
Abstract
We describe a patient affected by migraine with visual and somatosensory aura, whose symptoms were consistently attenuated by noninvasive peripheral vagal nerve stimulation (nVNS) in multiple prospectively recorded attacks. When compared with the current standard of care, nVNS significantly reduced the duration of visual aura in all the attacks (n = 5) and prevented the somatosensory aura in three of the five attacks. The overall duration of nVNS-treated auras was 19.0 ± 4.2 min, significantly shorter than the duration of aura in attacks treated with standard of care (103.8 ± 10.3 min). This single-case study requires confirmation in a larger sample size, but we believe that this first report is suggestive of likely efficacy given the relatively high number of treated attacks and the consistent effect of nVNS.
Keywords
Introduction
A number of noninvasive neuromodulation techniques have shown efficacy in the acute treatment of migraine 1 through a number of different pathophysiological mechanisms. Ayata and colleagues recently reported that noninvasive vagal nerve stimulation (nVNS) significantly reduces the susceptibility to cortical spreading depression. 2 Cortical spreading depression is considered the electrophysiological event underlying migraine aura, 3 suggesting a clinical role for nVNS to treat aura symptoms as well as the treatment of headache pain.
Here, in this report, we describe a case study of a patient whose aura was repeatedly and consistently shortened by nVNS.
Case report
The subject is a 38-year-old female patient affected by migraine with (MA) and without aura according to the International Classification of Headache Disorders 3rd edition criteria. She has been followed up as an outpatient at the Headache Science Centre of the IRCCS Mondino Foundation (Pavia, Italy) since 2015. Migraine without aura presented more frequently, occurring on 7–8 days per month, while the frequency of MA attacks was 5–6 episodes per year.
Her usual aura consisted of a monolateral negative scotoma with gradual onset, progressively evolving in homonymous hemianopia (either left or right), constantly followed by unilateral paresthesias with a progressive ascending involvement from the hand to the hemiface. The full aura duration was 2 h, with visual and paresthetic aura each lasting 60 min. In some cases, the two types of aura presented with a partial overlap with the visual aura fading, while the paresthetic aura began to spread. The full aura has always been followed almost immediately by severe unilateral migraine (either left or right) associated with nausea, frequent vomiting, photophobia, and phonophobia. The migraine pain responded in 60 min to eletriptan 40 mg, but in 80% of the attacks the pain returned after 4–5 h. The patient was on a stable dose of cinnarizine (25 mg daily) for migraine prevention. She was also on combined oral contraception since 2013, without any worsening effect on migraine. Neurological examination was normal. Brain MRI and intracranial arteriosus ANGIO-MRI showed a para-physiological variation of the anterior communicating artery devoid of clinical relevance. Her medical history was unremarkable with the exception of a mild asymptomatic iron-deficient anemia.
In 2016, she was enrolled in the PRESTO study, 4 a randomized sham-controlled trial on the efficacy of nVNS delivered with the gammaCore® device (electroCore, Inc., Basking Ridge, New Jersey, USA) in the acute treatment of migraine attacks. During the open-label phase, she had the chance to treat attacks of MA with active nVNS, reporting a positive effect on the overall duration of her aura symptoms.
At the end of the clinical trial, we provided her with active nVNS asking her to treat the subsequent MA attacks alternatively with nVNS or standard of care (SoC). To best evaluate the effect of nVNS on aura symptoms, the patient was trained to deliver a 120-s stimulation per side of the neck at the moment of aura onset, regardless of the location of the visual/paresthetic symptoms. At her discretion, the stimulation could be repeated after 15-min, according to the paradigm that was adopted during the pivotal trial.
For SoC, the patient was free to use her usual symptomatic drug (eletriptan 40 mg) whenever she felt it necessary.
The features of aura and pain were reported in her personal headache diary. The following outcomes were recorded: duration of visual aura, involvement of the visual field (quarter, half, or whole visual field), duration of somatosensory aura, extension of somatosensory aura (hand, arm, and hemiface), possible adverse events, and presence or absence of the pain phase. If this latter manifested, the patient was instructed to record pain intensity (mild, moderate, or severe) and associated symptoms (nausea, photophobia, and phonophobia).
The patient signed a written informed consent for data collection and use and gave verbal consent for information about herself to be published.
Results
During the observation period (from July 2016 to September 2018), the patient reported nine MA attacks; five were treated with nVNS, while the other four were managed with SoC.
The patient recorded a consistent effect of nVNS on both aura symptoms and pain. The duration of the visual symptoms was significantly shortened by nVNS when compared to SoC (17.0 ± 4.5 vs. 53.5 ± 4.8 min, respectively; Mann–Whitney U test: p = 0.001). After nVNS, the visual aura was limited to a quarter of the visual field in all cases, while it spread to half of the visual field after SoC. Additionally, the somatosensory aura was completely prevented in three of the five attacks treated with nVNS and lasted only 5 min in the remaining two. For all nVNS-treated attacks, somatosensory symptoms never involved the hemiface, being limited to the hand and the arm. The somatosensory aura was present in all the four attacks treated with SoC with a mean duration of 50.0 ± 9.1 min.
The overall duration of the aura phase was 19.0 ± 4.2 min after nVNS, significantly shorter than the 103.8 ± 10.3 min with SoC (Mann–Whitney U test: p = 0.001; Figure 1).

Comparison of duration of aura symptoms after nVNS and SoC: single attacks and averaged results. nVNS: noninvasive vagal nerve stimulation; SoC: standard of care; MA: migraine with aura.
In two of the five attacks treated with nVNS, the aura was not followed by headache pain or associated symptoms, while it started at the end of the aura in the remaining three attacks (mild-to-moderate intensity, associated with photophobia and phonophobia). Headache was always reported in all four attacks treated with SoC (severe intensity, associated with nausea, photophobia, and phonophobia). Whenever headache was present, the patient successfully treated it with eletriptan 40 mg, regardless of its intensity or prior use of nVNS.
No adverse events were reported for nVNS or SoC.
Aura and headache features of the recorded attacks are summarized in Table 1.
Aura and headache features of the MA attacks treated with nVNS or SoC.
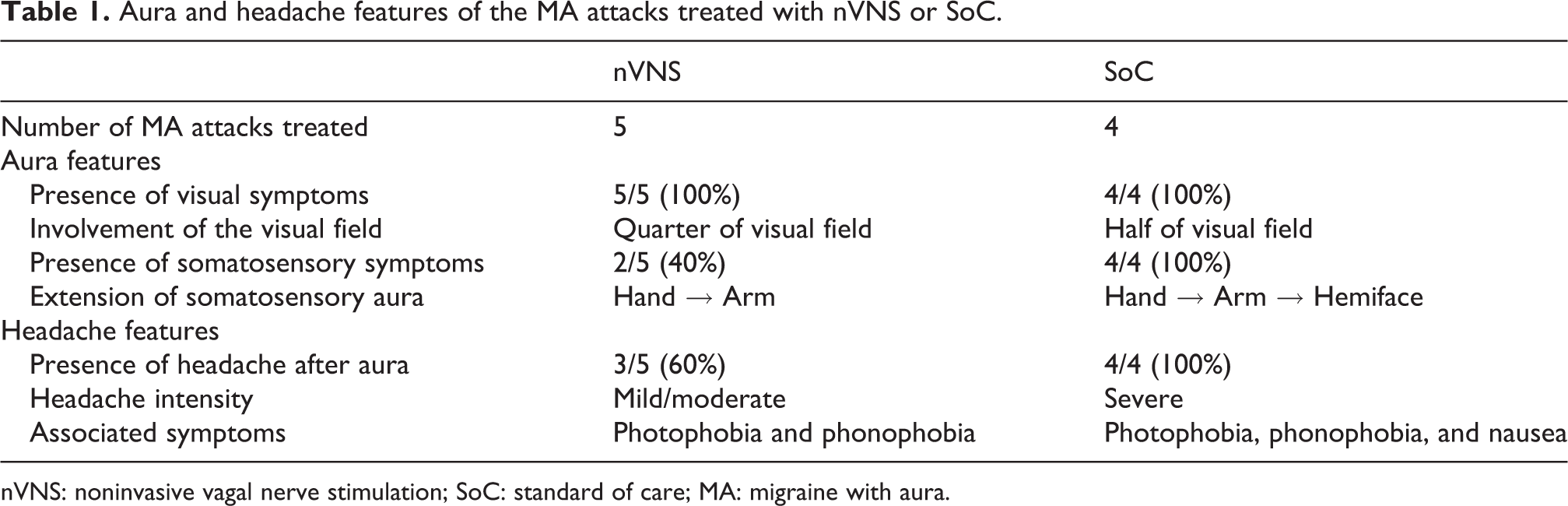
nVNS: noninvasive vagal nerve stimulation; SoC: standard of care; MA: migraine with aura.
Discussion
Preclinical data show that nVNS affects multiple areas involved in pain transmission and in migraine pathophysiology, such as nucleus tractus solitarius, trigeminal nucleus caudalis, spinal trigeminal nucleus, dorsal raphe nuclei, hypothalamus, locus coeruleus, and periaqueductal grey. 5,6 Furthermore, nVNS is able to modulate the susceptibility to cortical spreading depression. 2
The clinical utility of nVNS has been already demonstrated for the acute treatment of migraine 4,7 as well as the acute and preventive treatment of cluster. 8,9 To the best of our knowledge, this is the first documented report suggesting the effectiveness of nVNS on aura symptoms. Although based on a single patient, our observation is intriguing for several reasons: (i) the assessment was prospectively designed and included multiple attacks treated with nVNS and SoC; (ii) there are currently no approved or effective symptomatic treatments for the management of aura symptoms; and iii) nVNS is an FDA-approved and CE-marked device for acute migraine treatment, portable, easy to use, and with a favorable benefit/risk ratio.
The present data provide a strong rationale for assessing the potential effects of nVNS in the acute treatment of MA in a more comprehensive way, ideally in a randomized and sham-controlled trial.
Clinical implications
No effective first-line acute treatments are available for the managemet of aura symptoms. Noninvasive vagal nerve stimulation consistently shortened aura duration. Vagal nerve stimulation is a noninvasive approach with a favorable benefit/risk ratio.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CT received fees for participation in advisory board for Allergan S.p.A.; electroCore, Inc.; Teva; Eli Lilly; and Novartis. EL is an employee of electroCore, Inc., and receives stock ownership.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.