
Abstract
The combination of Aidi injection (ADI) and epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) in treating non-small cell lung cancer (NSCLC) has been reported, but the effects of this therapy have not been systematically assessed. Randomized controlled trials (RCTs) published before June 2020 were searched from 6 databases. Two reviewers independently assessed the methodological quality of 8 RCTs involving 667 patients diagnosed with stage III-IV NSCLC. We found that ADI combined with EGFR-TKI increased the objective response rate (ORR) significantly (relative risk [RR]: 1.60; 95% confidence interval [CI]: 1.28-1.99, P < 0.0001). There was also improvement in the disease control rate (DCR) (RR: 1.25; 95% CI: 1.11-1.40, P = 0.0002) as compared with EGFR-TKI alone. This therapy also increased the percentage of CD3+ cells (weighted mean difference [WMD]: 9.86; 95% CI: 4.62-15.10), CD4+ cells (WMD: 6.10; 95% CI: 1.67-10.53), and the CD4+/CD8+ (WMD: 0.35; 95% CI: 0.28-0.43). With regard to drug toxicity, the occurrence of rash was significantly reduced by ADI combined with EGFR-TKI (RR: 0.78, 95% CI: 0.63-0.97, P = 0.03); however, we did not find a significant reduction in the occurrence of dry skin, nausea and vomiting, as well as diarrhea between the 2 therapies. ADI combined with first-generation EGFR-TKIs may be more effective in improving tumor response, reducing the occurrence of rash, and enhancing immune function in NSCLC than EGFR-TKI alone.
Introduction
Lung cancer is the most lethal cancer with approximately 142,670 mortalities in the United States in 2019. 1 In China in 2013, it was estimated that there were more than 700,000 new lung cancer patients. 2 The percentage of non-small cell lung cancer (NSCLC) among all lung cancer cases is 80%, 3 and the current 5-year survival rate is only 4% in distant NSCLC. 4
To date, the most common oncogenic driver of NSCLC is epidermal growth factor receptor (EGFR) mutation. 5 Research has shown that EGFR-mutated lung adenocarcinoma accounts for about 10%-15% and 50% of cases, respectively, among Caucasian and Asian patients. 6 If advanced NSCLC patients have EGFR mutation, then there is strong evidence to suggest the use of EGFR tyrosine kinase inhibitors (TKIs). Chemotherapy with platinum could be a second choice. 7 -10 Thus, in advanced NSCLC patients with EGFR mutations, TKI therapy has become the standard first-line treatment. In addition, EGFR-TKIs can significantly benefit unselected Asian patients with advanced recurrent NSCLC, as adverse reactions are well tolerated and the overall efficacy is commensurate with the standard second-line chemotherapy. 11 -15 Therefore, patients could use EGFR-TKIs in the second-and third-line.
Despite rapid developments in molecular biology, first-generation EGFR-TKIs still occupy a dominant position in the treatment of NSCLC. 16 To date, first-generation EGFR-TKIs developed for NSCLC include erlotinib, gefitinib, and icotinib. In China, icotinib has proprietary intellectual property rights. 17 For NSCLC patients with EGFR mutation, first-generation EGFR-TKIs would be preferred over chemotherapy. 18 However, more than half of the patients gradually develop resistance after 9-14 months. 16 Despite technological advances, first-generation EGFR-TKIs also result in several side effects, including intestinal obstruction, hyponatremia, hypokalemia, and alopecia, 19 as well as diarrhea and rash, which are the most frequent adverse events. These factors may affect a patient’s survival, quality of life, and treatment outcome. At the same time, the LUX LUNG-7 study revealed that 3% of patients could not continue gefitinib therapy due to elevated liver enzyme levels. 20 Some patients were also unable to tolerate EGFR-TKI therapy owing to severe adverse reactions. Therefore, additional therapies are needed to reduce the risk of acquired resistance and alleviate the side effects of EGFR-TKIs.
Chinese medicine has been widely used in the treatment of lung cancer in China. 21 -24 Chinese medicine is associated with potential benefits, especially with regard to increasing the therapeutic effectiveness and alleviating the side effects of EGFR TKI. 25 -28 Aidi injection (ADI), which consists of extracts from Astragalus (Astragalus membranaceus), Eleutherococcus senticosus (Acanthopanax senticosus), ginseng (Panax ginseng C. A. Mey), and cantharidin (Lytta vesicatoria), is 1 such Chinese herbal preparation intended for intravenous use. 29 In the last several years, increasingly more clinical trials have reported that ADI adjuvant to chemotherapy could significantly improve treatment, raise immunity, and reduce the incidence of adverse drug reactions. 30 -33 Moreover, the number of published clinical studies on ADI and EGFR-TKI is increasing. 34 -41 However, these trials have a limited sample size, and the therapeutical outcome of ADI has not been assessed systematically. Therefore, we conducted this meta-analysis to explore the clinical outcome of ADI and EGFR-TKI therapy and evaluate its clinical value.
Methods
Data Collection and Strategies of Search
We searched the following databases up to June 2020: PubMed, Embase, Cochrane Library, Wanfang Database, Chinese Biomedical Literature Database, and Chinese National Knowledge Infrastructure. We used several terms as medical subject headings or free words: “non-small cell lung cancer,” “lung cancer,” “pulmonary cancer,” “lung carcinoma,” “pulmonary carcinoma,” “gefitinib,” “erlotinib,” “icotinib,” “EGFR-TKI,” “Aidi injection,” and “randomized controlled trials.” Two reviewers independently identified relevant clinical studies.
Inclusion Criteria
Clinical studies meeting the following criteria were included: (1) participants: NSCLC patients diagnosed histopathologically or cytologically and treated with EGFR-TKI; (2) type of study: RCTs with or without blinding; (3) type of intervention: a treatment group of ADI combined with EGFR-TKI and a control group of EGFR-TKI; and (4) type of outcome measurements: objective response rate (ORR), disease control rate (DCR), and performance status as the main outcome measures, with immune function and reduction in EGFR-TKI toxicity as the secondary outcome measures. The risk ratios and 95% confidence intervals (CIs) were also required to be calculated accurately.
Participant Exclusion Criteria
Studies meeting the following criteria were excluded: (1) studies enrolling patients with other malignancies; (2) studies including patients with a lung cancer type other than NSCLC; (3) other Chinese herbs were used; (4) duplicated studies; (5) studies without statistical data; and (6) studies with incomplete data.
Outcome Measures
Based on the World Health Organization scale, 42 ORR was obtained by adding the proportion of partial response to the proportion of complete response; DCR was defined as the sum of the proportions of complete response, partial response, and no change. The drug toxicity rate was the number of patients with any grade toxicity divided by the total number of patients.
Extraction of Data and Assessment of Quality
After searching the databases, 2 reviewers began to gather data. The reviewers assessed the methodological quality of 8 trials on the basis of the criteria of Systematic Reviews of Interventions 5.1.0. 43 The content assessed were (1) blinding of patients, study operators and outcome; (2) sequence generation; (3) incomplete final data of the study, such as how many patients drop out of the study; (4) allocation concealment. We also evaluated other biases using 3 categories: yes, no, and unclear. When disagreements occurred, we consulted a third reviewer.
Analysis of Data From the 8 Studies
We used Review Manager 5.3 software to perform the analysis. We used relative risk (RR) with a 95% CI to express dichotomous variables. If the study showed heterogeneity (I 2 > 50% and/or P < 0.10), the random model was appropriate; otherwise, we used the fixed model and Mantel-Haenszel method. P < 0.05 meant that the outcome was statistically significant. If more than 10 trials were enrolled, potential publication bias would be assessed and a funnel plot would be made.
Results
Description of Studies
A flow diagram describing the screening process is shown in Figure 1. After searching 6 databases, 174 trials were identified. After removing duplicates and screening the records, 13 studies were identified, of which 5 were excluded due to inappropriate interventions (n = 1), inappropriate tumor stage (n = 1), retrospective design (n = 1), and low quality (n = 2). Finally, 8 studies 34–41 involving 667 patients were included in this meta-analysis; 334 patients received ADI combined with EGFR-TKI and 333 received EGFR-TKI alone.

Flow diagram describing the screening process.
Characteristics of the 8 Studies
We paid attention to the first author, number of participants, tumor node metastasis (TNM) stage, line of treatment, EGFR mutation status, and treatment intervention. Eight clinical studies were found in Chinese journals, which had been performed in China from 2011 to 2020. The stages of lung cancer among the cases in the 8 studies were advanced. A single study mentioned second line treatment. Three of the 8 studies reported patients with EGFR mutation. Gefitinib was given 250 mg daily; icotinib, 375 mg once; and erlotinib, 150 mg daily. The dose of ADI was 50-100 mL per day. The treatments were administered for a duration of 1-3 months in the eligible studies.
Characteristics of the 8 Studies.

Abbreviations: n, number of participants; NA, not available.
* Line of treatment.
† EGFR: EGFR mutation status.
‡Protocol: treatment group intervention.
Methodological Bias
All studies mentioned randomization; 5 of the 8 trials described the randomization process. None of the trials discussed the concealment of treatment allocation or blinding procedures, which caused selection bias. One trial reported no dropouts. Generally, all RCTs had an unclear bias risk; at the same time, insufficient methodological quality existed. The assessment of the meta-analysis is illustrated in Figure 2.

Graph showing risk of bias in the enrolled randomized controlled trials.
Outcome Measures
Objective response rate
Seven studies that included a total of 493 patients reported an ORR (Figure 3). A fixed model (homogeneity, I 2 = 0%; P = 0.65) was chosen. Results showed that the ORR of ADI plus EGFR-TKI was significantly better than that of gefitinib (RR: 1.60; 95% CI: 1.28-1.99, P < 0.0001).
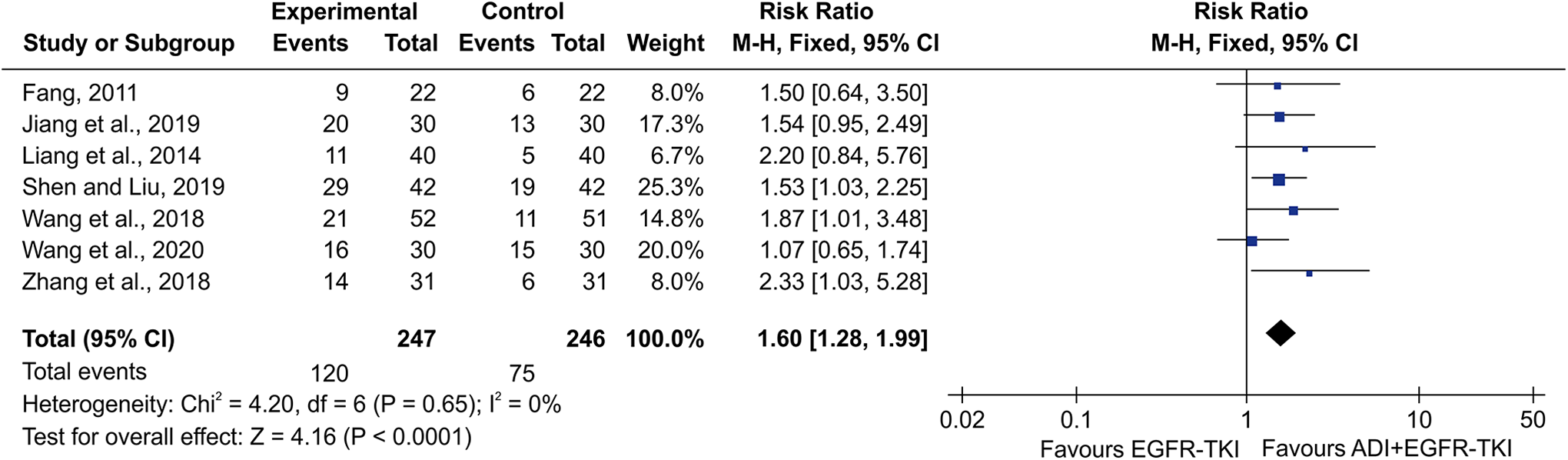
The effect of ADI plus EGFR-TKI on the ORR in NSCLC patients. CI, confidence interval; ADI, Aidi; M-H, Mantel-Haenszel.
Disease control rate
Six studies that included 409 patients evaluated DCR (Figure 4). The heterogeneity was not significant (I 2 = 28%, P = 0.23) between them. According to the fixed-effects model, ADI plus EGFR-TKI treatment could increase the DCR more than EGFR-TKI (RR: 1.25; 95% CI: 1.11-1.40, P = 0.0002).

The therapy of ADI plus EGFR-TKI on the DCR in NSCLC patients.
EGFR-TKI toxicity
Rashes were reported in 4 studies that included 246 patients in total. The analysis showed that ADI plus EGFR-TKI could significantly decrease the incidence of rash compared with EGFR-TKI alone (RR: 0.78; 95% CI: 0.63-0.97, P = 0.03) (Figure 5). We used a fixed-effects model as heterogeneity was not significant among the 4 trials (I 2 = 0%, P = 0.95).

The adverse reactions of Aidi plus EGFR-TKI in NSCLC patients. ADI, Aidi.
Dry skin was reported in 2 studies with 106 patients (Figure 5). With I 2 = 0% for the heterogeneity test, the fixed model was used. We found that ADI plus EGFR-TKI was not significantly different from EGFR-TKI alone (RR: 0.75; 95% CI: 0.28-2.01, P = 0.57) in causing skin dryness.
Four studies that included 246 patients reported nausea and vomiting. Because heterogeneity was not significant (I 2 = 0%, P = 0.80), we used the fixed model and found that ADI plus EGFR-TKI did not significantly reduce the occurrence of nausea and vomiting compared with EGFR-TKI (RR: 0.69; 95% CI: 0.33-1.42, P = 0.31) (Figure 5).
Two studies that included 184 patients reported diarrhea (Figure 5). There was no obvious heterogeneity (I 2 = 0%); therefore, we used the fixed model. ADI plus EGFR-TKI did not significantly reduce diarrhea compared with EGFR-TKI alone (RR: 0.78; 95% CI: 0.53-1.16, P = 0.22).
Immune function
Three trials calculated the proportion of CD3+, CD4+, and CD4+/CD8+ cells with 318 patients (Figure 6). The combined weighted mean difference (WMD) and 95% CI were calculated by a random model. The 2 groups showed significantly different results with regard to CD3+ (WMD: 9.86, 95% CI: 4.62-15.10, P = 0.0002), CD4+ (WMD: 6.10, 95% CI: 1.67-10.53, P = 0.007), and CD4+/CD8+ (WMD: 0.31, 95% CI: 0.10-0.52, P = 0.005), indicating that ADI combined with EGFR-TKI can enhance the immune function of patients with NSCLC.

Aidi plus EGFR-TKI on the levels of CD3+, CD4+, and CD4+/CD8+ cells. SD, standard deviation; ADI, Aidi; IV, inverse variance.
Discussion
This meta-analysis included 8 studies involving 667 patients. This is the first study to conduct a systematic review of ADI and first-generation EGFR-TKI.
Chinese medicine is beginning to play an important role in the reduction of toxicity and enhancement of efficacy in the treatment of lung cancer. In this study, ADI combined with EGFR-TKI prolonged ORR and DCR. Further, side effects were observed in patients receiving first-generation EGFR-TKI. In this meta-analysis, ADI combined with EGFR-TKI showed improved proportions of CD3+, CD4+, and CD4+/CD8+ cells in patients with NSCLC.
Apoptosis of tumor cells and inhibition of cell proliferation have been observed after ADI use. The main ingredients of ADI are Astragalus (Astragalus membranaceus), Eleutherococcus senticosus (Acanthopanax senticosus), ginseng (Panax ginseng C. A. Mey), and cantharidin (Lytta vesicatoria). Ginsenoside Rg3 (Rg3), a product of ginseng and an antiangiogenic agent, is effective in protecting lung adenocarcinoma cells from DNA damage while simultaneously inhibiting tumorigenesis, 44 thereby showing clinical benefits. 45 20(S)-Rg3 can reverse icotinib resistance through Rg3-induced autophagy inhibition. 46 Thus, ginseng may be useful for treatment where EGFR-TKI resistance is observed. Moreover, (20 S)-protopanaxatriol, an aglycone of ginsenosides, has been used for reducing the contents of intracellular lipid droplets, ultimately reversing gefitinib resistance. 47
In addition, astragalus polysaccharides, which are components of astragalus, may downregulate the PI3K/AKT signaling pathway of human lung cancer through autophagy. 48 Cantharidin has been shown to impede NSCLC A549 cell growth and migration and promote autophagy and apoptosis. 49 Acanthopanax senticosus polysaccharide extract from the root of Eleutherococcus senticosus decreases the proliferation, invasion, and migration of NCI-H520 cells (human tumor cell line). 50 ADI also enhances anti-tumor immunity, 51 restoring cellular immunity damaged by platinum-based chemotherapy, 33 and reduces chemoradiotherapy-related toxicities. 30,52 These findings may provide evidence to support the clinical benefits of ADI for patients with NSCLC from the molecular point of view, and the effects of ADI and EGFR-TKI therapy might be directly associated with benefits for these patients.
However, ADI plus first-generation EGFR-TKIs needs to be further investigated. Moreover, improving the methodological quality of RCTs is critical and more methodologically rigorous studies are needed to confirm these findings. The methodologies of the 8 included studies had some limitations. First, all the RCTs claimed random assignment of interventions; however, only 5 described the method of randomization and none mentioned the concealment of treatment allocation. Second, none of the trials mentioned blinding and intention-to-treat analysis. Only 1 of the trials noted that there were no dropouts. Therefore, selection bias, performance bias, and detection bias may exist in the selected studies. Third, only 3 studies provided information on EGFR mutation status, which may have led to clinical heterogeneity. Furthermore, the 8 studies included 1 group treated with ADI combined with EGFR-TKI and another with EGFR-TKI only; thus, the absence of a placebo group may have led to false-positive results. Funnel plots could not be produced due to the insufficient number of trials.
Conclusion
Combination therapy of ADI with EGFR-TKI is beneficial in treating NSCLC and may increase the ORR and DCR, decrease the risk of developing a rash, and improve immune function. To confirm these conclusions, RCTs with larger sample sizes and better study designs are warranted.
Footnotes
Authors’ Note
Na Xiao and Hailang He: Methodology, writing original draft, visualization, and project administration. Jing Wang and Li Zhang: Software analysis, formal analysis. Fanchao Feng and Yong Xu: Data curation and investigation. Brandon Chow: Writing, reviewing, and editing. Jingyi Huang: Validation of the study. Xianmei Zhou and Rui Dong: Conceptualization and supervision. Specific study data are available from the corresponding author upon request. No ethical approval was required for this manuscript because this study did not involve human subjects or laboratory animals. Na Xiao and Hailang He are co-first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.