
Abstract
Objective:
To systematically review the vascular effects of glibenclamide.
Background:
Infusion of adenosine triphosphate (ATP)-sensitive potassium (KATP) channel opener (KCO) levcromakalim dilates cranial arteries and induces headache and migraine attacks. Recent data show that levcromakalim-induced vasodilation is associated with headache. Glibenclamide is a KATP channel blocker that may alter the vascular tone and thus has an impact on headache or migraine prevention.
Methods:
A search through PubMed was undertaken for studies investigating the vascular effects of glibenclamide in vitro as well as in vivo published until July 2019.
Results:
We identified 58 articles; 31 in vitro studies, 24 in vivo studies and 3 studies with both. The main findings were that glibenclamide inhibited levcromakalim-induced and other KCOs-induced vasodilation, while the basal vascular tone remained unchanged.
Conclusion:
Glibenclamide could inhibit vasodilation by KCOs, and further studies are needed to clarify the vascular effect of glibenclamide on human cranial arteries.
Introduction
Recent studies implicated the adenosine triphosphate (ATP)-sensitive potassium (KATP) channels in migraine pathophysiology 1 and suggested that KATP channel blockers might have potential as novel treatments for migraine. 2 KATP channels are found in several tissues including pancreatic α- and β-cells and smooth muscle cells in cranial arteries. 3 The activity of KATP channel is crucial for controlling insulin secretion and vascular tone. Intravenous infusion of KATP channel opener (KCO) levcromakalim provokes headache in healthy volunteers and migraine attacks in migraine patients. 2 The precise mechanisms by which the opening of KATP channels induces headache in healthy volunteers and migraine attacks in migraine patients are unclear. Interestingly, levcromakalim dilates cranial arteries and the dilation is associated with headache. 4 Thus, the vasodilation upon KATP channel activation is relevant, but whether KATP channel inhibition could affect cranial arteries and thereby prevent headache is unknown. The widely used antidiabetic drug glibenclamide is a KATP channel blocker that belongs to the second generation of sulfonylurea. 5 Here, we performed a systematic review on the vascular effect of glibenclamide in vitro and in vivo.
Method
Search strategy
We searched PubMed for articles on the vascular effect of glibenclamide with a focus on cranial arteries. Three full searches were performed by using keywords and PubMed’s vocabulary thesaurus for indexed articles called Medical Subject Headlines (MeSH).
The first search was performed to find articles investigating the effect of glibenclamide combined with KCOs or other vasoactive compounds and consisted of three parts: (1) terms for the vascular effect; (2) terms for glibenclamide; and (3) terms for KCOs such as levcromakalim, cromakalim, lemakalim, bimakalim, SR47063, pinacidil and diazoxide, and other vasodilators including Pituitary adenylate cyclase activating polypeptide (PACAP), Calcitonin gene-related peptide (CGRP), vasoactive intestinal peptide, Glyceryl trinitrate (GTN), sildenafil, cilostazol, nicorandil, histamine, acetylcholine, and noradrenaline.
Keywords used in the search database were (1) “Blood Vessels” [MeSH], “Vasoconstriction” [MeSH], “Vasodilation” [MeSH], “Vascular Resistance” [MeSH], “Blood Pressure” [MeSH], “Vasoconstriction” “Vasodilation”, “Blood Vessels,” “Vascular Resistance,” and “blood pressure” AND (2) “Glyburide” [MeSH], “Glyburide,” “Glibenclamide,” “Diabeta,” “Euglucon 5,” “Neogluconin,” “HB-419,” “HB 419,” “HB419,” “HB-420,” “HB 420,” “HB420,” “Maninil,” “Micronase,” “Daonil,” “Euglucon N” AND (3) “Cromakalim” [MeSH], “Cromakalim,” “Lemakalim,” “Levcromakalim” “bimakalim”, “SR47063,” “pinacidil” [MeSH], “diazoxide” [MeSH], “calcitonin-gene related peptide” [MeSH], “pituitary adenylate cyclase-activating polypeptide” [MeSH], “vasoactive intestinal peptide” [MeSH], “glyceryl trinitrate” [MeSH], “sildenafil” [MeSH], “cilostazol” [MeSH], “nicorandil” [MeSH], “histamine” [MeSH], “acetylcholine” [MeSH], “noradrenaline” [MeSH]. Articles were restricted to English language and reviewed initially by title and abstract and then full text to confirm eligibility for the systematic review.
The second search was performed to find articles investigating the combined effect of glibenclamide and levcromakalim on cranial arteries. The search consisted of three parts: (1) terms for cranial arteries, (2) terms for glibenclamide, and (3) terms for KCOs or other vasoactive compounds. Keywords for the two latter search parts were the same as for the first search, while the first part consisted of the following: (1) “Vertebral Artery” [MeSH], “Meningeal Arteries” [MeSH], “Basilar Artery” [MeSH], “Carotid Arteries” [MeSH], “Cerebral Arteries” [MeSH], “Vertebral Artery,” “Meningeal Arteries,” “Basilar Artery,” “Carotid Arteries,” “Cerebral Arteries” and were processed in the same manner as the first search.
The third search was performed to find articles investigating the basal effect of glibenclamide upon cranial arteries. The search consisted of two parts: (1) terms for cranial arteries and (2) terms for glibenclamide. The search parts were the same as the respective terms in the second search and were processed in the same manner as the previous searches. A search flowchart is depicted in Figure 1.

Flowchart of search protocol. *Records excluded due to search criteria:
The search was completed on July 15, 2019. Articles were restricted to English language and reviewed first by title and abstract and then full text to confirm eligibility for this review. Furthermore, a review of reference lists from the included articles was performed to identify supplementary works not included through the initial search protocol. Two reviewers (MMK and MS) assessed the eligibility of the records found, and disagreements were resolved through discussion.
Results
Our search protocol identified 772 articles, of which 58 were included. There were 31 in vitro studies, 24 in vivo studies, and 3 studies with both. Altering of basal vascular tone after glibenclamide was investigated in vitro in 16 studies and in vivo in 12 studies. Glibenclamide effects on KCOs-induced and other vasoactive compounds-induced vasodilation were examined in vitro in 31 studies and in vivo in 21 studies. These studies show that glibenclamide attenuated KCO-induced vasodilation without altering the basal resting vascular tone.
Discussion
The major finding of the present review is that targeting KATP channels has no vasoconstriction effect at the basal resting vascular tone. However, glibenclamide attenuates vasodilation induced by levcromakalim and other KCOs. Interestingly, the shown glibenclamide effect is like the effect of the new CGRP monoclonal antibodies that only constrict pre-dilated arteries without altering the basal tone. 7 The relationship between glibenclamide and other vasoactive compounds known to provoke migraine attacks such as CGRP and GTN was contradictory. Furthermore, there is no information about the in vivo glibenclamide effect on human cranial arteries.
In vitro human and animal studies
Table 1 summarizes the main findings. The general methods used in vitro studies were arterial segments or cell cultures in organ baths measured by myographs, patch clamps, or strain gauges. These studies used tissues/cells from different species including human, rat, rabbit, pig, canine, and feline. The common finding is that glibenclamide attenuated KCOs-induced vasodilation without altering the basal vascular tone. However, two studies fall outside that classification. One study with canine middle cerebral artery (MCA) and basilar arteries reported that glibenclamide decreased the basal tone. 23 Another study with rat tissues showed that glibenclamide increased the basal tone of the meningeal artery, while the basal tone of the superior cerebellar arteries remained unchanged. 30 The expression of KATP channel in smooth muscle cells and endothelial cells may explain why endothelium removal is not essential for KATP channel activity. These data further support previous findings that endothelium removal decreased the sensitivity of basilar arteries, but not of MCAs to levcromakalim, and the maximum relaxant response was stronger in basilar arteries with endothelium than without endothelium. 28
Summary of the in vitro experiments.a
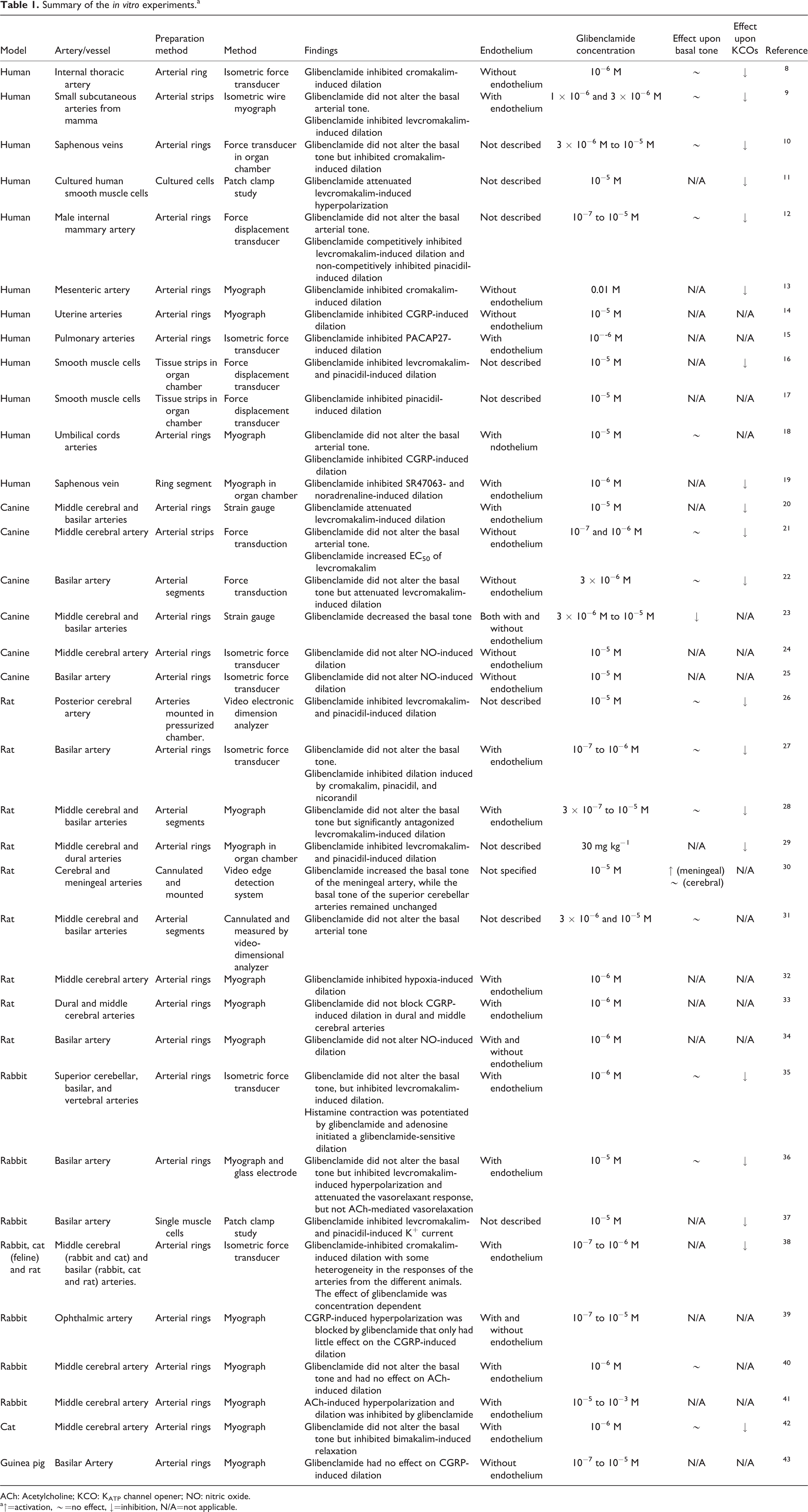
ACh: Acetylcholine; KCO: KATP channel opener; NO: nitric oxide.
a↑=activation, ∼=no effect, ↓=inhibition, N/A=not applicable.
The relationship between glibenclamide and other vasoactive compounds known to trigger headache/migraine was contradictory. Histamine contraction was potentiated by glibenclamide in superior cerebellar, basilar, and vertebral arteries isolated from rabbit. 35 Glibenclamide inhibited PACAP27-induced dilation in human pulmonary arteries 15 and did not alter nitric oxide (NO)-induced dilation. 24,25,34
Glibenclamide inhibited CGRP-induced relaxation in human uterine 14 and umbilical cords arteries. 18 However, glibenclamide did not alter CGRP-induced dilation in pig basilar artery 43 and in rat dural arteries and MCAs. 33 Another study with rabbit ophthalmic artery showed that CGRP-induced hyperpolarization, which partially leads to dilation in smooth muscle cells, was blocked by glibenclamide, while the CGRP-induced dilation remained largely unaffected. 39
Glibenclamide did not alter acetylcholine (ACh)-induced dilation in rabbit MCAs 40 and basilar arteries. 36 Another study with rabbit MCA showed that glibenclamide inhibited ACh-induced hyperpolarization and dilation. 41
In vivo animal studies
The closed cranial window was the main method used to investigate the effect of glibenclamide in animal models in vivo, and the results are summarized in Table 2. Glibenclamide did not alter the basal vascular tone but attenuated KCOs-induced vasodilation. In contrast, two studies showed that glibenclamide increased the basal tone in rat dural artery including middle meningeal artery. 29,30
Summary of the in vivo experiments.a

KCO: KATP channel opener; NO: nitric oxide; Ach: acetylcholine.
a↑=activation, ∼=no effect, ↓=inhibition, N/A=not applicable.
Glibenclamide inhibited CGRP-induced dilation in rat basilar and pial arteries. 51,52 However, one study reported that glibenclamide attenuated CGRP-induced dural dilation without affecting CGRP-induced pial dilation. 33
Glibenclamide did not alter ACh-induced dilation in rat basilar artery 55 and NO-induced dilation in rat basilar, dural, and pial arteries. 33,53,61 Glibenclamide attenuated opioid-induced pial artery dilation in neonatal pigs, 62 and PGE2- and PGI2-induced pial arteries dilation in neonatal pigs. 65
In vivo human studies
To date, no studies have been carried out investigating the in vivo effects of glibenclamide on human cranial arteries. Studies in patients with brain swelling after large hemispheric infarction reported safety and efficacy of intravenous glibenclamide but did report its effect on cerebral hemodynamics or on heart rate and blood pressure. 49,66 One study reported that single treatment with oral glibenclamide increased systolic but not diastolic blood pressure compared with placebo. 67 Another study reported no difference between mean systolic and diastolic blood pressure and heart rate after daily treatment with oral glibenclamide over a month compared with placebo. 45
In humans, glibenclamide inhibited sildenafil-induced radial artery dilation, 48 and attenuated sodium nitroprusside-, ACh-, and methacholine-induced cutaneous vasodilation. 46,47 Furthermore, glibenclamide abolished the vascular effect on forearm blood flow caused by nicorandil (pharmacological drug with dual function, KATP channel opener and NO donor). 44 Interestingly, CGRP-induced forearm vascular dilation was largely unaffected. 68
Future perspectives
Glibenclamide is a highly lipophilic KATP channel blocker that belongs to second-generation sulfonylureas. 5 Sulfonylurea compounds were originally proposed to be antimicrobial agents, but the common side effect was hypoglycemia due to the inhibition of pancreatic β-cell KATP channels. 69 Currently, they are widely used in clinical practice as antidiabetic drugs, 69 and several generations of sulfonylureas are available; first generation (tolbutamide), second generation (gliclazide, glipizide, and glibenclamide), and third generation (glimepiride). 5 Sulfonylureas bind and cause KATP channel closure, which results in depolarization and cell/tissue-specific signaling pathway. KATP-channel is a hetero-octameric complex consisting of four pore-forming K+ inwardly rectifying (Kir) subunits and four regulatory sulfonylurea receptor (SUR) subunits. 1 Kir subunits are expressed with two isoforms: kir6.1 and kir6.2, while SUR subunits are expressed with three isoforms SUR1, SUR2A, and SUR2B. KATP-channel expression with different compositions of Kir6 and SUR subunits leads to distinct functional properties in different tissues. 1 The binding of sulfonylureas to KATP-channel is isoform dependent; with a concentration in the therapeutic window, tolbutamide and gliclazide bind only to SUR1, whereas other types of sulfonylureas including glibenclamide bind to some extent also to SUR2A and SUR2B (Table 3). 71
Compounds directly affecting KATP-channel.

a KATP-channel openers in green and KATP-channel blockers (sulfonylureas) in red. 70
Whether glibenclamide is suitable for acute migraine treatment would be the next question to address in this context. The SUR2B subunit is highly expressed in migraine-related structure, including cranial arteries, trigeminal ganglion, and trigeminal nucleus caudalis. 28,71 –73 Although glibenclamide is not a specific blocker for SUR2B, further studies investigating the effect of glibenclamide alone and in combination with levcromakalim will elucidate the role of KATP channel on human cerebral hemodynamics and on headache/migraine (Figure 2).

Levcromakalim opens KATP channels and potassium diffuses extracellular causing hyperpolarization and vasodilation. In vitro and in vivo glibenclamide blocks KATP channels and inhibit levcromakalim-induced vasodilation. KATP: adenosine triphosphate-sensitive potassium
Key findings
Glibenclamide inhibited levcromakalim- and other KCOs-induced vasodilation. Glibenclamide does not alter the basal vascular tone. Glibenclamide might be a suitable tool to further investigate the role of KATP channels in headache and migraine.
Footnotes
Acknowledgments
The authors thank Lundbeck Foundation for their support.
Declaration of conflicting interests
MA reports personal fees from Allergan, Amgen, Alder, Eli Lilly, Novartis, and Teva. He has no ownership interest and does not own stocks of any pharmaceutical company. He serves as an associated editor of Cephalalgia, co-editor of the Journal of Headache and Pain. MA is the President of the International Headache Society and General Secretary of the European Headache Federation. MMK has acted as an invited speaker for Novartis and received travel grant from ElectroCore. MS and AG declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Lundbeck Foundation (R155-2014-171).