
Abstract
Aim: To explore a possible relationship between vasodilatation and delayed headache we examined the effect of pituitary adenylate cyclase-activating polypeptide-38 (PACAP38) on the middle meningeal artery (MMA) and middle cerebral artery (MCA) using high resolution magnetic resonance angiography (MRA).
Methods: In a double-blind, randomized, placebo-controlled study 14 healthy volunteers were scanned repeatedly after infusion (20 min) of 10 pmol/kg/min PACAP38 or placebo. In addition, four participants were scanned following subcutaneous sumatriptan (6 mg).
Results: We found significant dilatation of the MMA (p = 0.00001), but not of the MCA (p = 0.50) after PACAP38. There was no change after placebo (p > 0.40). Vasodilatation (range 16–23%) lasted more than 5 h. Sumatriptan selectively contracted the MMA by 12.3% (p = 0.043).
Conclusion: PACAP38-induced headache is associated with prolonged dilatation of the MMA but not of the MCA. Sumatriptan relieves headache in parallel with contraction of the MMA but not of the MCA.
Introduction
Pituitary adenylate cyclase activating polypeptide (PACAP) is a relatively newly discovered neuropeptide belonging to the secretin/glucagon super family (1). PACAP exists in two forms, PACAP27 (2) or the C-terminally extended form, PACAP38, which is the most prominent form in the CNS (1). PACAP is involved in various biological processes, including sensory processing, vasodilatation and inflammation (3). PACAP receptors are found in human cerebral arteries and sensory, sympathetic and parasympathetic ganglia (4). In addition, PACAP38 may have a neuroprotective role as reported in animal stroke models (5), and therefore it has been of interest to study cerebral pharmacodynamics in vivo in humans (6).
Intravenous infusion of PACAP38 triggers immediate and delayed headache in healthy volunteers and delayed migraine-like attacks in migraine patients without aura (6,7). Furthermore, PACAP38 induces prolonged dilatation of the superficial temporal artery (STA) (7). The contribution of immediate and sustained arterial dilatation to PACAP38-induced delayed headache and migraine responses is unknown. Moreover, the long duration of PACAP38-induced vasodilatation has previously not been sufficiently examined. Recently, a magnetic resonance angiography (MRA) study has shown that dilatation of the middle meningeal artery (MMA) may be involved in the generation of immediate headache in healthy participants by calcitonin gene-related peptide (CGRP) (8). Vasodilatation was also present during CGRP-induced migraine attacks (9). The effect of PACAP on MMA tone, the principal artery supplying the dura mater, has not previously been studied.
We here examine the effect of PACAP38 infusion on the MMA and the MCA circumference over several hours using a high resolution MRA technique in a randomized, double-blind placebo-controlled design in healthy volunteers. We hypothesized that PACAP38-induced headache is associated with prolonged dilatation of both MMA and MCA.
Materials and methods
Participants
We recruited 15 healthy volunteers (8 female and 7 male; mean age 25 years (range 20–28) and mean weight 73 kg (range 54–95 kg)). Exclusion criteria were: a history of serious somatic disease; migraine or any other type of headache (except episodic tension-type headache less than once a month); daily intake of any medication except contraceptives; and contraindications for MRI scan. All female participants used safe contraceptive methods. All participants gave informed consent to participate. The Ethical Committee of Copenhagen approved the study (H-1-2008-108), which was conducted in accordance with the Helsinki II Declaration of 1964, as revised in Edinburgh in 2000.
Design and randomization
15 participants were randomly allocated in a 2:1 order to receive 10 pmol/kg/min PACAP38 (n = 10) (Calbiochem®, Darmstadt, Germany) or placebo (n = 5) (isotonic saline) for 20 min. The chosen PACAP38 dose has previously been shown to induce headache and haemodynamic changes in the brain in healthy volunteers and migraine without aura patients (6,7). The reason for selecting an unequal allocation was that we expected no placebo response on the vessels. Furthermore, a small placebo group would be sufficient to blind the researcher.
Participants who reported a delayed headache of intensity ≥ 2 on a verbal rating scale (VRS) from 0 to 10 received a subcutaneous injection of sumatriptan 6 mg (Imigran® injection, Glaxo Wellcome Operations, Barnard Castle, UK). The data analysis was performed blindly with respect to both the experimental drug and the time sequence of the MRA images.
Experimental procedures
All participants reported to the laboratory headache free. Coffee, tea, cocoa or other methylxanthine-containing foods or beverages, and tobacco were not allowed for at least 12 h before start of the study. Participants were placed in the supine position in the MR scanner room and a venous catheter (Venflon, Becton Dickinson Infusion Therapy AB, Sweden) was inserted into the left antecubital vein for infusion. We collected blood samples to determine the baseline haematocrit. The participants were monitored with ECG (by ECG monitoring function attached to the MR scanner), end-tidal partial pressure of CO2 (PetCO2) (capnograph, Datex, Finland), mean arterial blood pressure (MAP) and heart rate (HR) (Veris monitor, Medrad, USA).
MR imaging was performed on a 3.0 Tesla Philips Achieva Scanner (Philips Medical Systems, Best, The Netherlands) using an eight-element phased-array receiver head coil. We obtained repeated MRA measurements covering the MMA and MCA before and after PACAP38/placebo infusion (Figure 1). All other variables were recorded at fixed time points (baseline, every 10 min in the period 0–40 min, at 70, 90, 110, 140 min, and every 30 min in the period 3–5 h) throughout the study (Figure 1). Based on previous data (6) we defined immediate (0–119 min) and delayed (2 to 5 h) phases. Headache intensity was recorded on a verbal rating scale (VRS) from 0 to 10 (0, no headache; 1, a feeling of pressure; 10, worst imaginable headache). We expected that PACAP38 would induce minimum of 1 on the VRS in all participants during the immediate and delayed phases (2 to 5 h). Participants who reported 2 or higher on the VRS were treated with the migraine-specific abortive drug sumatriptan (a 5-HT1B/D agonist) and they underwent additional scans to investigate the effect of sumatriptan on arteries (Figure 1).
Ten healthy participants were randomly allocated to receive infusion of PACAP38 and five participants to receive placebo over 20 min. Magnetic resonance angiography (MRA) was performed at baseline and 20 min and 110 min after infusion. Then, the participants were divided into two groups (Group A: VRS < 2 and Group B: VRS ≥ 2). Group A participants were scanned at fixed time points at 2.3 h and 4.8 h. Group B participants, who reported pain intensity ≥ 2 on the VRS in the delayed phase (2–5 h), were scanned before and 20 min after treatment with sumatriptan (suma). One participant withdrew after baseline scan because of discomfort. Data from one participant at 110 min was missing as a result of technical error.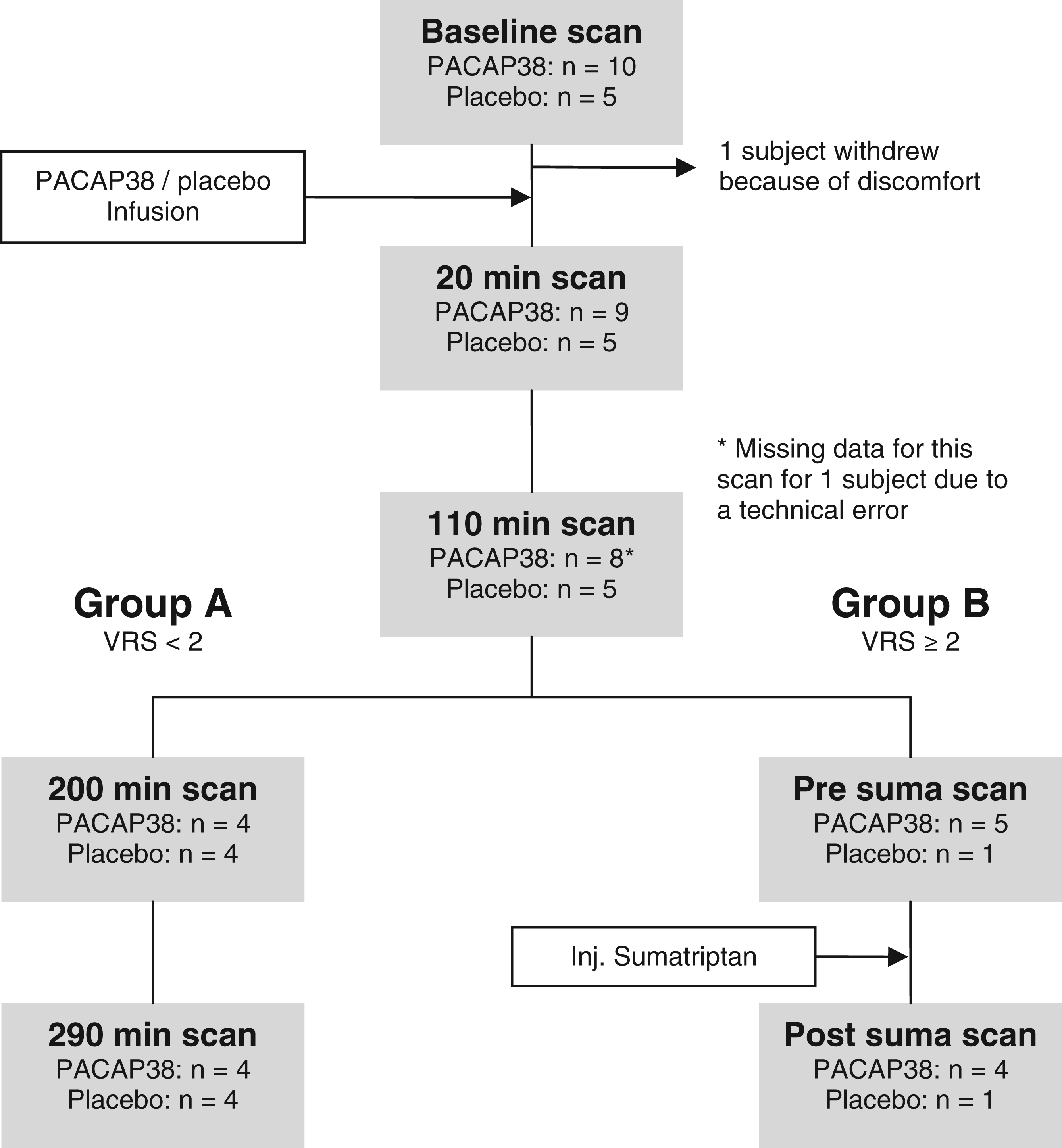
If the participants fulfilled IHS criteria C, D and E for migraine without aura (10), they were characterized as having migraine-like attacks.
Data acquisition and imaging protocols
For vessel imaging, a 3D inflow gradient echo sequence was used. First, a scout MR-angiography (MRA) was performed using field-of-view (FOV) 180 × 180 × 120 mm3; acquired matrix size (MxP) of 120 × 120, acquired voxel resolution 1.5 × 1.5 × 2.4 mm3, reconstructed resolution 0.70 × 0.70 × 1.20 mm3, repetition time (TR) 23 ms; echo time (TE) 5.4 ms; flip angle 20°; SENSE factor 2; two chunks; total scan duration of 73 s. The scout MRA was used to plan the subsequent MCA scans. The MRA of MCA used: FOV 200 × 200 × 74 mm3; MxP 800 × 406, acquired voxel resolution 0.25 × 0.49 × 1.00 mm3; reconstructed resolution 0.20 × 0.20 × 0.50 mm3; TR 25 ms; TE 3.5 ms; flip angle 20°; SENSE factor 2; four chunks; total scan time of 9 min 03 s. The first acquired angiography (baseline) had a large vertical FOV to ensure that the MCA was imaged, and was used to place the subsequent angiography of MMA. MMA scans had FOV 200 × 200 × 16 mm3; MxP 800 × 571; acquired voxel resolution of 0.25 × 0.35 × 0.70 mm3; reconstructed resolution 0.20 × 0.20 × 0.35 mm3; TR 25 ms; TE 3.5 ms; flip angle 20°; SENSE factor 2; two chunks; total scan duration of 5 min 29 s. When the participant was not removed from the MR scanner between two angiographies (between baseline (T0) and 20 min (T20), and between before and after sumatriptan), we used a MCA scan with shorter FOV 200 × 200 × 37 with total scan duration time 4 min 31 s.
Data analysis and statistics
Angiography
The angiography data were transferred to a remote workstation in Dicom format and then analysed by the LKEB-MRA Vessel wall analysis software (11). The software provides automated contour detection and quantification of the luminal boundaries in vessel segments. The MMA was identified by marking the branch from the main trunk of the maxillary artery and the MCA by marking the branch from the main trunk of the internal carotid artery. In each scan, a vessel segment with the exact same starting and ending point was identified on each side. The software automatically calculated a path line and measured the circumference of the vessel every 0.2 mm perpendicular to the centre line, from which the average circumference for each vessel was finally obtained.
Statistics
All absolute values are presented as mean ± standard error of mean (SEM), except headache scores, which are presented as median. Percent changes were reported as mean and 95% confidence interval (CI).
The primary endpoints were changes in the MMA and the MCA circumferences after infusion of PACAP38 and placebo over time. The secondary endpoints were (I) difference in area under the curve (AUC0–110 min) for the MMA and the MCA circumference between PACAP38 and placebo; (II) difference in the MMA and the MCA circumference before and after sumatriptan injection; (III) differences in AUCMAP, AUCHR and AUCPetCO2 between PACAP38 and placebo.
We analysed for changes over time with a two-way univariate analysis of variance (ANOVA) with participants and time as fixed factor. To reduce mass significance the following time points were selected for analysis (T0, T20 and T110). If overall differences were found, Dunnett’s test was applied to characterize which time points were different from baseline (p < 0.05). We calculated AUC according to the trapezium rule (12) to obtain a summary measure and to analyse the differences in response between PACAP38 and placebo. Baseline corrected values was used. Baseline differences and AUC values for the MMA and MCA circumference between PACAP38 and placebo were compared using independent samples t-test. Analysis of side-to-side differences, before and after sumatriptan, and AUC values for vital signs were performed with a paired two-way t-test. The level of significance was set at p < 0.05 for all analyses. All analysis was done using SPSS for Windows 17.0 (Chicago, Illinois, USA).
Results
Baseline values (± SEM) in 14 healthy participants
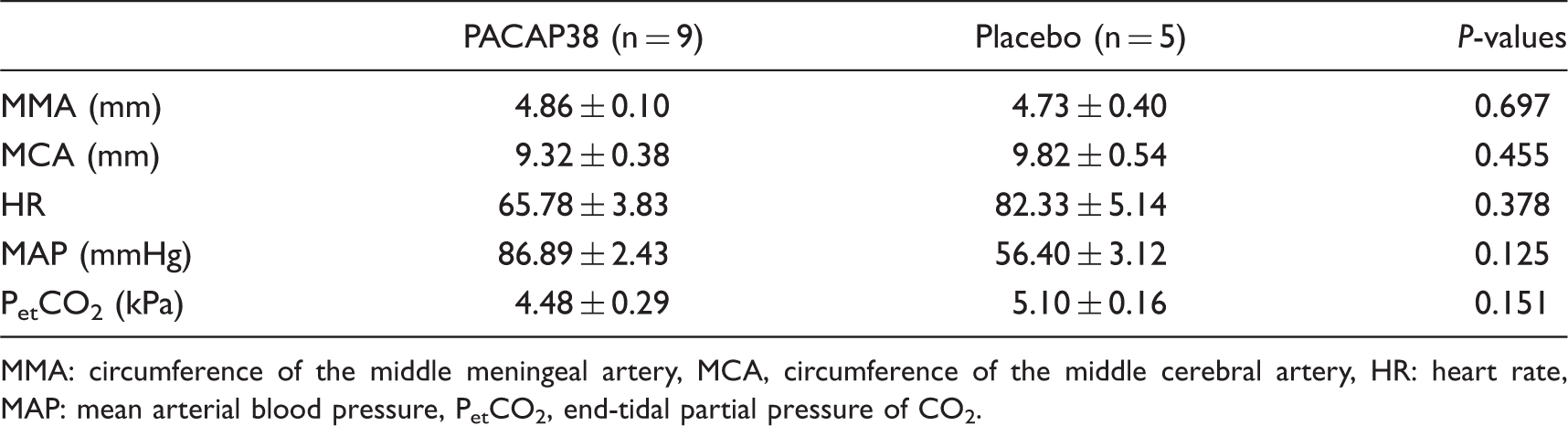
MMA: circumference of the middle meningeal artery, MCA, circumference of the middle cerebral artery, HR: heart rate, MAP: mean arterial blood pressure, PetCO2, end-tidal partial pressure of CO2.
Headache characteristics after PACAP38 in healthy volunteers

a: initial phase (0–119 min); b: delayed phase (2–5 h). *Headache characteristics: localisation/peak intensity/quality (throb: throbbing; pres: pressing)/aggravation by movement. †Associated symptoms: nausea/photophobia/phonophobia.
Effect of PACAP38 on MMA and MCA during immediate phase
ANOVA showed significant changes in MMA circumference after infusion of PACAP38 over time (p < 0.00004) but not after placebo (p = 0.27). Post hoc analysis revealed significant dilatation of the MMA at 20 min: 5.97 mm± 0.14 (p = 0.0003) and at 110 min: 5.76 mm± 0.10 (p = 0.001), after start of PACAP38 infusion compared with baseline: 4.85 mm± 0.11. We found no difference in MMA circumference at 20 min: 4.77 mm± 0.38 (p = 0.805) or at 110 min: 4.99 mm± 0.31 (p = 0.130) after placebo compared with baseline: 4.73 ± 0.40. Mean percent dilatation and CI are shown in Figure 2. The AUC0–110 min for MMA was significantly larger after PACAP38: 102.3 ± 13.8, compared with placebo: 13.8 ± 11.2 (p = 0.001) (Figure 2).
Percentage changes from baseline in mean circumference of middle meningeal artery (MMA) in the immediate phase. MMA dilated by 23.4% (14.0% to 32.8% CI) at 20 min and by 19.3% (10.1% to 28.6% CI) at 110 min at PACAP38 (n = 8) infusion. There was no statistical change after placebo (n = 5) infusion. Error bars represent 95% confidence intervals.
ANOVA showed no statistical changes in MCA circumference after infusion of PACAP38 over time (p = 0.39) or after placebo (p = 0.60). Post hoc analysis showed no changes of the MCA at 20 min: 9.27 mm± 0.43 (p = 6.02) or at 110 min: 9.13 mm± 0.41 (p = 0.458) after infusion start compared with baseline: 9.34 mm± 0.43. Placebo infusion showed no MCA changes either at 20 min: 9.93 mm± 0.47 (p = 0.650) or at 110 min: 9.69 mm± 0.35 (p = 0.641) compared with baseline: 9.82 mm± 0.54. Mean percentage changes and CI are shown in Figure 3. The AUC0–110 min for the MCA showed no difference between PACAP38: –17.4 ± 16.2, and placebo: 0.33 ± 23.9, p = 0.536 (Figure 3).
Percentage changes from baseline in mean circumference of middle cerebral artery (MCA) in the immediate phase. There was no statistical change after PACAP38 (n = 8) or placebo (n = 5) infusion. The error bars show 95% CI.
MMA and MCA circumference before and after sumatriptan
Five participants (56%) reported headache intensity ≥ 2 (range 2 to 6 on VRS) during the delayed phase. Four participants were scanned before and after injection of sumatriptan 6 mg subcutaneously, as one participant declined the administration of sumatriptan.
MMA circumference was significantly reduced 20 min after sumatriptan: 5.21 mm± 0.08 compared with the pre-treatment scan: 5.79 mm± 0.23 (p = 0.045). MCA remained unchanged 20 min after sumatriptan: 9.31 mm± 0.63 compared with the pre-treatment recording: 9.19 mm± 0.50 (p = 0.78) (Figure 4). All participants reported pain free at 50 min (mean time) after sumatriptan.
Percentage changes in the MMA and the MCA circumference between before and after injection of 6 mg sumatriptan in four healthy participants. The MMA changed by 23.8% (13.4% to 34.2%) before sumatriptan compared with baseline. The dilatation was reduced to 11.5% (2.8% to 20.8%) 20 min after sumatriptan administration. There was no change in the MCA circumference between before and after treatment with sumatriptan (p = 0.67). Individual and median (thick lines) headache intensity after PACAP38 (A) and after placebo (B) infusion. Participants who reported VRS ≥ 2 and received sumatriptan (Group A on Figure 1) are not shown in this figure.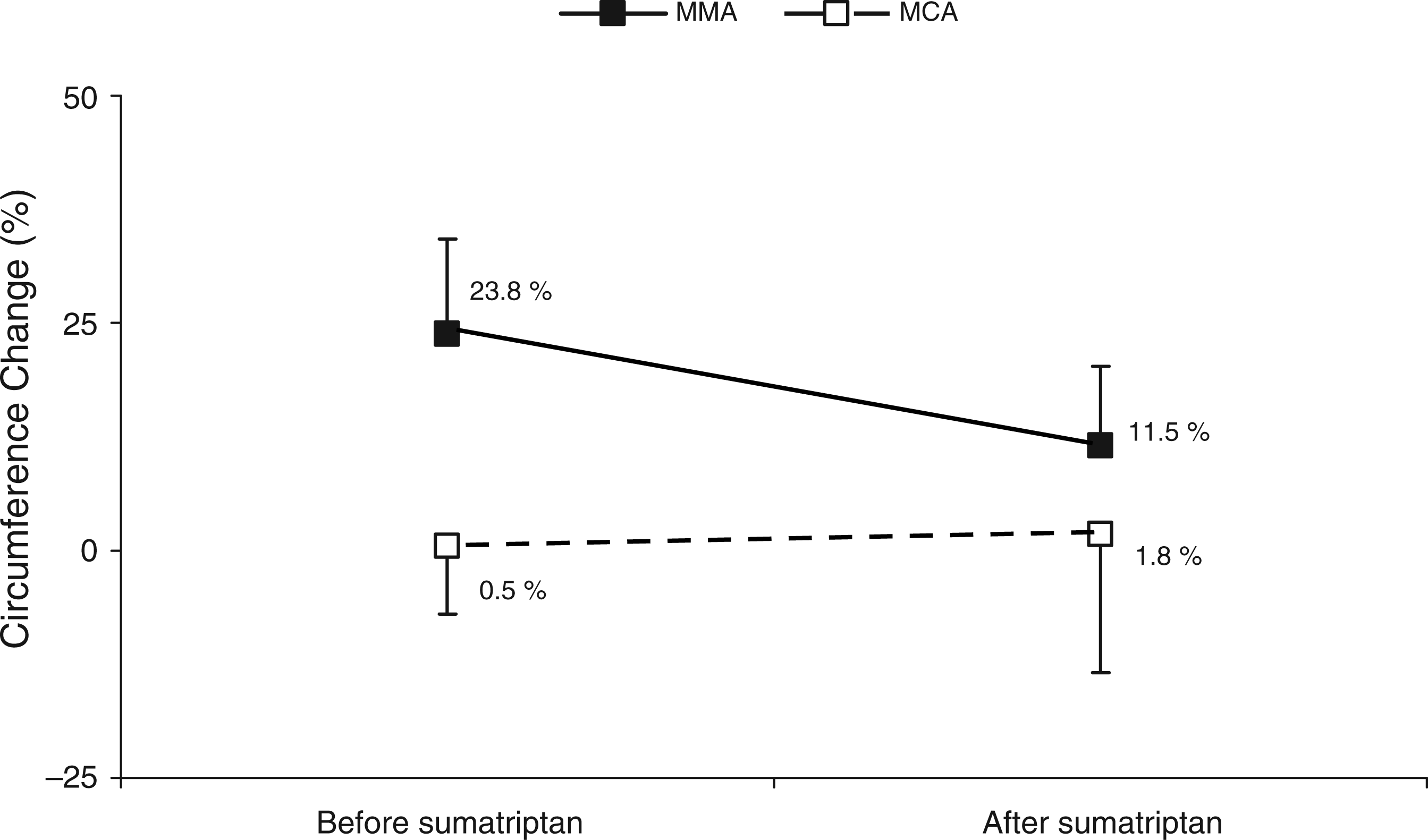

Effect of PACAP38 on heart rate, MAP and end-tidal CO2
Adverse events after PACAP38 and placebo infusion

There was no difference in AUCMAP, AUCHR and AUCPetCO2 between PACAP38 and placebo (p > 0.05) during the delayed phase (2–5 h) (Table 3).
Discussion
This is the first in vivo study of long-term haemodynamic effects of PACAP38 on extra- and intracerebral arteries during head pain using high resolution MRA. We assessed the circumference changes of the MMA and the MCA with time fixed repeated scan sessions for almost 5 h after start of infusion of PACAP38. The major findings were that PACAP38 caused a marked and long-lasting dilatation of the MMA associated with headache, whereas MCA circumference remained unchanged. In addition, subcutaneous injection of sumatriptan 6 mg reversed the MMA dilatation and the delayed headache without any effect on the MCA.
Effect of PACAP38 on extra and intracerebral arteries in humans
PACAP38 dilates human cerebral arteries (6,7) and acts as a neuromodulator (3). Birk and colleagues systematically examined cerebral haemodynamics in response to PACAP38 infusion in healthy volunteers (6). The authors reported headache and a dilatation of the MCA immediately after PACAP38 infusion. This important finding was followed by an investigation of PACAP38 in migraine patients (7). Schytz et al. found a short-lasting dilatation (8.5%) of the MCA, and a marked (37%) and prolonged (90 min) dilatation of the superficial temporal artery (STA) (7). In addition, PACAP38 caused a delayed headache and migraine-like attacks in patients and controls (6,7). However, a possible relationship between head pain and vasodilatation after PACAP38 remains unclear. The above mentioned studies used transcranial Doppler (TCD) combined with single photon emission computed tomography (SPECT) that have a few major limitations. First, the measurement of the MCA diameter was calculated from blood velocity in the MCA and cerebral blood flow and hence indirect. Secondly, the SPECT method is influenced by extracranial flow due to scattered radiation (Compton scatter). Finally, TCD cannot be used to explore a possible role of meningeal blood vessels (e.g. the MMA). The latter is very important as MMA is the principal artery supplying the dura mater, which is a pain-sensitive intracranial structure, suggested as a primary site of nociception in migraine pain (13–15). However, MRA is a direct way to measure diameter of arteries and superior to above mentioned methods.
PACAP38 induced vasodilatation and headache
In the present study we applied MRA to examine the MMA and the MCA directly with regard to the arterial circumference. We found PACAP38 to induce a marked and sustained dilatation of the MMA up to 23% and co-occurring with headache, whereas the MCA diameter remained unchanged. However, the most interesting observation was that dilatation of the MMA lasted more than 5 h, was associated with delayed headache and was reversed after administration of sumatriptan.
PACAP38 has to cross the blood brain barrier (BBB) to reach its receptors in the smooth muscle cells in the MCA (4,16,26). The transport of PACAP38 across the BBB is dependent on a saturable carrier mediated transport system (16). Only a very small percentage (0.053%) PACAP38 does, however, cross the BBB in mice in the 5 min period after intravenous administration (16). Birk et al. (6) reported no major direct effect on rCBF after PACAP38 infusion in healthy volunteers after CBF was corrected for hyperventilation. This suggests that a lack of vasodilatation of the MCA after PACAP38 could be explained partly by its inability to cross the BBB in humans.
PACAP38 exerts its effect via the VPAC1, VPAC2 and PAC1 receptors (17,18). VPAC1 is considered to be the main receptor responsible for the vasodilatation (19,20), whereas VPAC2 is primarily responsible for mast cell degranulation as VPAC1 is not expressed on human mast cells (21). Interestingly, PACAP38 and vasoactive intestinal polypeptide (VIP) belong to the same secretin/glucagon family and both share their effect on VPAC1 and VPAC2 receptors (1,2). In a study of cutaneous pain in humans, PACAP38 and VIP showed similar responses with regard to short-lasting vasodilatation and neurogenic inflammation in skin (22). However, provocation studies using intravenous infusion revealed differences between PACAP38 and VIP. Although both peptides have a short half life (PACAP38: 3.5 min (7); VIP: 1.0 min (23)) and plasma concentration of both returned to baseline 2 h after start of infusion we observed differences in vascular and headache responses. Thus, dilatation of the superficial temporal artery was relatively short-lasting after VIP (24) and sustained after PACAP38 throughout the observation period of 90 min (7). Moreover, VIP failed to induce migraine attacks (25), whereas PACAP38-induced delayed migraine-like attacks (7). These data suggest that long-lasting vasodilatation and delayed migraine after PACAP38 are unlikely to be due to an effect on VPAC1 and VPAC2 receptors. However, PACAP38, in contrast to VIP, also acts on the PAC1 receptor. Therefore, it is possible that the present data of marked and sustained effect of PACAP38 on the MMA and delayed headaches is due its selective effect on the PAC1 receptor. The present findings could also indicate that the delayed headache and migraine-like attacks might be due to a sustained dilatation of extracerebral arteries.
Another interesting observation in the present study is that anti-migraine drug sumatriptan reversed PACAP38-induced dilatation of the MMA and headache. We did not observe any effect of sumatriptan on the MCA. The same pattern was reported after CGRP administration in healthy volunteers (8). Taken together these findings suggest that head pain may arise from the extracerebral arteries and that contraction of the MMA, but not the MCA, has a role in headache relief after sumatriptan.
Footnotes
Acknowledgements
The authors thank all participating healthy volunteers. The authors would also like to thank Michael Baun, Danish Headache Centre, Research Park, Glostrup, for his advice concerning PACAP38 and radiographers Majut Lindhart, Bente Sonne Møller and Helle Simonsen for their assistance during the experiments.