
Abstract
Background:
Nationwide measles immunization campaigns are resource-intensive yet can fail to reach the same children who are not reached by routine immunization services. Alternative approaches to better reach missed communities and improve efficiency focus on identifying and reaching unvaccinated, “zero-dose” children. Understanding the scope and impact of these strategies can inform approaches to fill immunity gaps and reduce measles disease burden.
Objectives:
We conducted a scoping review to map the existing literature on supplemental strategies used to reach zero-dose or under-vaccinated children in low- and lower-middle-income countries (LLMICs).
Eligibility criteria:
Our review focused on the “reach” component of the Identify-Reach-Monitor-Measure-Advocate (IRMMA) framework. We included literature describing vaccination interventions for measles-rubella, polio, and the Essential Program on Immunization (EPI) in LLMICs published from 2010 to 2021 in multiple languages. We excluded papers that solely focused on non-selective national vaccination campaigns.
Sources of evidence:
We searched peer-reviewed databases (PubMed, WorldWideScience, and Scopus) and gray literature in World Health Organization (WHO) regional databases, the WHO Institutional Repository for Information Sharing, and John Snow, Inc. resource libraries.
Charting methods:
Screening and extraction were conducted in Covidence. We iteratively coded, classified, and analyzed extracted data. Interventions were classified into the IRMMA framework categories: demand generation, human resources, supply chain, and service delivery.
Results:
Of 9450 articles screened, 185 met criteria for inclusion in the final analytic set. Strategies consisted of enhancements to the routine immunization program, with service delivery being the most frequent, followed by demand generation. Many studies described the integration of multiple strategies, offering opportunities to maximize reach and impact.
Conclusion:
The vaccination strategies other than campaigns described in this review have been implemented in multiple countries; some demonstrate greater potential to reach zero-dose and under-vaccinated children. In the face of an evolving funding environment, prioritizing interventions that are most likely to reach unvaccinated children is key.
Plain language summary
Large measles vaccination campaigns use a lot of resources but still often miss the same children who don’t get routine vaccines. To fix this, some health programs try new ways to find and vaccinate children who have not received any vaccines—called “zero-dose” children. This study reviewed existing research to understand which strategies work best to reach these children in low- and middle-income countries.
The review looked at programs focused on reaching children with vaccines for measles-rubella, polio, and other routine immunizations. It included studies published between 2010 and 2021 and excluded ones that only looked at national mass campaigns.
Researchers reviewed 9,450 articles and found 185 that matched their criteria. The most common strategies involved improving how and where vaccines are given (service delivery), followed by efforts to increase demand for vaccines. Many programs used a mix of approaches to be more effective.
In summary, there are many strategies beyond large campaigns that have been used in different countries to reach unvaccinated children. Some of these approaches may be more effective and should be prioritized, especially as funding becomes more limited.
Keywords
Introduction
Many countries rely on nationwide, non-selective vaccination campaigns to close measles and rubella immunity gaps. The World Health Organization (WHO) recommends that countries conduct periodic vaccination campaigns until routine immunization coverage with two doses of measles-containing vaccine (MCV) is at least 90% for three consecutive years. 1 However, campaigns—which involve vaccinating all children within a specified age range regardless of prior vaccination status—are resource-intensive and imprecise. 2 These campaigns may fail to reach children most in need, such as in remote, impoverished urban, or conflict-affected areas that are underserved by routine immunization services. 3 In addition, campaigns are resource intensive, demanding extensive time, staffing, and financial support, often diverting resources from routine programs. 4 Campaigns often miss zero-dose children and can result in substantial revaccination of children who previously received at least one or two doses of MCV. 5
New approaches are needed to better reach the highest-priority populations and improve resource utilization. 3 Rather than vaccinate all eligible children, these supplemental strategies focus on reaching under-vaccinated (children who have not received the full schedule appropriate for their age) and zero-dose or unvaccinated children (defined, in this review, as children who never received a dose of diphtheria-tetanus-pertussis containing vaccine (DTP1)). In countries with high-performing vaccination programs, supplemental strategies tailored to identify and fill immunity gaps could improve equity and more effectively reach zero-dose children. To enact these strategies, policymakers need to have the resources and support to shift from non-selective, nationwide campaigns to more targeted strategies. However, the evidence base for countries to select among these strategies is inadequate.
We conducted a scoping review to help countries identify more effective alternatives to nationwide, non-selective campaigns. Our aims were to assess the existing body of literature on supplemental strategies that have been used to reach zero-dose or under-vaccinated children in low- and lower-middle-income countries (LLMIC), and to understand how these strategies were used and tailored to populations of interest.
Materials and methods
We conducted a scoping review guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Scoping Review Extension recommendations. 6 We identified articles published from 2010 to 2021 to capture literature around Gavi funding strategies for MCV/measles-rubella vaccine (MR). We searched three databases of peer-reviewed literature (PubMed, WorldWideScience, and Scopus) and gray literature identified in WHO regional databases, the WHO Institutional Repository for Information Sharing (WHO IRIS), and John Snow, Inc. (JSI) resource libraries. Search terms were related to child immunization in LLMICs, developed in consultation with immunization experts and a reference informationist at the Johns Hopkins Welch Medical Library (Supplemental Materials, Annex 1). JSI papers were identified by the study team through manual review.
Screening and extraction were conducted in Covidence, adhering to the inclusion and exclusion criteria outlined in the Supplemental Materials, Annex 2. 7 Each article was screened by two reviewers based on title and abstract, with conflicts resolved by discussion with the full research team. Full-text screening was completed by two reviewers for each article, with conflicts resolved by a third reviewer or by consensus. We included papers that identified or characterized un/under-vaccinated children in LLMICs and described tailored strategies to reach them. We further refined our inclusion criteria and conducted a second round of full-text screening to limit the scope of this review on interventions most relevant for measles vaccination strategies—those describing interventions for antigens that have historically relied on campaigns (i.e., MCV/MR and polio) or the Expanded Program on Immunization (EPI) as a whole; interventions that focused on the “reach” component of the Identify-Reach-Measure-Monitor-Advocacy (IRMMA) framework 8 ; and interventions in LLMICs. To prevent duplication and complement a scoping review by Bhatnagar 9 we excluded literature and materials that exclusively described non-selective vaccination campaigns. We included national immunization days, child health days, and other campaign-like activities that were excluded from the Bhatnagar review.
We identified 9450 titles through our search strategy. After excluding duplicates, we screened the titles and abstracts of 8239 based on our inclusion and exclusion criteria (Supplemental Materials, Annex 2). We screened the full text of 2451 articles and extracted data from 256 articles. We then conducted a second round of full-text screening. Data extraction was completed by one reviewer per article, with 10% of extraction validated by a second reviewer. We iteratively coded, classified, and analyzed extracted data. Preliminary groupings were established in consultation with expert reviewers and project leadership, in alignment with the IRMMA framework (Figure 1). Classifications are defined in the Supplemental Materials (Annex 3).
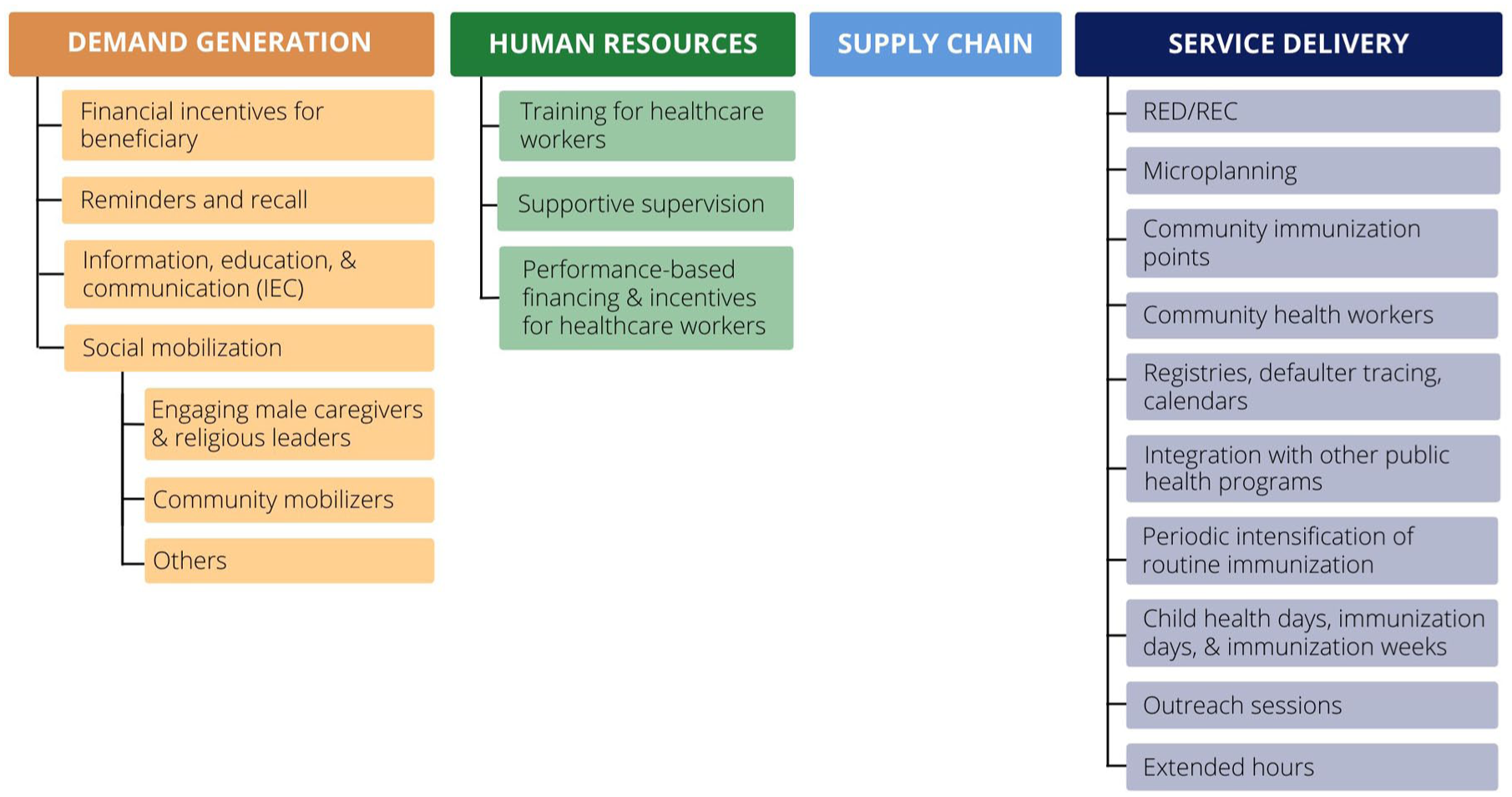
Classification of supplemental strategies in line with IRMMA framework. 8
Results
We included 185 total articles in the final analytic set, as shown in the PRISMA flow chart (Figure 2).
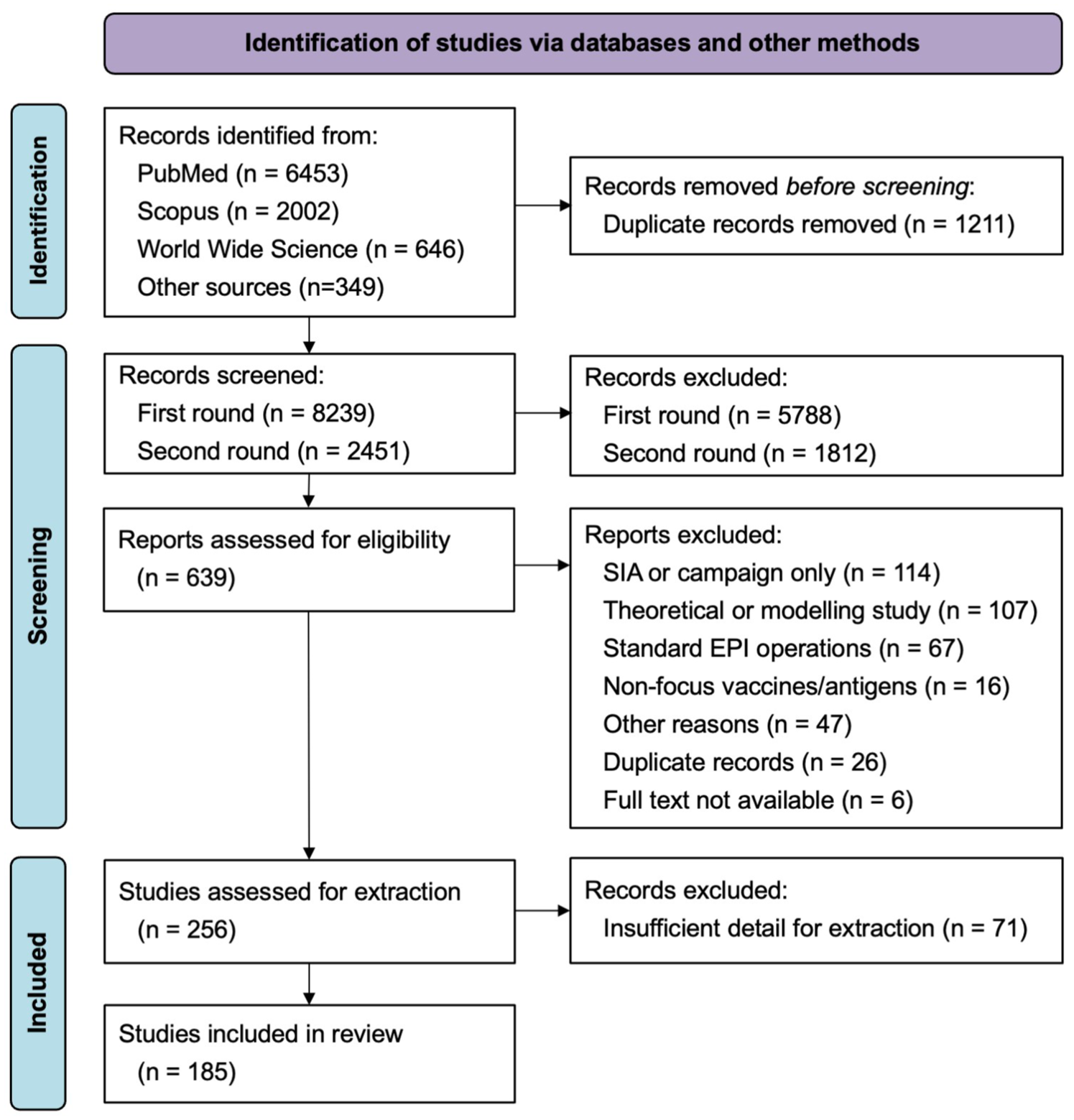
PRISMA flow diagram. 10
The most common countries were India (n = 42), Nigeria (n = 30), and Pakistan (n = 12), countries with high numbers of unvaccinated and under-vaccinated children and among the last countries with endemic wild poliovirus (Figure 3).11,12 Supplemental strategies were applied at various levels, with district-level implementation most frequently reported (n = 49, 26%).
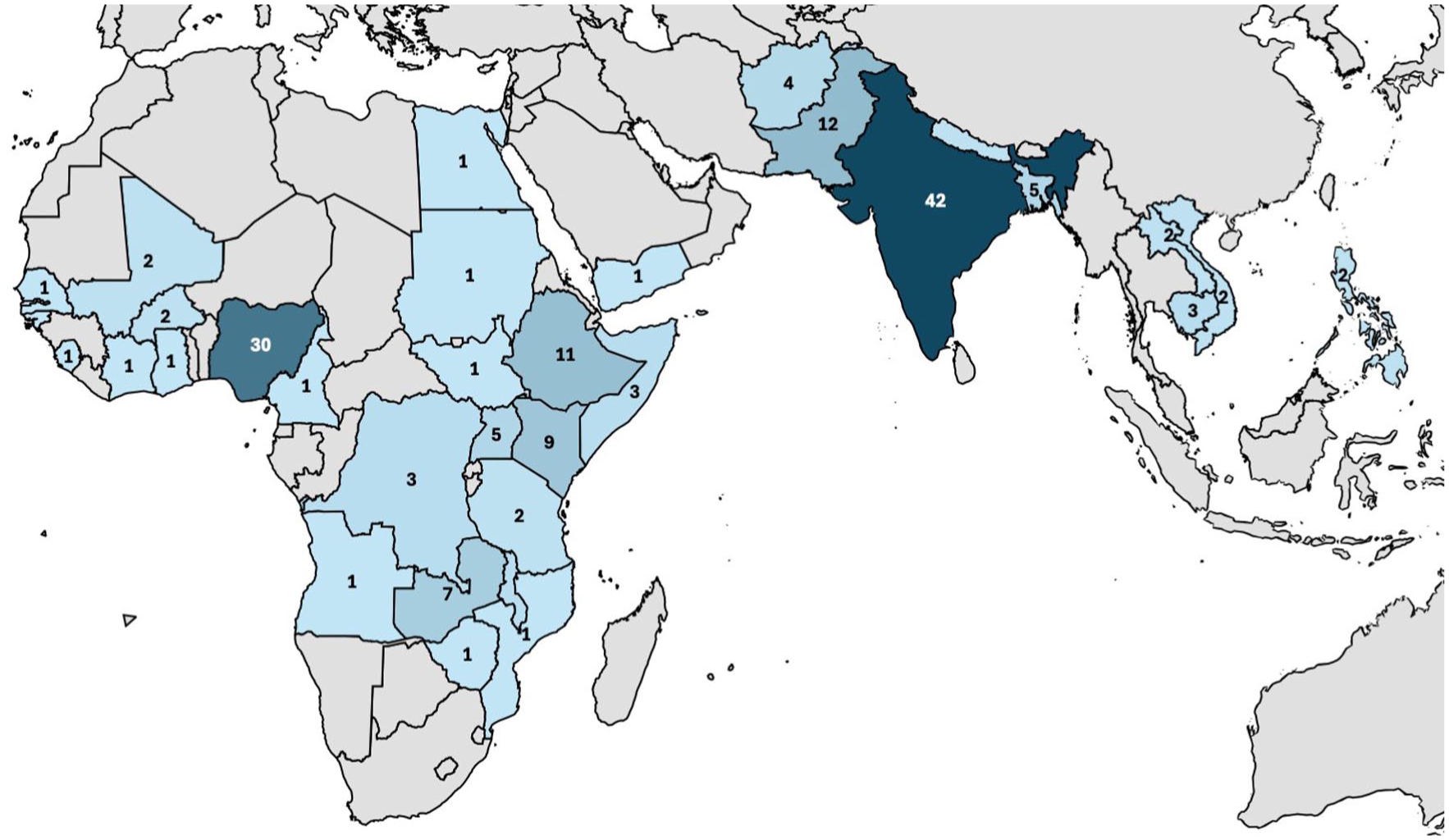
Geographic distribution of included studies indicating a specific focus country where supplemental strategies were implemented; multi-country reviews and global/regional studies not shown (n = number of studies).
Applying the IRMMA framework, most articles focused on service delivery (n = 106, 57%) or demand generation (n = 91, 49%) (Figure 4). Many articles reported multiple interventions across IRMMA categories. Importantly, several interventions frequently appear together in the literature—for example, Reaching Every District (RED)/Reaching Every Child (REC) and microplanning—as they are often part of a comprehensive strategy. Further details by intervention type (Annex 4) and article (Annex 5) are provided in the Supplemental Materials.
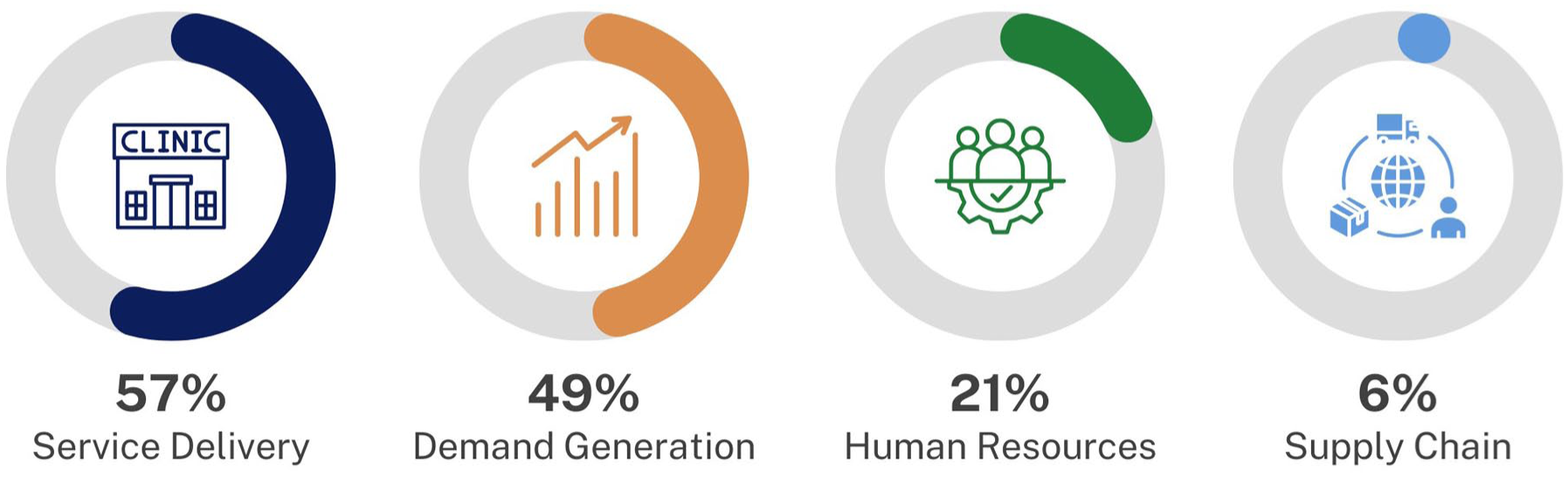
Number of included articles by IRMMA factor addressed.
Service delivery
Within service delivery, interventions included those focused on identifying and vaccinating children (i.e., RED/REC, microplanning, community immunization points, and community health workers (CHWs)), those linking immunization to another public health priority or department (i.e., immunization registries, defaulter tracing, and multi-intervention integration), and those in which routine immunization services were adapted to reach unvaccinated or under-vaccinated children (i.e., periodic intensification of routine immunization (PIRI), child health days/weeks, outreach sessions, and extended clinic hours; Table 1).
Illustrative examples of service delivery interventions.
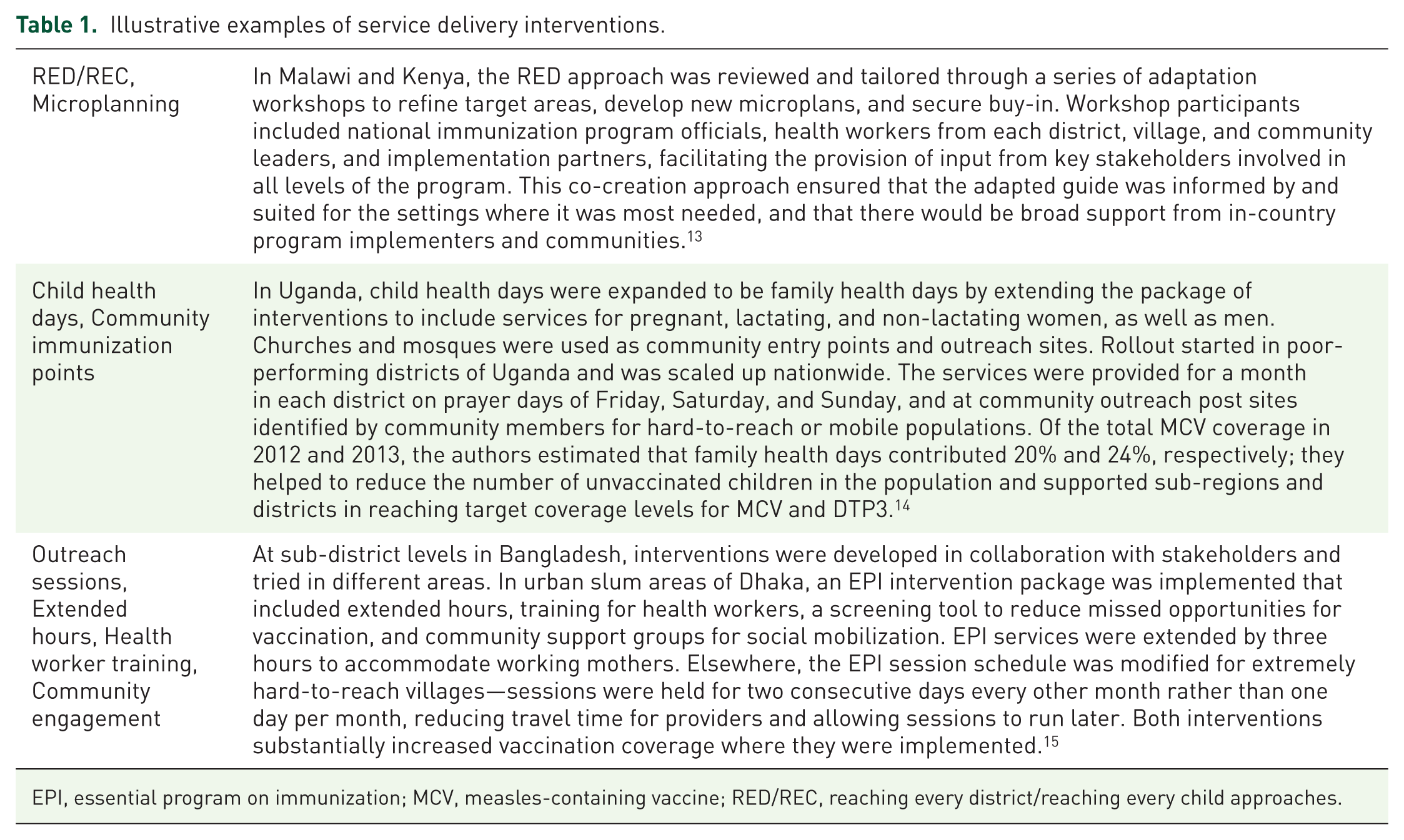
EPI, essential program on immunization; MCV, measles-containing vaccine; RED/REC, reaching every district/reaching every child approaches.
The RED/REC approach—a community-based strategy originally developed by the WHO Regional Office for Africa that aims to identify and reach every unimmunized child in every district—was discussed in 14 articles.13,16–28 Since 2002, RED/REC has been hailed as an effective strategy that can be tailored to meet local needs and target high-priority areas, with many reporting sustained gains in immunization coverage and improvements to data quality, and CHW engagement. 29
Microplanning was the primary focus in 13 papers, frequently with RED/REC implementation.13,16,17,19,28,30–37 Microplanning allowed for tailoring to reach remote, isolated, marginalized, or conflict-affected areas. Articles highlighted the importance of a robust initial microplanning process and iterative updates to adapt to evolving program needs. Immunization coverage gains were not specifically attributed to microplanning but focused on geographic areas and communities with relatively low vaccination coverage.
The use of registries, defaulter tracing, and calendars to identify and reach under- and unimmunized children was discussed in 18 papers.26,38–54 Most also discussed the use of community mobilizers or reminder systems, highlighting the importance of integrating these planning approaches with demand generation. The registry tools described were often digital, requiring software and apps. Several papers highlighted this learning curve and the associated costs of software and app development as potential barriers to effective implementation. Most settings employing these strategies saw an improvement in immunization coverage and timeliness, though the specific boost provided by the registries and tracing approaches often could not be separated from other interventions. Defaulter tracing—engaging health workers (or technologies) to follow-up with children who missed immunization appointments or doses—was also beneficial. However, there are substantial technology and human resource costs to implement these types of planning strategies.
Integration with other public health programs was described in five articles.55–59 Vaccination strategies were linked to broader maternal and child health, maternity care, malaria, HIV/AIDS, and water, sanitation, and hygiene (WASH) initiatives to leverage the reach and demand for these services to improve vaccination uptake and vice versa. Integration had mixed results for vaccination coverage, with some studies finding no association or even reductions in vaccine uptake when linked to other services, while others saw some improvements. One cluster randomized trial that explored integrating infant malaria treatment noted a significant improvement in MCV, DTP2, and DTP3 coverage. 57 Many authors noted that structural and access barriers, such as distance to a facility, prevented vaccination coverage improvements even as other service uptake improved through integration.
CHWs were reported in 25 papers.24,25,31,36,41,45,46,51,53,60–75 CHWs provided a range of maternal and newborn care services. Engaging at these time points provides the opportunity to educate families on a range of topics, including nutrition and immunization. Effective CHW programs face the challenges of building and maintaining community trust and quality service delivery. Some settings establish specific criteria for CHWs, such as India’s ASHA network. The impact of CHWs in improving vaccination coverage varied by setting and priority interventions, and several studies highlighted statistically significant but small changes to full immunization status and uptake of health services. Almost all emphasized the need to support continued training, capacity development, and retention strategies for CHWs, including payment, and the need to strengthen political and programmatic support for sustainable CHW networks.
Community immunization points were set up to reach children in places where they frequent, as reported in 18 articles.18,28,30,35,66,67,69,76–86 These included schools, transit points, and border posts for mobile populations, and, in conflict-affected and emergency settings, permanent polio vaccination teams or security personnel to provide vaccination. The ability to quickly mobilize resources when there is an opportunity is important in conflict-affected settings, but some strategies may carry potential implications for community trust and vaccine acceptance.
Of the five papers that described PIRIs, most were India’s Mission Indradhanush program in districts with low vaccination coverage and high dropout rates.18,87–90 This comprehensive program included door-to-door identification of children missing vaccination, development of district-level planning to decide vaccination sites, social mobilization by CHWs, and immunization sessions done seven consecutive days per month. There was a focus on sessions reaching urban slums, nomadic populations, and other underserved areas.
Child health days, immunization days, and immunization weeks were described in 24 articles. In most cases, these events offered other services in addition to immunization, such as growth monitoring, vitamin A supplementation, oral rehydration therapy, and malaria prevention and treatment.14,18,20,30,63,76,77,84,91–106 Services were provided at different venues, including households, health facilities, schools, and community outreach posts, as noted above. In some countries, child health days and immunization weeks were routinely conducted to catch-up children who missed routine immunization, such as in Sierra Leone. 95 Other countries implemented subnational immunization days to target provinces or districts with poor immunization coverage, hard-to-reach populations, interruptions in the routine immunization system, or recent outbreaks. These were most often done for polio vaccination. In conflict-affected settings (e.g., Yemen and Somalia), these interventions were crucial to delivering services to children, as the routine system had been disrupted for extended periods.
Planning for outreach sessions in 25 articles included using quantitative and/or qualitative data to determine which communities were underserved and had the highest number of zero-dose children, for optimal targeting of sessions in those areas.17,20,21,24,28,32,34,40,41,78,84,97,100,107–118 Some outreach sessions were conducted via mobile clinics or teams that changed location to reach remote communities during different seasons. Four articles described extended hours for vaccination sessions in urban areas, including urban slums, to increase opportunities for caregivers to bring children for vaccination.15,24,45,119
Demand generation
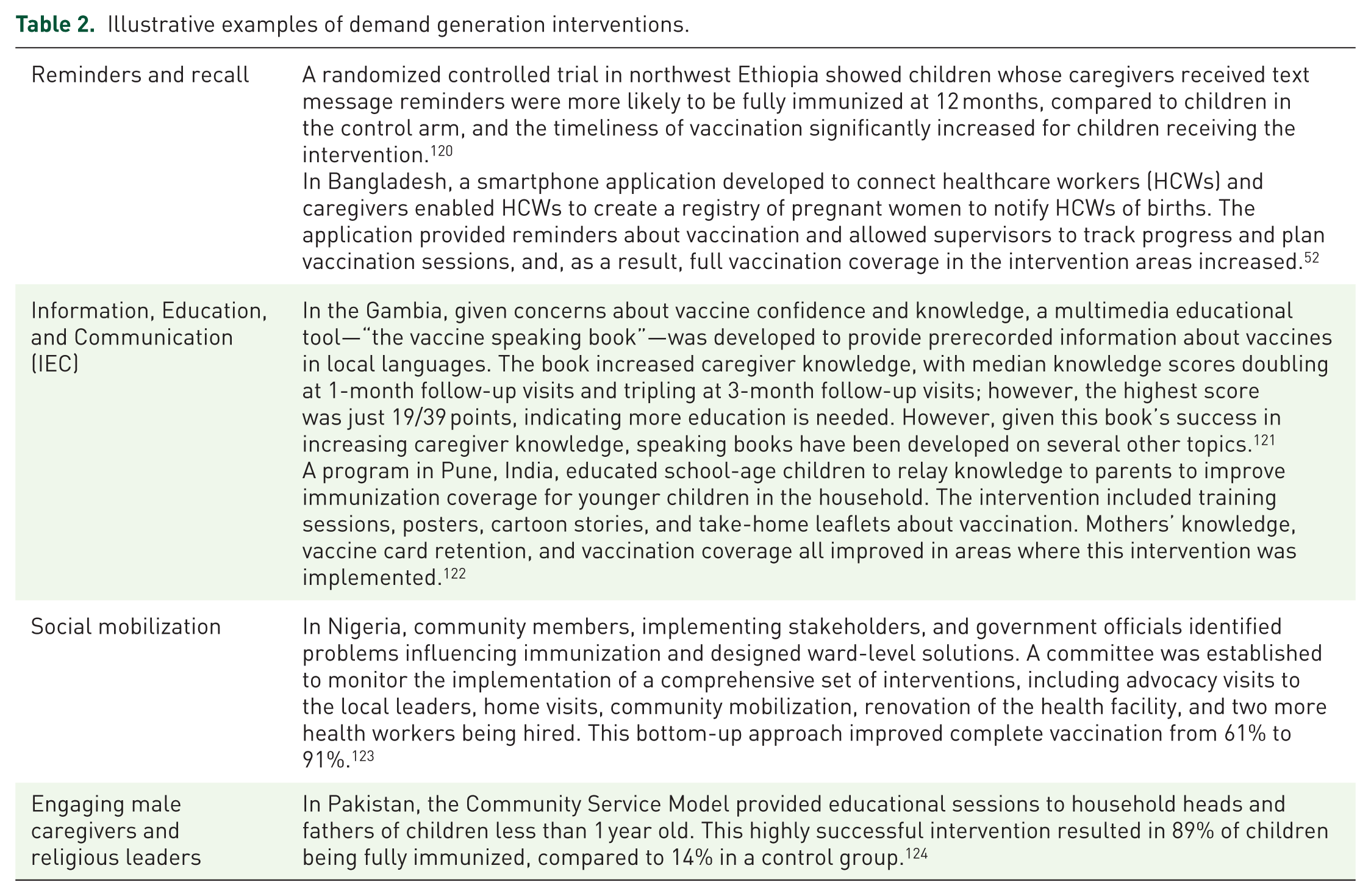
Demand-side interventions—in 91 (49%) articles—included financial incentives for caregivers; reminder and recall systems for caregivers when vaccinations are due; and information, education, and communication interventions to educate caregivers. Social mobilization—including mass media, community mobilizers, village committees, male caregivers, and religious leaders to promote vaccination—was discussed in more than half of demand generation articles (51, 56%) and seemed to work well in all contexts. Social mobilization is considered a key aspect of immunization programs. Of the 91 articles describing demand generation interventions, 28 (31%) included reminder and recall systems. Providing information and education to caregivers seemed successful in all contexts (Table 2).
Illustrative examples of demand generation interventions.
Sixteen studies reported on financial incentives to beneficiaries to improve vaccine uptake, including conditional and unconditional cash transfers, microcredit, and voucher programs.24,63,75,125–137 A meta-analysis by Bassani et al. found little or no evidence of a beneficial impact of financial incentives on vaccination coverage and a small, but nonsignificant, improvement in vaccination coverage due to cash transfers. 134 A review by Cruz et al. found that cash transfers mostly improved vaccination coverage for children under-five, though such transfers alone may not ameliorate inequities in immunization. 132 Many of the financial incentive articles indicated some increase in vaccination coverage, varying by antigen and region. Most focused on cash transfers, whereas Bassani et al. explored incentives more broadly, including microcredit, voucher schemes, and user fee removal. 134 For measles vaccination, studies were mixed in terms of coverage improvements from conditional cash transfers, although not all studies provided cash transfers up to the age of measles vaccination.
Use of reminders (SMS or voice) and recall to notify caregivers when vaccinations are due was frequently coupled with another intervention component and was described in 28 articles.24,37,38,42,47,50,52,75,93,120,135–152 In five studies, caregiver reminders were implemented with financial incentives.24,93,135–137 Some studies not only sent tailored reminders about vaccines due but also to provide educational messaging on immunization and child health. Most studies found that reminder systems improved vaccination rates, as did two systematic reviews.137,141 Reminders were frequently implemented sub-nationally (e.g., villages, health facilities, and city zones). Innovation included mHealth technology that linked an electronic registry with reminders and an application for HCWs to list and track children and remind parents of vaccines due.
Information, education, and communication (IEC) interventions, described in ten articles, focused on educating communities about immunization.24,51,114,118,121,122,143,149,153,154 While some interventions used traditional peer-to-peer approaches or groups, half of these interventions used mHealth platforms to disseminate information. There were also several “edutainment” interventions that provided content in an engaging manner.
Social mobilization interventions in 51 articles included different initiatives: mass media promotion, community meetings, village development committees, and training and sensitization for journalists, teachers, village leaders, community-based organizations, government officials, and other stakeholders.14,15,30,31,33–36,39,43–46,51,54,63,68,75,78,83,86,98,99,114,117,119,123,124,135,152,153,155–175 Social mobilization articles were generally in three subgroups: those engaging male caregivers and religious leaders, community mobilizers, and other approaches.
Engagement of male caregivers or religious leaders to promote vaccination was reported in 16 articles.14,15,30,39,51,54,78,99,119,124,152,163,166,169,171,174 In areas where male caregivers or heads of household have significant influence on vaccination decisions, this intervention can be particularly successful. Where religious leaders are influential and trusted sources of information, they can use their platform to promote vaccination. Engagement of religious leaders was often done as a component of additional social mobilization activities.
In 31 papers, community mobilizers had responsibilities ranging from defaulter tracking and creating registries of children to be vaccinated to providing educational messages.15,31,33–36,39,43,44,75,78,83,86,98,114,117,119,135,153,155,157–162,164–166,170,175 They were sometimes involved in surveillance activities (e.g., acute flaccid paralysis) or promoting other health programs like growth monitoring and nutrition and WASH. In half of the studies, community mobilizers were part of a broader social mobilization strategy that included other interventions. A few studies provided community mobilizers with financial remuneration or phone credit time, but costs were mostly related to training. All studies described using community mobilizers as a successful strategy for increasing demand for vaccination; most were from India and Nigeria, established for polio vaccination.
Other social mobilization approaches were discussed in 20 articles.44–46,63,68,78,98,114,117,123,155,156,158,164,166,167,169,172–174
Human resources
Human resource interventions included healthcare worker training, supportive supervision, and financial incentives for healthcare workers (Table 3). Of the 38 articles, more than half included training. Supportive supervision seemed successful in all contexts.
Illustrative examples of human resources interventions.

EPI, essential program on immunization.
Health worker staffing and training, described in 24 articles, included a variety of programs: peer mentoring, coaching, collaborative learning, refresher sessions, and manager training.15,24,34,36,37,44,45,49,54,75,98,112,115,119,145,154,155,176–182 Training topics ranged from vaccine administration and scheduling, adverse events, facility management, interpersonal communication, and promotion of vaccines. Some programs were designed for training with healthcare workers and community members, while others implemented existing training, such as curricula created by the WHO. Training success was often measured by knowledge improvements, vaccination coverage, and service quality. Programs generally targeted regions with poor routine immunization performance, low vaccination coverage, and poor provider knowledge.
Supportive supervision of healthcare workers in immunization was included in 11 papers, mainly as a component of multiple interventions.21,24,31,34,35,44,48,52,118,176,183 Supportive supervision was provided in conflict-affected regions, primary health centers, and to EPI staff. One paper focused solely on supportive supervision, primarily monitoring EPI performance, correcting errors, and monitoring progress. Outcomes for all interventions using supportive supervision were improvements in immunization coverage, data quality, knowledge, attitudes, and practices.
Financial incentives for healthcare workers in nine articles included performance-based financing (PBF) for CHWs, such as ASHAs in India.31,93,133,178,184–188 In studies utilizing vouchers and direct payments, performance was measured through services performed: vaccinations, consultations, and planning services. PBF effects were measured through vaccination coverage, quality of care, vaccine availability at intervention facilities, staff attitude, staff morale, and staff punctuality. For vaccination coverage, results were generally mixed, with an almost equal split among interventions seeing improved coverage and interventions seeing no impact or only small improvements. Authors speculated that unsuccessful schemes could have been challenged by possible demand-side barriers, vaccine stock-outs, and other health financing reforms that crowded out the effects of the PBF. PBF schemes were also impacted by the existing quality of care and administrative difficulties in calculating and providing vouchers.
Supply chain
Supply chain interventions were described in 14 articles and included vial policies (e.g., open vial policies), vaccines in alternate presentation (e.g., reducing doses per vial), cold chain improvements, and vaccine distribution changes (Table 4).46,48,54,101,189–198 Healthcare workers preferred lower-dose vials, resulting in increased vaccination coverage. Open vial policies were associated with lower wastage.
Examples of supply chain interventions.

MCV, measles-containing vaccine.
Improved cold chain, specifically increased refrigerator availability, was associated with increased vaccination coverage but presented funding challenges for procurement and maintenance of new equipment, increasing vaccine delivery costs. Distributing vaccines straight to facilities rather than through subnational warehouses reduced stock-outs and improved vaccination coverage. We did not include supply chain maintenance or expansions for new vaccine introductions.
Multiple interventions
Just over 40% of included papers (n = 79) described programs or strategies that incorporated multiple components rather than a single intervention (Figure 5). Service delivery interventions were often combined (i.e., microplanning and RED/REC) or paired with interventions in other IRMMA categories, such as demand generation. The most common overlapping interventions were social mobilization with community mobilizers and healthcare worker staffing and training. Strategies that engaged community mobilizers were frequently accompanied by other interventions, especially other social mobilization activities and enhanced healthcare worker training and staffing (Supplemental Materials, Annex 6).

Articles that included two or more strategies, color-coded by IRMMA framework component.
Discussion
Vaccination campaigns remain a key strategy to close immunity gaps, but tailored strategies may more effectively and efficiently reach un- and under-vaccinated children. In the context of volatile funding and donor priorities, along with constrained resources, it has never been more essential for countries to have access to a range of options to leverage existing systems and structures to maximize EPI reach and impact. This scoping review is among the first to broadly explore how immunization programs in LLMICs are adapting approaches to improve vaccine uptake and coverage. We identified 185 articles published between 2010 and 2021 that described service delivery, demand generation, supply chain, and human resources interventions to reach under-vaccinated and zero-dose children in LLMICs.
Coordinating multiple interventions for co-delivery and tailoring to the appropriate local context offers important opportunities to maximize reach and impact. Existing initiatives can be leveraged to include additional interventions, reflected by the community mobilizers being the most common intervention that overlapped with other strategies. For example, India’s ASHA program is used to implement other interventions, such as microplanning and PBF, demonstrating the value community mobilizers have in meeting community needs.72,74,187 Blending multiple strategies into a comprehensive, integrated approach to identify and reach zero-dose or under-vaccinated children is vital to improving the impact of supplemental strategies, which could help to alleviate the need for campaigns.
Some papers described how campaigns provide an opportunity to enhance routine immunization services.37,196 Several interventions were similar to campaigns: child health days, national immunization days, immunization weeks, and PIRIs are all short-term, resource-intensive initiatives that provide additional opportunities to catch-up children who missed routine vaccination. While they include additional outreach or even house-to-house vaccination, the main distinction from campaigns is that they do not blanket vaccinate anyone in the target age group, regardless of previous vaccination status. Some were done nationally, but many were tailored to reach specific populations. These types of tailored approaches may be a viable alternative to nationwide non-selective campaigns.
In an aim to document the range of studies exploring these strategies, we included systematic and umbrella reviews in our analytic set. We found that these reviews are typically more narrowly focused, either reviewing only one type of intervention (e.g., reminder and recall or cash-based incentives) or focused on a particular antigen.132,137,141 In addition to the complementary scoping review led by Bhatnagar, 9 two other scoping reviews have explored strategies to reach zero-dose children. A recently published scoping review by Levin and colleagues focused on economic and costing factors 199 and a review by Beaulieu and colleagues that focused on components of Immunization Agenda 2030. 200 Our review adds important breadth and depth, seeking to capture a more comprehensive snapshot of the strategies in use or potentially of use to countries navigating resource constraints, volatile demand, and complex delivery contexts. We focused broadly on any enhancement to the routine EPI system—approaches that build upon the traditional EPI structures—that was not a vaccination campaign. However, what may be an enhancement in one setting could be a core component of the routine immunization program in others. For example, India’s Universal Immunization Program leverages a broad, multi-level CHW network 160 ; however, CHWs may not be part of the routine program in other settings and would thus be considered an enhancement to the routine immunization program.
In focusing on these routine enhancements, we are challenged to measure intervention-specific impact and quantify the effect of these approaches on immunization coverage, timeliness, and trust. Most studies were evaluations of pilot or implemented programs, and few studies were able to disentangle the effects of a specific approach on target outcomes or capture individual data showing the effect of the intervention.129,179 These tended to be studies with a quasi-experimental design. Many studies relied on Demographic Health Surveys or other surveys to associate interventions with changes in population-level coverage, which falls short of describing local effects in the communities with more under- or unvaccinated children. We noted that just 11% of included articles had a qualitative component. Further implementation research is essential to better describe the effectiveness, efficiency, and acceptability of these interventions. Pairing quantitative learnings with qualitative data detailing healthcare worker and caregiver perspectives on these interventions is a key opportunity to inform the selection and tailoring of campaign alternatives to best suit the needs and preferences of the communities they aim to serve. Both are important areas needing further study and, crucially, documentation of activities already underway in EPI programs in LLMICs but not yet incorporated into the published literature base.
Few studies estimated the economic costs of these routine enhancement programs, nor the return on investment. One example was the Bangladesh intervention package, including extended hours, training, a missed opportunities screening tool, and community mobilization. The cost to implement the strategy was estimated at $20.95 per fully immunized child; however, it is unclear how this compares to the cost of providing vaccines via a campaign. 15 Some papers did discuss incremental costs or other resource needs, such as the number of worker-hours per month needed for defaulter tracing, 32 but these costs are heavily influenced by local context and the ability to mobilize existing networks. Of note, Levin et al 199 focused on economic interventions and analyses and similarly found a dearth of economic evidence. Taken together with our findings, this highlights the need to better understand the opportunities and tradeoffs of economic interventions (like PBF for health care workers, or financial incentives for program beneficiaries) and other strategies, especially compared to the cost of nationwide campaigns or the vaccine-preventable cases and deaths resulting from persistent immunity gaps.
We acknowledge several limitations. Our findings are likely influenced by publication bias toward positive outcomes and language bias. We identified several studies that reported neutral or nonsignificant results, but few reported negative findings. There were a few reports of a measurable impact of each intervention type, primarily due to a lack of appropriate comparison groups. Where possible, we included descriptions of study results, summarizing the approaches and highlighting select examples with more generalizable contexts or specific outcome measures. We did not include a formal assessment of data quality in this review, and the quality of study results varied. Most studies reported only short-term outcomes but lacked long-term impact or measures of sustainability. We did not include papers that focused exclusively on conflict-affected areas but captured relevant learnings that could be applied in non-conflict settings; this is an important area needing further study. Finally, we iteratively adjusted our scoping review approach as we learned of complementary work underway. 9 Adapting our approach to avoid redundant efforts helped ensure the results address key knowledge gaps.
Conclusion
Campaign alternatives and routine vaccination program enhancements described in this review have been implemented in multiple countries, yet some demonstrate greater potential to reach zero-dose and under-vaccinated children. More work is needed to better understand the benefits and tradeoffs of different supplemental (non-campaign) strategies—both alone and in combination with other approaches—on vaccination coverage. Contextual tailoring is critical; different settings will likely benefit in differing degrees from implementing the strategies.
As global immunization efforts evolve, there is a need to equip LLMMIC governments and global partners with the insights to make data-driven decisions about which tailored vaccination strategies beyond campaigns can help them best reach un- and under-vaccinated children. In the face of an evolving funding environment and the threat of reemerging vaccine-preventable diseases, prioritizing interventions that are most likely to reach children who have not already been vaccinated will be key. By improving uptake of vaccination through tailored supplemental strategies, countries may improve coverage rates, close immunity gaps, and lessen the need for resource-intensive national vaccination campaigns.
Supplemental Material
sj-docx-1-tav-10.1177_25151355261442364 – Supplemental material for Exploring supplemental immunization strategies to reach zero-dose children in low- and middle-income countries: a scoping review
Supplemental material, sj-docx-1-tav-10.1177_25151355261442364 for Exploring supplemental immunization strategies to reach zero-dose children in low- and middle-income countries: a scoping review by Andrea C. Carcelen, Molly Sauer, Pooja Sangha, Porcia Manandhar, Natalya Kostandova, Alex C. Kong, Rachel Larson, Rupali J. Limaye and William J. Moss in Therapeutic Advances in Vaccines and Immunotherapy
Supplemental Material
sj-docx-2-tav-10.1177_25151355261442364 – Supplemental material for Exploring supplemental immunization strategies to reach zero-dose children in low- and middle-income countries: a scoping review
Supplemental material, sj-docx-2-tav-10.1177_25151355261442364 for Exploring supplemental immunization strategies to reach zero-dose children in low- and middle-income countries: a scoping review by Andrea C. Carcelen, Molly Sauer, Pooja Sangha, Porcia Manandhar, Natalya Kostandova, Alex C. Kong, Rachel Larson, Rupali J. Limaye and William J. Moss in Therapeutic Advances in Vaccines and Immunotherapy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.