
Abstract
Background:
Malaria is a leading cause of death among children under 5 years of age in sub-Saharan Africa. The malaria vaccine is an important preventive measure introduced by the World Health Organization to reduce malaria and its associated mortality and morbidity. We aimed to assess the acceptance of the malaria vaccine among next of kin of children under 5 years of age in Gulu City, Northern Uganda.
Methods:
Between October and December 2023, we conducted a cross-sectional study in Pece–Laroo division, Gulu City, Uganda. Socio-demographic, vaccine profile and health system factors were collected. Multivariable logistic regression was performed using STATA 16 to determine factors associated with acceptance of the malaria vaccine among next of kin of children under 5 years.
Results:
A total of 432 participants were enrolled. Of these, the majority were female (72.5%, n = 313) with most aged 30 years and above (51.2%, n = 221). Overall, 430 (99.5%) participants had good knowledge about malaria. The majority (91.4%, n = 395) had good acceptance of the malaria vaccine. Factors independently associated with acceptance of the malaria vaccine were knowing a child who died of malaria [adjusted prevalence ratio (aPR): 1.07, 95% confidence interval (CI): 1.01–1.13, p = 0.022] and preferring the injection route for a malaria vaccine (aPR: 1.1, 95% CI: 1.06–1.22, p < 0.001). All 395 participants with good knowledge of malaria had good acceptance of the malaria vaccine (p = 0.007).
Conclusion:
There was a high acceptance of the malaria vaccine in Laroo–Pece division, Gulu, Uganda. However, there is a need for further health education to achieve universal acceptability of the malaria vaccine in preparation for the malaria vaccine implementation program in Uganda.
Introduction
Malaria remains an important public health threat to the sub-Saharan region of Africa with enormous health and economic implications. Malaria significantly affects vulnerable populations such as children under 5 years resulting in high mortality and morbidity among this population. The World Health Organization (WHO) reported an estimated 249 million cases of malaria worldwide, resulting in 608,000 malaria deaths in 2022. Moreover, more than 80% of these malaria deaths occurred among children under 5 years of age. 1 Additionally, African countries shared disproportionally high malaria cases and deaths accounting for 93.6% and 95.4% of all reported cases, respectively. 1 Uganda is among the high-burden countries, ranking as the third highest globally with a burden of about 5.1% in 2021. 1 Furthermore, there was a 2% increase in incidence in 2022. 1 The steady rise in the malaria cases especially in the post-coronavirus disease-2019 (COVID-19) era was attributed to the disruption that COVID-19 brought to the malaria prevention and treatment measures enforced by Ministry of Health in Uganda. 2
Despite the decline of malaria deaths among children from 87% to 76% worldwide, malaria is still the leading cause of mortality among children less than 5 years in high-burden countries, like Uganda. 1 However, enormous efforts to curb malaria have been made towards the common goal of decreasing malaria-related deaths including vector control measures, intermittent preventive treatment and antimalarial drugs. Furthermore, the newly rolled out malaria vaccine RTS, S/AS01 through the malaria vaccine implementation programme has reached over 2 million children in Ghana, Kenya and Malawi by 2022 with proven safety and effectiveness.3,4 As such, the malaria vaccine has seen a drop of about 13% in all-cause early childhood deaths as well as a significant reduction in severe malaria cases.3–6 Furthermore, an overall 30% reduction in severe malaria and a 21% reduction in hospitalization due to malaria parasitaemia was reported by WHO in 2021. 6 In fact, in 2021, the WHO recommended the use of the malaria vaccine among children under 5 years in the high transmission countries. 7
However, the uptake of the malaria vaccine is highly dependent on factors such as awareness, willingness and acceptance of the vaccine among caregivers of children under 5 months. 8 Whereas there has been a registered generally low awareness of the malaria vaccine, caregivers are more willing to accept the malaria vaccine as part of the measures to curb the burden of malaria worldwide. For instance, awareness among caregivers in Nigeria was estimated at 40.3% while acceptance was 91.9%. 8 Similarly, the acceptance was estimated at 76% and 81% in Guinea and Sierra Leone. 9 Uganda is among the few countries set to pioneer the enrolment of the vaccine in early 2024; however, the level of acceptance of the malaria vaccine in Uganda remains unknown. 10
Therefore, it is essential to prepare the ground for introducing the vaccine by assessing awareness and willingness to use the vaccine, which is still impeding the acceptance of the vaccine in Africa, Uganda inclusive. Despite the high burden of malaria in most parts of Uganda, including Gulu, there are no studies on the acceptance of the malaria vaccine among these communities. Therefore, in this study, we aimed to assess the acceptance of the malaria vaccine among next of kin of children under 5 years in a rapidly urbanizing city in Northern Uganda.
Methods
Study design
A community-based, descriptive, cross-sectional study was conducted among adults with children 5 years or younger residing in Pece–Laroo division, Gulu City, Uganda between October and December 2023. We followed the Strengthening the Reporting of Observational Studies in Epidemiology Guidelines. 11
Study setting
This study was done in Laroo–Pece division in Gulu city which is a city north of Kampala approximately 333 km from the capital bordered by Pader and Omoro districts in the east, Oyam district in the south, Nwoya district in the southwest, Gulu district to the north, Amuru to the west. The coordinates of Gulu city are 2°46′54.0′′ N 32°17′57.0′′ E. The climate of Gulu city is tropical with two seasons dry season from December to March and wet season from April to November. The economic activities of Gulu City are wholesale and retail trade. Laroo–Pece division has a population of 111,300 people (2014 national census) with 72 villages and 17 parishes.
Inclusion criteria
The study participants were adults aged above 18 years who were parents or guardians of at least a child aged 5 years or younger and health workers in Laroo–Pece division, Gulu City, Uganda.
Sample size estimation
The sample size was estimated using the Kish–Leslie formula with the following assumptions: margin of error of 5%, at 95% CI, the prevalence of the prevalence of willingness modestly estimated at 50% since there was no previous study in Uganda about the acceptability of the malaria vaccine in Uganda. Using a 10% non-response rate the final calculated minimum sample size was estimated at 384 participants.
Sampling procedure
A multi-stage random sampling of the divisions, parishes and villages was done followed by a systematic random sampling of the individual households. Stratified random sampling proportionate to size was done to determine the number of participants from each parish. Households were selected using systematic random sampling, taking the second household unit until the sample size was met.
Data collection
Data were collected over 3 months from October to December 2023 using an interviewer-administered, structured questionnaire administered by trained research assistants who are fluent in both English and Acholi languages with regular supervision. The data collection tool was adapted from questionnaires of previously published studies on knowledge and awareness of malaria vaccine in similar populations in other countries.9,12–14 We identified village health teams (VHTs) practicing within the study area. We conducted a comprehensive 1-day training on malaria, the malaria vaccine, the process of seeking informed consent and reviewed the data collection tools (Supplementary Materia 1_Data Collection Tool). Data collected included socio-demographic characteristics such as age, gender, education level and level of income, occupation of the next of kin, vaccine profile such as route and frequency of administration, side effects of the vaccine and health system factors such as vaccine availability, health worker factors and supply chain.
Statistical analysis
Data was collected using the kobo toolbox and later exported to Microsoft Excel for data cleaning and coding and later imported to STATA MP version 17.0 for analysis. Knowledge and acceptance were scored and categorized as good (score ⩾ 4) and poor (⩽3). The dependent variable and categorical independent variables were summarized as frequency and percentage. Numerical variables were summarized as median and interquartile range (IQR) since they were not normally distributed. The association between dependent (knowledge and acceptance of malaria vaccine) and independent variables was assessed using modified Poisson regression since acceptance and knowledge of malaria vaccine among the participants was >15%. The association between knowledge and acceptance of the malaria vaccine was assessed using Fisher’s exact test as the number of cells in cross-tabulation was less than five cells. p < 0.05 was considered statistically significant.
Results
Study enrolment
Of 447 potential participants screened, 432 were eligible and were enrolled in the study, given a response rate of 97% (Figure 1).

Study flow diagram.
Sociodemographic characteristics
Overall, we included 432 participants, with a mean age of 32.4 years [standard deviation (SD): 10.6]. Participants were almost evenly distributed across age groups, with 48.8% below 30 years (n = 211) and 51.2% aged 30 or above (n = 221). The majority were female (n = 313, 72.5%), and relationships were primarily maternal (n = 267, 61.8%). Christians constituted the predominant religious group (n = 393, 91%), while educational attainment varied, with 38.7% having primary education (n = 167) and 17.4% having tertiary education (n = 75). Employment status revealed a majority being self-employed (n = 273, 63.2%), and 97.9% reported an average monthly income below 100,000 Ugandan Shillings (n = 423). The median family size was 4 (IQR: 3–6), and the majority were not health workers (n = 408, 94.4%). Notably, 87.2% of children had suffered from malaria in the past year (n = 376), and 48.8% of participants knew a child who had died from malaria (n = 211), providing a comprehensive overview of the demographic and health-related characteristics of the study cohort (Table 1).
Sociodemographic characteristics of the respondents Gulu City, Northern Uganda, 2023.

IQR, interquartile range; SD, standard deviation.
Malaria vaccine preference
Most participants (n = 269, 62.4%) showed a preference for injections. About two-thirds (n = 289, 67.1%) of the participants preferred two or three doses of the vaccine (Table 2).
Route and dosing preference of malaria vaccine among the respondents in Gulu city, Northern Uganda, 2023.

Knowledge regarding malaria
Almost all study participants (99.8%, n = 431) had heard of malaria. When asked about the cause of malaria, 96.5% (n = 417) demonstrated awareness. However, awareness of malaria vaccine was reported by 62% (n = 268), and 71.7% (n = 314) believed in its preventability. Regarding the perception of reducing malaria-related fatalities through vaccination, 79.2% (n = 342) agreed. Awareness of the World Health Organization’s recommendation for the RTS, S malaria vaccine for children in Uganda was reported by 60.7% (n = 262). The majority (88.4%, n = 382) believed that malaria is a serious health issue requiring vaccination, and 81% (n = 350) agreed that a malaria vaccine would reduce treatment expenses. Concerns about potential negative health impacts were expressed by 66.4% (n = 287), while 88.7% (n = 383) acknowledged the life-threatening nature of untreated malaria. A notable viewpoint, expressed by 25.7% (n = 111), was the belief that with available treatment and nets, a vaccine is unnecessary (Table 3). Almost one-third of the participants knew about the malaria vaccine from the Radio (n = 113, 26.2%), followed by VHT (26.2%, n = 113), health workers (20.15, n = 87), internet (3.5%, n = 15) and least newspaper (2.1%, n = 9) (Figure 2).
Knowledge regarding malaria and malaria vaccine among the next of kin of children under 5 years of age in Gulu City, Northern Uganda.

WHO, World Health Organization.

Source of information on malaria vaccine among respondents in Gulu city, Northern Uganda, 2023.
Overall, 430 (99.5%) participants had good knowledge about malaria.
Acceptance of malaria vaccine
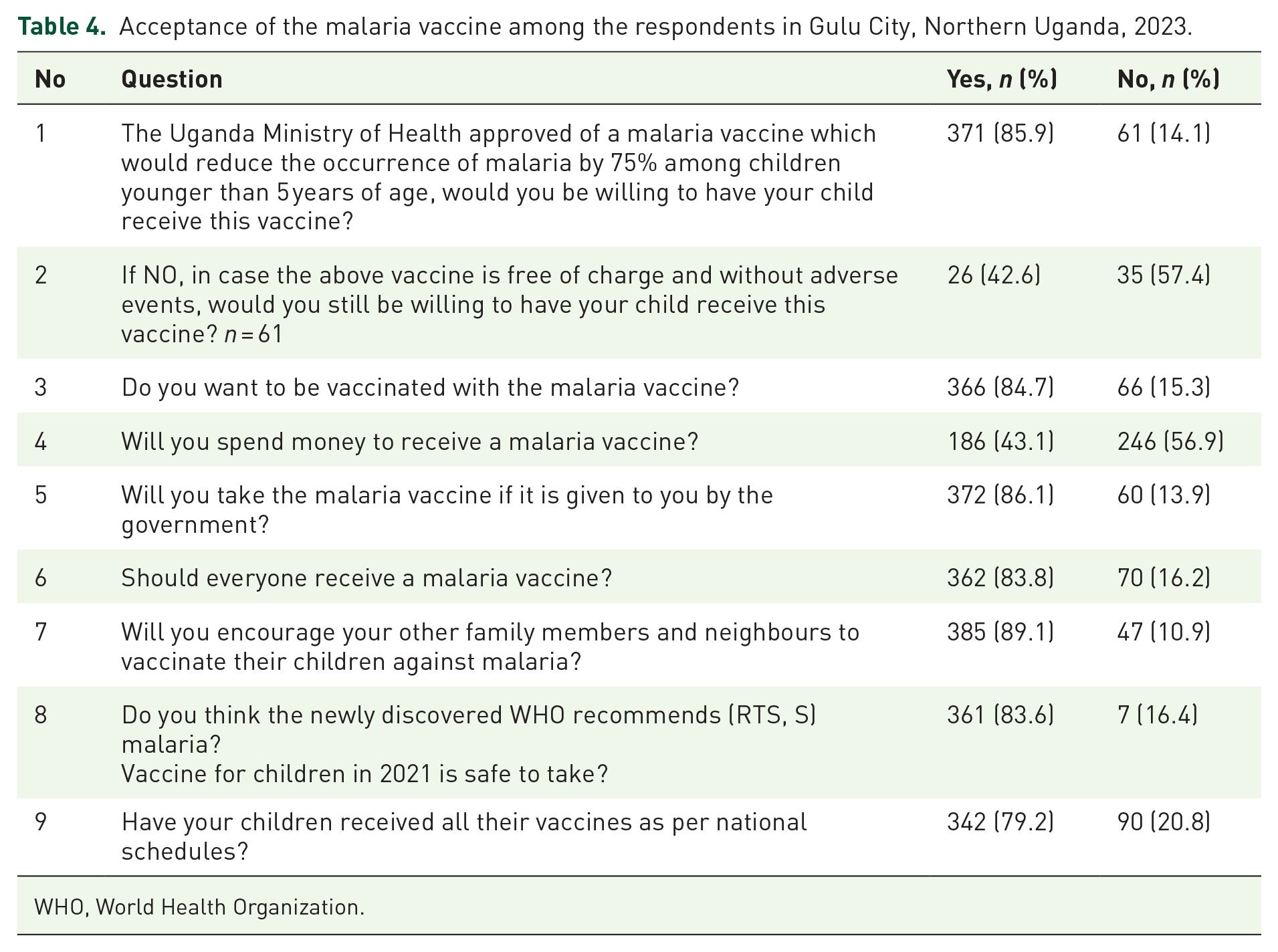
A substantial majority, 85.9% (n = 371), expressed willingness to have their child receive a Ministry of Health-approved malaria vaccine that could reduce occurrences by 75% among children under 5 years of age. In the scenario where the vaccine was free and without adverse events, 42.6% (n = 26) of those initially unwilling indicated a change in their stance. Additionally, 84.7% (n = 366) expressed a desire to be vaccinated themselves, while 56.9% (n = 246) would not spend money to receive the malaria vaccine. Government provision of the vaccine received strong support, with 86.1% (n = 372) willing to take it if offered. The consensus was also evident in the belief that everyone should receive the malaria vaccine (83.8%, n = 362), and a high percentage, 89.1% (n = 385), expressed intent to encourage family members and neighbours to vaccinate their children. Furthermore, the perceived safety of the WHO-recommended (RTS, S) malaria vaccine for children in 2021 was affirmed by 83.6% (n = 361). Lastly, 79.2% (n = 342) reported that their children had received all their vaccines as per national schedules (Table 4).
Acceptance of the malaria vaccine among the respondents in Gulu City, Northern Uganda, 2023.
WHO, World Health Organization.
Overall, 395 (91.4%) participants had good acceptance of the malaria vaccine.
Bivariate analysis of factors associated with knowledge and acceptance of the malaria vaccine
At bivariate analysis, factors associated with good knowledge of malaria were, being a Muslim compared to Christianity (p = 0.008), any level of education compared to informal education (all p values < 0.008), knowing a child ever who suffered from malaria in the past 1 year (p = 0.011) and preference for three doses of the malaria vaccine compared to one dose (p < 0.001).
For acceptance of the malaria vaccine, being a Muslim compared to Christianity (p = 0.022), any level of education compared to informal education (all p values < 0.012), employment compared to unemployed (p < 0.016), knowing a child who died of malaria (p < 0.001) and preference for injection route of the malaria vaccine compared to oral routes (p = 0.01) (Table 5).
Bivariate analysis of factors associated with knowledge and acceptance of the malaria vaccine among the respondents in Gulu City, Northern Uganda, 2023.

CI, confidence interval.
Multivariable analysis of factors associated with knowledge and acceptance of the malaria vaccine
After adjusting for all significant confounders, no factor was found to be independently associated with good knowledge. However, knowing a child who died of malaria (aPR: 1.07, 95% CI: 1.01–1.13, p = 0.022) and preferring the injection route for a malaria vaccine compared to oral administration (aPR: 1.1, 95% CI: 1.06–1.22, p < 0.001) were independently associated with malaria vaccine acceptance (Table 6).
Multivariable analysis of factors associated with knowledge and acceptance of the malaria vaccine among the respondents in Gulu City, Northern Uganda, 2023.

CI, confidence interval.
Association between malaria knowledge and acceptance of malaria vaccine
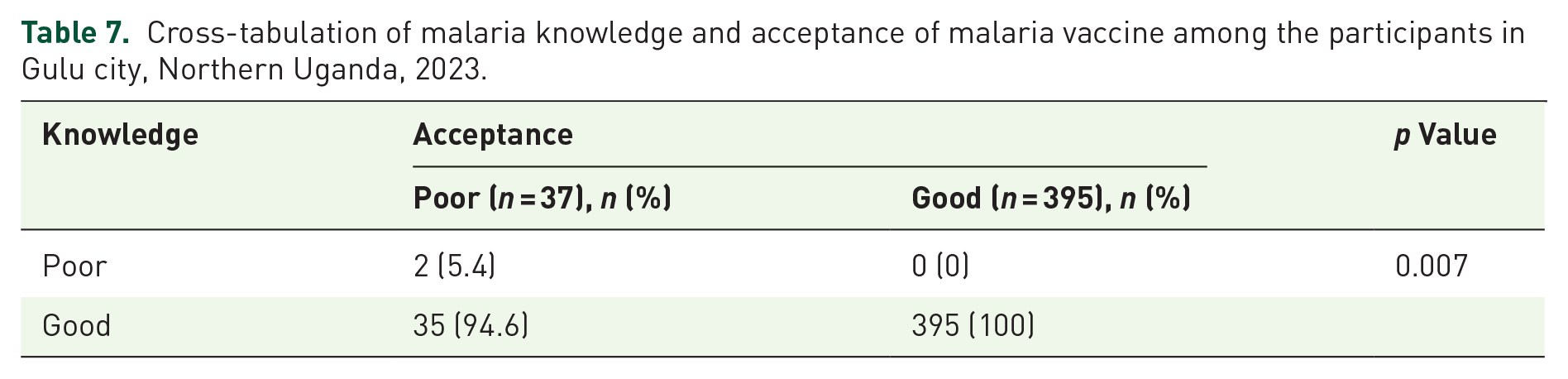
All 395 participants with good knowledge of malaria had good acceptance of the malaria vaccine (p = 0.007) (Table 7).
Cross-tabulation of malaria knowledge and acceptance of malaria vaccine among the participants in Gulu city, Northern Uganda, 2023.
Discussion
Vaccination against infectious diseases such as malaria has had significant success rates with eventual alleviation of the strain on the healthcare systems. 15 While strides have been made to develop the malaria vaccine, assessing the acceptability of the vaccine is important in ensuring the successful implementation of malaria vaccination programmes. 16 In this study, we aimed to assess the acceptance of the malaria vaccine among next of kin of children under 5 years in Gulu, Northern Uganda.
We found a high acceptance of the malaria vaccine among next of kin of children under 5 years at about 91.4% with 85.9% expressing willingness to have their children receive a Ministry of Health-approved malaria vaccine. In addition, a high proportion of caregivers had good knowledge of malaria (99.5%). Our findings are comparable to results from studies conducted in different countries such as Kenya, Nigeria, Bangladesh, Guinea and Sierra Leone where acceptance of the malaria vaccine among caregivers to children below 5 years ranged between 70% and 92%.9,12–14 Similarly, a recent systematic review by Sulaiman et al. 17 revealed a high aggregate malaria vaccine acceptance rate among caregivers of children under 5 years in low- and middle-income countries estimated at 95.3%. On the contrary, another study carried out in southwest Ethiopia showed a significantly low acceptance of about 32.3%. 18 A high acceptance of the malaria vaccine is significantly associated with a high uptake of the vaccine and hence a reduced burden and severity of malaria among children under 5 years. 6 Our study found a high acceptance rate for the malaria vaccine among caregivers of children under 5 years old, which is comparable to studies conducted in other countries. These findings highlight the importance of effective public health education and trust in health authorities. The strong connection between high acceptance and increased vaccine uptake suggests that promoting vaccination efforts could lead to reducing the severity of malaria among young children. Factors such as perceived benefits, community influence, accessibility and positive vaccination experiences contribute to this high acceptance rate. However, the significant difference in acceptance rates seen in studies such as the one in southwest Ethiopia 18 highlights the need for tailored interventions to address regional differences and potential barriers to vaccine acceptance. These findings stress the importance of ongoing efforts to combat malaria by addressing misinformation, improving access to vaccines and building trust in vaccination programs.
In this study, knowing a child who died of malaria and preferring the injection route for a malaria vaccine were independently associated with malaria vaccine acceptance. In addition, all participants with good knowledge of malaria had good acceptance of the malaria vaccine. This aligns with findings from similar studies from Sierra Leone and Tanzania where better knowledge of malaria in addition to higher levels of education was associated with high acceptance of the malaria vaccine.9,19 Furthermore, other factors, such as positive perceptions driven by health education provided by health workers and other opinion leaders in communities about the malaria vaccine, influence the acceptance of the vaccine, consequently increasing the coverage of the malaria vaccination implementation program. 20 Personal experiences about the dangers of malaria including associated mortality are more likely to compel caregivers to embrace preventive measures such as the malaria vaccine.20,21 These findings emphasize the urgent need to improve health education efforts focused on malaria among caregivers of children under 5 years old. By enhancing awareness and knowledge about malaria and the importance of vaccination, particularly in high-transmission areas like Uganda, we can boost acceptance rates of the malaria vaccine. This proactive approach holds promise for reducing the increasing burden of malaria in affected regions. Therefore, targeted educational campaigns aimed at caregivers are essential in our efforts to combat the disease and protect the health of vulnerable populations.
Our study had some limitations. Firstly, the sample size was relatively small, which may limit the generalizability of the results to other populations of children under 5 years in Uganda. In addition, we conducted a quantitative study and hence did not explore the personal experiences of participants to examine the factors associated with acceptance of the malaria vaccine. However, this study provides baseline data for the implementation of the malaria vaccination program in Uganda, aiming to commence promptly and provide improved insights into overcoming barriers to the acceptance of the malaria vaccine, particularly in Northern Uganda and the country.
To overcome the limitations of our study, we suggest a multicentre study recruiting people from all the regions and ethnicities within Uganda. Also, we can use mixed-methods study (both quantitative and qualitative techniques) to understand better why caregivers do or do not accept the malaria vaccine for young children and as well will enable us to understand the personal experiences of the community. We could also study this topic over time to see if things change. Talking with local communities and making plans to help them understand the importance of the vaccine could be helpful too and these will help us learn more about how to make the malaria vaccine program work better in Uganda.
Conclusion
In this study, we found a high acceptance and willingness to receive the malaria vaccination among caregivers of children younger than 5 years of age in Laroo–Pece division, Gulu, Uganda. The considerable demand emphasizes the importance of cautiously managing end users’ expectations as the vaccine is introduced to the public soon. Our findings also point to the necessity for an ongoing sensitization of child caregivers by the health care workers in private and public health facilities as well as the community health workers (such as VHTs), radio and TV stations through relevant messages to enhance their awareness of the vaccine’s significance. Consequently, health education and communication from Ugandan government sources play a crucial role in disseminating more knowledge about the malaria vaccine.
Supplemental Material
sj-docx-1-tai-10.1177_20499361241247467 – Supplemental material for Malaria vaccine acceptance among next of kin of children under 5 years of age in Gulu, northern Uganda in 2023: a community-based study
Supplemental material, sj-docx-1-tai-10.1177_20499361241247467 for Malaria vaccine acceptance among next of kin of children under 5 years of age in Gulu, northern Uganda in 2023: a community-based study by Felix Bongomin, Fiona Jollyne Megwera, Jerry Mundua, Nabirah Naluwooza, Frank Ayesiga, Yakobo Nsubuga, Grace Madraa, Winnie Kibone and Jerom Okot in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-docx-2-tai-10.1177_20499361241247467 – Supplemental material for Malaria vaccine acceptance among next of kin of children under 5 years of age in Gulu, northern Uganda in 2023: a community-based study
Supplemental material, sj-docx-2-tai-10.1177_20499361241247467 for Malaria vaccine acceptance among next of kin of children under 5 years of age in Gulu, northern Uganda in 2023: a community-based study by Felix Bongomin, Fiona Jollyne Megwera, Jerry Mundua, Nabirah Naluwooza, Frank Ayesiga, Yakobo Nsubuga, Grace Madraa, Winnie Kibone and Jerom Okot in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-pdf-3-tai-10.1177_20499361241247467 – Supplemental material for Malaria vaccine acceptance among next of kin of children under 5 years of age in Gulu, northern Uganda in 2023: a community-based study
Supplemental material, sj-pdf-3-tai-10.1177_20499361241247467 for Malaria vaccine acceptance among next of kin of children under 5 years of age in Gulu, northern Uganda in 2023: a community-based study by Felix Bongomin, Fiona Jollyne Megwera, Jerry Mundua, Nabirah Naluwooza, Frank Ayesiga, Yakobo Nsubuga, Grace Madraa, Winnie Kibone and Jerom Okot in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.