
Abstract
Aim:
To systematically review the available literature on the prevalence and clinical characteristics of headache in patients with Tourette syndrome (TS), a neurodevelopmental condition characterized by the chronic presence of motor and vocal tics.
Design:
We conducted a systematic literature review of original studies using three clinical databases (Medline, EMBASE and PsycInfo), according to the standards outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Outcome measures included both tic severity and tic frequency.
Results:
Our systematic literature review identified six studies on the prevalence and characteristics of headache in patients with TS (data on paediatric patients were available from five studies and data on adult patients from four studies). The proportion of patients with TS who had a diagnosis of headache ranged from 29% to 62%. Migraine was the most commonly investigated headache disorder in this patient population. The findings of the reviewed studies showed that the prevalence of migraine in patients with TS ranges between 13% and 43% and is significantly higher compared to the two control groups (p < 0.05).
Discussion:
The prevalence of headache in patients with TS could be higher than in the general population, with the most reliable data being available for migraine. Overall, the literature on the prevalence and characteristics of headache in TS is sparse and highly heterogeneous. Further research on the prevalence and clinical correlates of migraine, tension-type headache and other types of headache in patients with TS across the lifespan is needed to inform clinical practice aimed at improving health-related quality of life in patients with tics.
Introduction
Tourette syndrome (TS) is a complex neurodevelopmental disorder characterized by the chronic presence of multiple motor tics plus at least one vocal tic since childhood or adolescence. 1,2 Tics are defined as sudden, involuntary, repetitive, non-rhythmic movements and vocalizations and are characteristically preceded by sensory experiences (‘premonitory urges’). 3,4 It is estimated that 0.3–1% of school-age children fulfil the diagnostic criteria for TS, with differing degrees of severity. 5,6 The majority of patients with TS present with co-morbid conditions, including obsessive–compulsive disorder (OCD) and attention-deficit and hyperactivity disorder (ADHD), as well as frequent affective symptoms and impulsivity. 7 Over the last few decades, there has been growing interest in co-morbid psychiatric disorders (especially tic-related OCD and ADHD), in consideration of their impact on patients’ health-related quality of life across the lifespan. 7 –9 Relatively little is known about the neurological co-morbidities of TS, despite reports of neurological soft signs 10 and increased risk for common neurological conditions such as epilepsy. 11 Moreover, pain is increasingly being recognized as a prominent feature of TS, presumably of multifactorial origin. 12
The association between TS and headache has been investigated in a number of observational studies, suggesting an increased prevalence of headache in patients with TS. However, to date, there has been no systematic review summarizing and critically appraising these findings. Specifically, little is known about the prevalence of different types of headache in patients with TS, as well as the clinical correlates of headache in this patient population. A better understanding of the relationship between TS and headache could shed some light on the possible pathophysiological mechanisms leading to the development of both tics and specific headache types. Moreover, evidence-based knowledge on this aspect of TS would enable clinicians to improve diagnostic and therapeutic strategies for patients. We, therefore, set out to conduct a systematic literature review on the prevalence of the main different types of headache and their clinical correlates in patients with TS.
Methods
This systematic literature review was conducted in accordance to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, 13 used in conjunction with the Explanation and Elaboration document. 14 We included in our review all studies on the prevalence and clinical characteristics of headache in patients with a formal diagnosis of TS according to the Diagnostic and Statistical Manual for Mental Disorders (DSM) criteria. 1 Only studies in which headache was diagnosed using criteria outlined by the International Classification of Headache Disorders (ICHD) or criteria matching those set by the ICHD (in studies that did not explicitly mention ICHD criteria) were considered for inclusion. 15 Case series and case single reports were excluded from this review, as well as study abstracts without the availability of full texts.
The searches were conducted on three clinical databases: Medline, EMBASE and PsycInfo. The search terms were as follows: ‘Tourette*’ OR ‘Tic*’ AND ‘Headache*’ OR ‘Migrain*’. For comprehensiveness, the reference lists of eligible articles were also screened to identify any relevant articles. Google Scholar was used to search for the grey literature. Since a few of the reviewed studies were published in the same scientific journals, the contents of relevant journals, including Cephalalgia, Headache, Movement Disorders, Journal of Neurology Neurosurgery and Psychiatry and Journal of Neuropsychiatry and Clinical Neurosciences, were manually searched for any further articles on the reviewed topic. We did not limit our search to articles published in English language, and there were no chronological, geographic or demographic limitations to the inclusion of studies. Both qualitative and quantitative study designs were included for review. The Crowe Critical Appraisal Tool (CCAT) was used to assess the quality of the selected studies, and any studies scoring less than 30% were excluded from the review. 16,17
Results
Our systematic literature search yielded a total of 1144 articles, after removal of duplicates. A manual search of reference lists for relevant articles yielded a further 12 articles, for a total of 1156 articles. Of these, 44 were considered relevant to the review and their full texts were inspected, after 8 studies were excluded because their full texts were not available. A total of 10 articles that looked at headache prevalence in TS, but did not include ICHD criteria or criteria consistent with ICHD standard as part of their study, were excluded from the present review. Seven articles (corresponding to six independent studies) met all the inclusion criteria and were included in the present review (Figure 1). 18 –24

PRISMA flow diagram outlining the identification, screening, assessment for eligibility and inclusion of studies in the present review. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The six independent studies, summarized in Table 1, involved a total of 465 patients with TS (average sample size 78 patients; range 21–140 patients).
Summary of studies on headache in patients with TS.
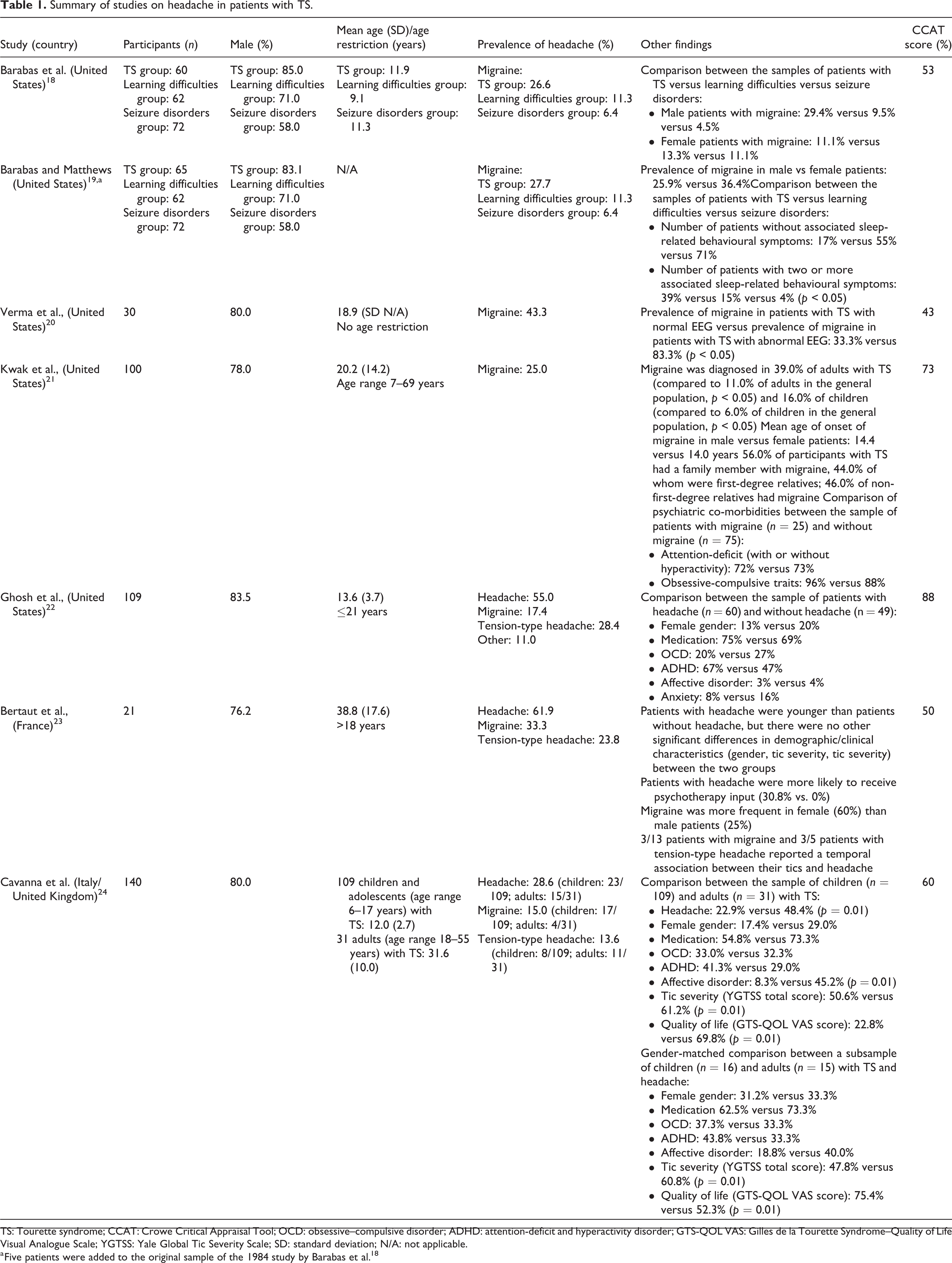
TS: Tourette syndrome; CCAT: Crowe Critical Appraisal Tool; OCD: obsessive–compulsive disorder; ADHD: attention-deficit and hyperactivity disorder; GTS-QOL VAS: Gilles de la Tourette Syndrome–Quality of Life Visual Analogue Scale; YGTSS: Yale Global Tic Severity Scale; SD: standard deviation; N/A: not applicable.
a Five patients were added to the original sample of the 1984 study by Barabas et al. 18
DSM-validated criteria for the diagnosis of TS were used in four studies, 18 –20,22,24 the diagnostic criteria developed by the Tourette Syndrome Classification Study Group were used in one study, 21 and formal diagnosis of TS with no explicit reference to published criteria was established in one study. 23 The ICHD criteria for the diagnosis of headache were used in four of the reviewed studies, 21 –24 and criteria for the diagnosis of headache that were consistent with the ICHD standards were used in two studies published before the introduction of the ICHD criteria. 18 –20 Data on paediatric patients were available from five studies 18 –22,24 and data on adult patients from four studies. 20,21,23,24 Table 2 details the quality assessment of the reviewed studies on headache in patients with TS, with individual CCAT scores.
Quality assessment of the reviewed studies on headache in patients with TS, with individual CCAT scores.

TS: Tourette syndrome; CCAT: Crowe Critical Appraisal Tool.
Three of the included studies reported prevalence figures for overall headache, migraine and tension-type headache in patients with TS. 22 –24 The remaining three studies focused on the prevalence of migraine only. 18 –21
The prevalence of overall headache in patients with TS ranged from 28.6% to 61.9%, whereas the prevalence of tension-type headache ranged from 7.3% to 35.5%. Migraine was found to be the most researched headache disorder with regard to its association with TS, as all of the included studies investigated the prevalence of this headache disorder in clinical samples of patients with TS: the reported prevalence figures ranged from 12.9% to 43.3% (Table 3).
Prevalence of migraine in patients with TS.

TS: Tourette syndrome.
One study found that migraine was significantly more frequent in children with TS compared to adults with TS, whereas the prevalence of tension-type headache followed the opposite pattern. 24 One study reported the prevalence of other types of headaches to be 11.0%. 22
The presence of co-morbid disorders was not found to be associated with significantly higher rates of headache in patients with TS. 22,23 Although the presence of attention-deficit and hyperactivity symptoms and obsessive–compulsive symptoms was not significantly associated with higher rates of migraine, 21 co-morbid sleep-related behavioural symptoms and abnormal electroencephalographic (EEG) findings were associated with significantly higher rates of migraine in patients with TS. 19 Finally, the results of one study showed that adults with TS and co-morbid headache consistently presented with higher tic severity and poorer quality of life compared to children with TS and co-morbid headache (p = 0.01). 24
Discussion
We conducted the first systematic literature review on the prevalence and clinical correlates of headache in patients with TS. Our search yielded 6 studies, involving a total of 465 patients with TS. 18 –24 The three studies that assessed the overall prevalence of headache in patients with TS found that headache is a commonly reported condition in this patient population, with prevalence figures ranging from 28.6% to 61.9%. 22 –24 Of note, the reported prevalence of headache in adults with TS (range 48.4–61.9%) 23,24 was higher than the prevalence of headache in the general adult population as reported in a 2007 documentation of headache prevalence and disability worldwide. 25 However, based on the World Health Organization’s atlas of headache disorders published in 2011, 26 the 1-year prevalence of headache globally for adults age 18–65 ranged from 21.6% in African countries to 78.8% in the Eastern Mediterranean (46.5% in the Americas): a range of prevalence data that is not significantly different from the one we observed in the TS population. With regard to the clinical correlates of headache in patients with TS, there was no evidence of any significant association between the presence of headache and gender, tic severity, or co-morbid conditions. 22 –24
The prevalence of migraine in clinical samples of patients with TS was investigated in all the reviewed studies, with figures ranging from 12.9% to 43.3%. 18 –24 Studies investigating adult patients with TS reported migraine prevalence figures of 12.9–39.0%, 21,23,24 whereas studies investigating paediatric patients with TS reported migraine prevalence figures of 15.6–27.7%. 18,19,21,22,24 Only one study reported the prevalence of migraine in two control groups consisting of paediatric patients with other neurological conditions (learning difficulties and seizure disorders). 18,19 The results of this study showed a significantly higher prevalence of migraine in patients with TS compared to those with learning difficulties and seizure disorders (p < 0.05). The prevalence of migraine in patients with TS could be higher than the figures reported in the general population. 25 –27 Taken together, the results of our systematic literature review are in line with previous reports of increased prevalence of migraine in the TS population. 11 With regard to the clinical correlates of migraine in TS, the level of evidence for gender differences was overall low. 19,21,23 Common psychiatric co-morbidities such as ADHD symptoms and obsessive–compulsive traits did not appear to be associated with a higher prevalence of migraine in patients with TS. 21 Finally, both abnormal EEG findings 20 and sleep-related behavioural symptoms 19 appeared to be more common in patients with TS and migraine.
Based on the findings of epidemiological and clinical studies, a number of hypotheses have been suggested to explain the increased prevalence of migraine in the TS population. The proposed models can be grouped into three categories: common disturbance of serotonin metabolism, common disturbance in the extrapyramidal system and common genetic aetiologies between migraine and TS. The hypothesis of a shared pathophysiological basis is in line with the available evidence of altered serotonin metabolism in both conditions. 18,21,24,28,29 Interestingly, the results of a functional neuroimaging study showed that patients with TS and co-morbid OCD had significantly increased levels of dopamine alongside increased serotonin binding potential compared to patients with TS without OCD and to healthy controls. 30 These findings would be consistent with the hypothesis that specific TS-OCD phenotypes (i.e. patients with TS and tic-related obsessive-compulsive behaviours) might be selectively associated with migraine. If confirmed by further studies, this hypothesis might have wide-ranging implications for clinical practice, as the serotonergic agents used to treat OCD are also beneficial for anxiety and affective symptoms, a common co-morbidity of both TS and migraine. 24,31 –33 A shared disturbance in the extrapyramidal system has also been proposed, mainly based on neuroimaging findings showing the involvement of basal ganglia–thalamocortical circuitries. 34,35 Specifically, functional magnetic resonance imaging has provided the strongest finding pointing to a role of the basal ganglia in the pathophysiology of migraine, 34 whereas both structural and functional neuroimaging studies have suggested the involvement of the basal ganglia in the pathophysiology of tic disorders. 35 More recently, large-scale genetic studies including genome-wide association studies have paved the way for the study of possible shared hereditability patterns for TS and migraine. 36,37 The possibility of genetic associations between TS and migraine would benefit from further investigations. For example, Ganos et al. reported the case of a male adolescent with TS, co-morbid ADHD, obsessive–compulsive behaviour and autism spectrum disorder, as well as additional paroxysmal kinesigenic dyskinesia resulting from PRRT2 mutation misdiagnosed as complex tics. Interestingly, the authors of this case report were prompted to screen for mutations in the PRRT2 gene by the significant family history of migrainous headaches, as well as the reported infantile convulsions of both the patient and his mother. 38
The three studies investigating the prevalence of tension-type headache in samples of patients with TS found prevalence figures ranging from 7.3% to 35.5%. 22 –24 Specifically, tension-type headache was diagnosed in 7.3–28.4% of children with TS 22,24 and 23.8–35.5% of adults with TS. 23,24 These preliminary findings appear to be broadly in line with epidemiological data from the general population, 25 however, it is difficult to draw any firm conclusion from a small number of studies with limited sample sizes. The results of the only study comparing children and adults with TS 24 complemented the findings of a recent study on a large sample of 401 patients with headache, suggesting that psychiatric symptoms and social stressors were associated significantly more often with tension-type headache than with migraine. 39 None of the reviewed studies investigated the clinical correlates of tension-type headache in TS or reported the frequency of tension-type headache in control groups. Likewise, only one study investigated the prevalence of other types of headache (aura followed by non-migraine headache, headache attributed to depressive disorder, primary stabbing headache, headache attributed to cervical myofascial pain due to tic-related pericranial muscle overuse), reporting a figure of 11% in a sample of 109 paediatric patients with TS. 22 Clearly, further investigation is warranted in this area, with particular attention to the characterization of the burden of headache secondary to tics.
The present systematic literature review has limitations. We found that there is a relative paucity of high-quality data: a total of six independent studies met our inclusion criteria. The reviewed studies were highly heterogeneous in terms of diagnostic criteria, research protocols, patient groups (some studies focused on children, whereas others investigated adult samples). Moreover, most studies did not report prevalence figures for headache in matched control groups. The level of clinical heterogeneity was deemed too high to conduct a meta-analysis on the available data. The diagnostic criteria for both TS and headache have changed over time, raising the possibility that the results of some of the older studies might not be transferable or reproducible in patients who were diagnosed more recently. Finally, the reviewed studies recruited patients through tertiary referral centres, where more complex and severe cases of TS tend to be seen. Therefore, referral bias might limit the generalizability of our findings to the wider TS population.
In summary, the first systematic literature review on the association between headache and TS found that the prevalence of headache in patients with TS could be higher than in the general population, with the most reliable data being available for migraine. Overall, the literature on the prevalence and characteristics of headache in TS is sparse and highly heterogeneous. Further research on the prevalence and clinical correlates of migraine, tension-type headache and other types of headache in patients with TS across the lifespan is needed to inform clinical practice aimed at improving health-related quality of life in patients with tics. Specifically, if the association between TS and migraine is confirmed by future research on larger populations, there could be relevant implications for clinical practice. For example, topiramate, a pharmacological agent used for migraine prophylaxis, has been included in the recently published guidelines on the treatment of tics of the American Academy of Neurology. 40 –43 A better understanding of the relationship between migraine and tics could assist in the characterization of TS phenotypes and improve diagnostic and treatment strategies.
Footnotes
Acknowledgements
Gratitude is expressed to Tourettes Action UK and Tourette Association of America for their ongoing support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.