on health and wellbeing (14) and is a widely used physiotherapeutic treatment strategy. Migraine especially has a great impact on family life and social activities (15), and co-existing TTH and NP may have a negative influence on their burden of disease as the prognosis of migraine may worsen with co-existing TTH (16), and NP has been found to be a predictor of increased disability in persons with migraine (17).
The effect of aerobic exercise involving cross-training, biking and brisk walking on persons with migraine and co-existing TTH and NP has not yet been studied. The aim of this study was, therefore, to evaluate the effect of a three-month aerobic exercise program for persons suffering from migraine and co-existing TTH and NP in a randomized, controlled, clinical trial.
Methods
Design
The study was a prospective, single-centre, open-label, randomized and controlled clinical trial evaluating three months of aerobic exercise with follow-up six months from baseline (Figure 1).
Study design.
Ethics
All participants signed an informed consent form. Databases generated during the study excluded personal data in accordance with requirements of the Danish Data Protection Agency. The local ethical committee of the Capital Region approved the study (protocol no H-1-2011-090). The study was conducted in accordance with the Declaration of Helsinki. The study is registered in the Protocol Registration and Results System; Register Number: NCT02269501.
Participants
Seventy persons were recruited via public advertisements and referrals from a specialized headache centre in Denmark from January 2013 to July 2015. There were no requirements with regard to their exercise level. The inclusion criteria were a minimum of two attacks of migraine and a minimum of one day with TTH and a minimum of one day with NP per month. The exclusion criteria were whiplash injury, significant neck trauma (caused by trauma to the neck, fracture, distortion, or violent attack that have caused the current NP), nerve root compression of the cervical spine, persistent headache attributed to traumatic injury to the head, medication overuse headache, cluster headache, trigeminal neuralgia, pregnancy, breastfeeding, severe physical and/or mental illness, abuse of alcohol and drugs, and inability to speak and understand Danish.
Randomization
Participants fulfilling the inclusion criteria were asked to complete a four-week diagnostic headache diary (18) supplemented with questions about NP to confirm the requirements for frequency of headache and NP. After completion, the participants were randomized into an exercise group or control group. The block randomization sequence was conducted by an independent medical doctor and based on a computer-generated list with a block size of six. The results of the randomization were sealed in envelopes provided with consecutive numbers by an independent physiotherapist. The enrolling physiotherapist (LSK) was not involved in this procedure.
Procedure
All participants were provided with information about the study and a leaflet about possible migraine triggers. All participants were examined and diagnosed by a neurologist and underwent a physical examination by an experienced physiotherapist (LSK). The four-week diagnostic headache diary served as baseline. The diary was continued during the three-month treatment period, of which the last four weeks were used to measure the status of migraine, TTH and NP. This procedure continued for four weeks prior to follow-up.
Diagnostic headache diary
The diagnostic headache diary was used to gather information on headache characteristics and associated symptoms to support the diagnosis of migraine or TTH. Chronic migraine was subdivided into migraine headache and tension-type-like headache (19). Participants were asked to report frequency, pain intensity and duration of headache and NP; as well as intake of acute medication. Headache forms were classified according to the International Classification of Headache Disorders (ICHD-3 beta) (19). NP was defined as pain located to the anatomic region of the neck with or without radiation to the head, trunk, and upper limbs grade I-II (based on the classification system developed by the Neck Pain Task Force) (20).
Participants completed questionnaires on three occasions during the study period: At baseline, at the end of the treatment period, and at the end of follow-up. These questionnaires were validated for the target population in a previous study (21) and included: (a) International Physical Activity Questionnaire short form (IPAQ) (22), (b) the World Health Organization five-item Well-Being Index (WHO-5) (23) and (c) Impact of Migraine, Tension-Type Headache and Neck Pain (Impact M-TTH-NP) (21).
IPAQ
The level of physical activity was measured using the IPAQ short form (22). The total weekly exercise time in minutes (walking, moderate and vigorous physical activity) was multiplied by the metabolic equivalent task (MET) for each category. One MET equals the energy expenditure while resting. Total physical activity MET-minutes/week was computed to show the sum of walking, moderate, and vigorous MET-minutes/week scores.
WHO-5
Psychological well-being was measured by WHO-5 based on a 2-week recall period (23). Responses were rated on six-point Likert categories with the end-points 0 (at no time) and 5 (all of the time). The scores were summed (maximum score 25) then multiplied by 4 (range 0–100, with lower scores indicating lower wellbeing).
Impact M-TTH-NP
The Impact M-TTH-NP consists of 79 items covering pain, headache triggers; psychosocial, socioeconomic and work related factors during a four-week recall period (21). In the present study, perceived ability to perform daily activities was used and assessed by 15 items: “In the past four weeks, when you had migraine/TTH/NP, to what extent did you experience a decrease in your ability to perform the following activities?”
Responses were rated on an 11-point numeric rating scale (NRS-11) with the end points 0 = no decrease and 10 = decreased to the greatest possible extent. The daily activities included were ability to perform household chores, perform paid work/study tasks, participate in social activities not including family activities, participate in family activities, and engage in physical activity such as aerobic exercise or strength training.
Physical fitness
The participants performed a test of their degree of physical fitness, which was based on an estimation of the maximum oxygen uptake (VO2max) using Åstrand’s submaximal bicycle test (24). The test was performed on an ergometer bicycle (Monark Ergomedic 939E PC, Monark Exercise AB, Stockholm, Sweden) and conducted by a physiotherapist (LSK) and an assisting technician (HA) who were not blinded to the participants’ grouping. The test was applied at baseline, at the end of the treatment period, and at the end of follow-up.
During the study period, all participants continued with prescribed preventive and acute medication (adjusted regularly as needed). Those who were already engaged in some form of exercise activity were not asked to stop.
The participants were not allowed to seek other nonpharmacological treatment (such as acupuncture or psychological therapy) for their headache and NP during the study period.
Exercise group
The exercise group trained three times a week for three months. Once a week, they trained with a physiotherapist (LSK) and twice a week at home or at a gym. They were instructed to exercise at minimum once a week on a bike (indoor or outdoor) and at minimum once a week on a cross-trainer or brisk walking. Those who were comfortable with running could choose to do that as an alternative to cross-training or brisk walking. Each training session lasted for 45 minutes and exercise intensity was monitored by the individual’s perceived breathing rate corresponding to the exercise intensity based on a modified Borg’s scale of Rated Perceived Exertion (RPE scale) (25). The exercise period was divided into ten minutes warm-up (slightly out of breath but conversation is possible; corresponding to 11–13 RPE), 30 minutes endurance training (out of breath; conversation in short sentences; corresponding to 14–16 RPE) and five minutes cool-down (slightly out of breath but conversation is possible; corresponding to 11–13 RPE). During exercise lessons (with LSK), the breathing rate was monitored by letting the participants read a short text aloud. This exercise program was a modified version of a program previously developed by Varkey et al. that was well tolerated by persons with migraine (11).
During the treatment period, participants filled out an exercise diary with information on date and form of exercise. Also, participants were encouraged to write down perceived side effects caused by exercising. They were allowed to miss a maximum of five lessons out of 36. The treatment period was followed by a post-treatment period, where participants could continue to exercise according to their own preference.
Control group
Participants in the control group were instructed to carry on with their daily life as usual. Every four weeks, they received an email asking them to submit the headache and NP diary. After follow-up, they were offered individually tailored physical therapy. This information was written in the participant information and repeated at the first visit with the physiotherapist (LSK).
Primary endpoint
The primary endpoint was a change in the number of days with migraine.
Secondary endpoints
Secondary endpoints were changes in: (a) the number of days with TTH and NP, (b) pain intensity, (c) pain duration, (d) area under the curve (AUC) of duration × pain intensity for migraine, TTH and NP, (e) physical fitness, (f) level of physical activity, (g) psychological well-being, and (h) perceived ability to perform daily activities.
All endpoints were assessed at baseline, at the end of treatment and at follow-up.
Statistical analysis
Sample size
Thirty participants were needed to detect a clinically relevant difference in migraine days of 30% with a power of 80% (26). To take drop-outs into account, 10 participants were added.
Clinical characteristics of the participants were presented descriptively as counts, percentages, or means and standard deviations.
Analyses of between-group differences were done per protocol from baseline to the end of the treatment period, and from baseline to the end of follow-up by applying the independent-samples t-test. If data were not normally distributed according to the Shapiro-Wilk test, they were transformed into natural logarithms. Transformed data were used to calculate two-tailed p-values and confidence intervals (CI).
The analyses of within-group changes were done by applying the Wilcoxon signed-rank test or the dependent samples t-test, depending on whether data were normally distributed (according to the Shapiro-Wilk test).
Participants who received beta blockers were excluded from the Åstrand’s submaximal bicycle test.
Responses to IPAQ that were clearly outside the maximum range of physical activity were treated as measurement errors and excluded from the analyses of MET-minutes/week.
Post hoc analyses were subsequently performed for changes between exercise and control groups from baseline to the end of the treatment period, and from baseline to the end of follow-up with regards to days with migraine for those with chronic migraine and for those without chronic migraine and co-existing TTH (hereafter called episodic migraine) in order to investigate whether these two groups may show different effects.
All statistical analyses were performed using IBM SPSS version 22. Statistical significance was assumed when p < 0.05.
Results
Seventy persons with migraine and co-existing TTH and NP were included, 62 women and 8 men (Figure 2).
Flow chart of the study procedure.
A total of 18 participants withdrew from the study after inclusion. There were no significant differences between participants who completed the study and those who withdrew with regards to age, sex, and chronic migraine.
Clinical characteristics of included persons with migraine and co-existing tension-type headache and neck pain.
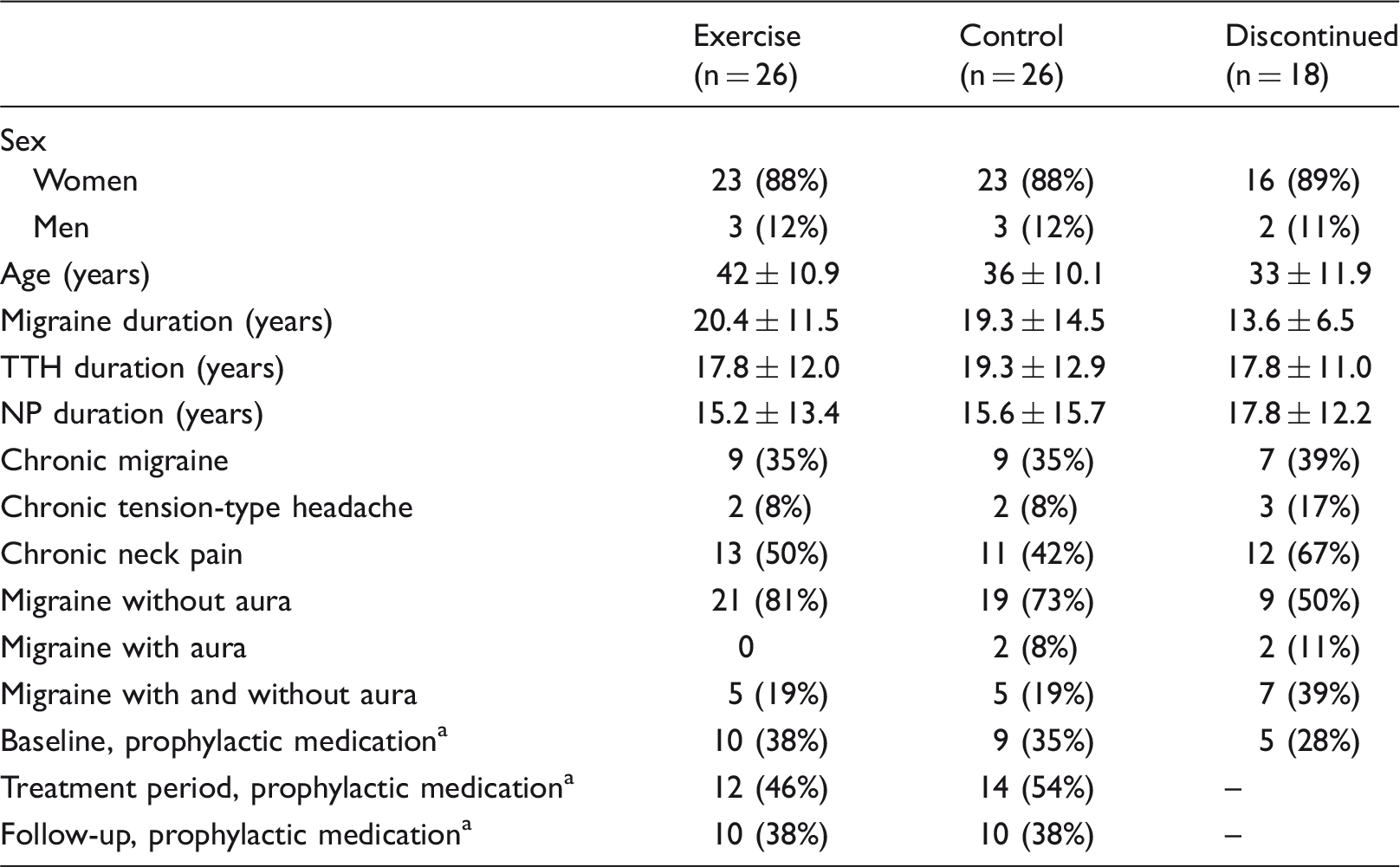
Numbers are presented as mean ± SD or number (%).
Beta blockers (used by 19% in exercise group, 12% in control group at baseline) and other preventives (topiramate, angiotensin II blockers, amitriptyline, catapressan and riboflavin).
Primary endpoint
Migraine, tension-type headache and neck pain variables, physical fitness, level of physical activity and well-being after 3 months treatment and at follow-up (six months from baseline).

Numbers are presented as mean (Standard Deviation).
Between-group differences were analysed by Independent Samples t-test from baseline to the end of treatment and from baseline to the end of follow-up.
Within-group differences were analysed by Wilcoxon signed-rank test from baseline to the end of treatment and from baseline to the end of follow-up.
p-value < 0.05.
AUC = area under the curve of duration × pain intensity.
Significant result.
Assessed using the Åstrand’s submaximal bicycle test to estimate the maximum oxygen uptake (VO2max).
Assessed using the International Physical Activity Questionnaire (IPAQ short form), MET-minutes/week equals the sum of walking, moderate and vigorous physical activity in minutes per week and multiplied by the metabolic equivalent task (MET) for each category.
Well-being assessed by the World Health Organisation five-item Well-Being Index (WHO-5) sum score from 0–100; lower scores indicate lower wellbeing.
Secondary endpoints
Between-groups differences
The ability to engage in daily activities owing to migraine, tension-type headache, and neck pain after 3 months treatment and at follow-up (six months from baseline).

Numbers are presented as mean (Standard Deviation).
Between-group differences were analysed by Independent Samples t-test from baseline to the end of treatment and from baseline to the end of follow-up.
Within-group differences were analysed by Dependent Samples t-test from baseline to the end of treatment and from baseline to the end of follow-up.
p-value < 0.05.
Variables were rated on an 11-point numeric rating scale with the end points 0 = no impact and 10 = most imaginable impact.
Social activities not including family activities.
Participation in family activities.
Significant result.
An increase in MET-minutes/week (p = 0.033) (Table 2), and improvements in the ability to perform daily activities because of reduced migraine impact were also observed from baseline to follow-up (Table 3). The ability to engage in household chores (p = 0.022) and physical activity (p = 0.042) because of reduced impact of TTH and physical activity because of reduced impact of NP (p = 0.004) was improved from baseline to follow-up (Table 3).
Within-group differences
In the exercise group, there was significant reduction in migraine pain intensity (p = 0.005), migraine duration (p = 0.045), migraine AUC (p = 0.034) and in NP intensity (0.045) from baseline to the end of treatment. Migraine variables and NP intensity were also reduced from baseline to follow-up except for migraine AUC. Physical fitness (p = 0.014) and psychological well-being (p < 0.001) improved significantly from baseline to the end of treatment. Psychological well-being was also significantly improved at follow-up (Table 2). The ability to engage in all daily activities because of reduced impact of migraine was significantly improved, and for some activities because of reduced impact of TTH and NP after treatment and at follow-up (Table 3).
The post hoc analyses of days with migraine in chronic and episodic migraine respectively showed no differences between the exercise group and control groups. Within the exercise group, the changes of days with migraine from baseline to the end of treatment and from baseline to follow-up in chronic migraine decreases were observed from 16 to 11 days (31%; p = 0.19) and from 16 to 9 days (44%; p = 0.018) respectively. In episodic migraine, decreases were observed from 7 to 6 days (14%; p = 0.12) and from 7 to 5 days (29%; p = 0.098) respectively (Figure 3).
Median changes in migraine frequency in days per month from baseline to end of treatment and to follow-up (six months from baseline).
The exercise group reported no side effects caused by training.
Discussion
To our knowledge, this is the first study to evaluate the effect of aerobic exercise on persons suffering from migraine and co-existing TTH and NP. The exercise group improved from baseline; however, no between-group difference was found for the primary endpoint, migraine frequency. The burden of migraine was significantly reduced from baseline, and significant between-group reductions were found in the exercise group compared to the control group.
Earlier RCT studies (4,9,10) have investigated the effects of aerobic exercise for persons with migraine. The methodologies used differed from ours and the results are, therefore, difficult to compare. However, the improvement of migraine in our exercise group is in line with the conclusion of the systematic review and meta-analyses by Luedtke et al. (2016) (6).
We did not find any between-group differences for TTH and NP severity. However, in the exercise group, the ability to engage in physical activity was significantly improved after treatment because of reduced impact of TTH and at follow-up because of reduced impact of TTH and NP compared to the control group. Previous studies have found that the prognosis of migraine may deteriorate with co-existing TTH (16), and that NP was a predictor of disability in migraine (17). Consequently, all three conditions need to be addressed and may require different treatment strategies.
The exercise group significantly improved their physical fitness after treatment compared to controls, but this effect was not observed at follow-up. It seems that the higher level of physical activity was maintained by the exercise group after the treatment period, but this was not enough to keep the level of improved physical fitness. A certain level of physical fitness may be needed to reduce migraine frequency over time, as suggested by Hagen et al. in a cross-sectional study that linked a high level of physical fitness with lower migraine prevalence (13).
Both groups significantly improved their psychological well-being. The improvement of the control group is likely a time effect phenomenon and/or positive expectations of future treatment (27), since the control group was offered individual tailored physiotherapy after follow-up.
The burden of migraine on the ability to engage in daily activities was significantly reduced in the exercise group compared to controls, together with the improved ability to engage in physical activity owing to reduced impact of TTH and NP. These effects may be explained by a positive alteration of avoidance behaviour, which is a known phenomenon in persons with headache and musculoskeletal pain conditions (28–30). This confirms that being physically active can reduce the negative impact of migraine on daily activities.
In the post hoc analyses, we did not find any differences between the exercise and control groups in migraine days for chronic and episodic migraine respectively. However, for chronic migraine a larger relative reduction in migraine days at follow-up was observed than for episodic migraine. Santiago et al. (9) showed significant positive effect of aerobic exercise on persons with chronic migraine. However, further studies are needed to confirm these findings.
Strengths and limitations
Strengths of the present study were its randomized design, high internal validity of headache diagnoses based on headache diaries, detailed headache history and examinations by a neurologist and physiotherapist. Secondary headaches were excluded. The frequency of headache and NP, pain intensity, duration and acute medication intake were reported by the participants as previously recommended (31). Finally, the degree of physical activity and physical fitness were assessed for both groups, and the exercise group also recorded physical activity in an exercise diary. These recordings provided us with detailed information on the level and degree of physical activity for both groups.
The use of a diagnostic diary to record days with migraine, TTH and NP is a strong instrument to reduce recall bias. However, occasionally it can be difficult to distinguish between a day with TTH and a day with migraine in persons with very frequent headaches. If any doubts arose, these were discussed among the headache experts of the study group and a consensus diagnosis was applied.
We designed this study as an add-on treatment, and did not make any demands for regulation of prophylactic medication in either group to reflect daily clinical practice. This may have influenced the results.
Even though the aerobic exercise program provided varied movements, such as biking, cross-training and brisk walking, this was not enough to show any significant between-group differences with regards to frequency, pain intensity and duration of TTH and NP. Consequently, different treatment modalities may be considered for future studies.
There was a drop-out rate of 28% in the exercise group and 24% in the control group, which could have increased the risk of type II errors. The reason for dropping out of a study is important, because drop-outs’ symptoms might have improved or worsened. However, in the present study we have evaluated participants in total including those who have improved, who did not have any change of symptoms, and who have worsened. We, therefore, believe our results to be realistic, but they should obviously be confirmed in future studies. Earlier reviews of the effect of exercise on persons with headache have recommended future studies to include a higher number of participants in order to increase power (6,31); however, recruiting participants for these kinds of active interventions with a long follow-up period is rather challenging, costly, and time consuming.
All participants were provided with a leaflet about possible migraine triggers, which could potentially have influenced the course of the study. However, avoiding triggers is part of the standard of care protocol at this level of specialized care, and information about triggers is also easily accessible online. We, therefore, consider the effect of this information to be limited.
Participants in the control group were offered individually tailored physiotherapy after the study period instead of the standard aerobic exercise program. This may have increased positive expectations of future treatment (27) and possibly affected several measures such as psychological well-being.
There was a possible selection bias, because persons who are interested in physical activity as a treatment for headache are more likely to sign up for such a type of study.
There were no specified requirements with regards to level of physical activity before entering the study, and the control group were not asked to stop exercising during the intervention period. However, the exercise group were significantly more physically active and significantly improved physical fitness compared to the control group after treatment, and the control group significantly decreased their level of physical activity during this period. Thus, the pre-study level of physical activity may have been limited as a confounder.
We recruited participants both from a tertiary referral headache centre and via advertisement. Almost half of the participants suffered from chronic headache and do not, therefore, represent a normal headache population. Also, our participants all suffered from TTH and NP besides their migraine, which may add to the symptom burden compared to those who suffer from migraine only.
The persons who conducted the test of physical fitness were not blinded to the participants’ grouping. This could possibly affect the results. However, this influence may be limited, as the test was controlled by a software program that required stable heart rate and predetermined speed, otherwise the test would fail.
Perspectives
A large subset of persons with migraine suffers from co-existing TTH and NP (1,32). In the present study, we separated these conditions in the analyses and our results indicate the need for different treatment modalities. The general health benefits of physical activity are well documented in healthy adults (14). This study showed that regular aerobic exercise significantly reduced the burden of migraine on the ability to engage in daily activities, and improved the ability to engage in physical activity owing to reduced impact of TTH and NP. In line with Varkey et al. (10), we found aerobic exercise to be safe to implement among our participants.
Conclusions and recommendations
There was no between-group difference for the primary endpoint, migraine frequency. However, a significant reduction was found in the exercise group for migraine frequency, pain intensity and duration of migraine, but no between-group differences. The group that engaged in aerobic exercise significantly improved the burden of migraine on daily activities and the ability to engage in physical activity owing to reduced impact of TTH and NP compared to controls. No between-group differences were observed for TTH and NP severity. This study underlines the importance of regular aerobic exercise for a reduction of migraine burden on daily activities.
Clinical implications
Migraine burden can be reduced by aerobic exercise. Aerobic exercise can improve the ability to engage in general physical activity. Aerobic exercise is safe for persons with migraine and co-existing tension-type headache and neck pain.
Footnotes
Acknowledgement
The authors wish to thank all participants for their cooperation; Hanne Andresen, technician, for assistance in testing the participants, and Maria Lurenda Westergaard for language editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study has been supported by the Medical Faculty of Lund University, Lund, Sweden, and the Danish Headache Centre, Rigshospitalet-Glostrup, Denmark. The study has been financially supported by Research grants from Rigshospitalet-Glostrup, Lundbeck Foundation, Aase and Ejnar Danielsen’s Foundation, Cool Sorption Foundation of 1989, Danish Physical Therapists’ foundation for research, education and practice development, The Association of Danish Physiotherapists’ Practice Foundation and The Danish Migraine and Headache Association. Our funders had no influence over the structure of analytical methods or the presented results.