
Abstract
Introduction:
Vaccination significantly reduces morbidity and mortality among children from vaccine-preventable diseases. Despite a global and regional immunization coverage estimate of 74%, Ethiopia has ~1,146,000 zero-dose children. Therefore, this study estimated the prevalence of zero-dose vaccination and identified factors and barriers among children under 2 years of age in South West Ethiopia.
Method:
An explanatory sequential mixed-methods design was employed; the quantitative component consisted of a community-based cross-sectional study, and the qualitative component was assessed using a qualitative descriptive approach through in-depth interviews. Following data cleansing, the status of the first dose of the pentavalent vaccination was classified as either “vaccinated for first dose of the pentavalent vaccine” or “not vaccinated for first dose of the pentavalent vaccine.” Then, associated factors of being zero-dose at p < 0.05 were identified using logistic regression analysis. Subsequently, reflexive thematic analysis was employed for qualitative data analysis because it enables both interpretive developments of latent meanings underlying barriers to zero-dose vaccination and inductive coding based on participant narratives.
Result:
The results indicated that 17% of children were zero-dose, and lack of antenatal care visit (adjusted odds ratio = 4.005; 95% confidence interval: 2.011–7.975, p = 0.000), lack of information regarding immunization services (adjusted odds ratio = 2.493; 95% confidence interval: 1.293–4.809, p = 0.006), and maternal gravidity of ⩽3 (adjusted odds ratio = 4.198; 95% confidence interval: 1.425–12.370, p = 0.009) were significant factors for zero-dose vaccination. From the majority of in-depth interview participants’ expressions, myths and misinformation about vaccination, far distance from the health facility, and lack of convenient means of transport were important barriers for childhood vaccination.
Conclusion and recommendation:
This study revealed that the magnitude of zero-dose children is 17%, and demonstrated that zero-dose vaccination in Southwest Ethiopia is best understood through a multi-level ecological lens. While quantitative analysis identified antenatal care attendance, maternal knowledge/information, and gravidity as significant predictors, qualitative findings revealed how individual knowledge gaps, interpersonal influences, institutional service limitations, and broader structural barriers in underserved agrarian and pastoralist settings intersect to shape immunization behavior.
Introduction
Immunization is a vital, cost-effective intervention aimed at reducing mortality rates among children under-5, adolescent girls, and women worldwide. It is the most effective public health measure for preventing infectious diseases that are strongly associated with high morbidity and mortality. 1 It is estimated that every dollar invested in immunization yields a return on investment of ~$16. 2
A well-functioning immunization system relies on the interaction of several components, including careful planning and management of human, financial, and logistical resources; effective communication strategies; quality service delivery; maintenance of high-quality vaccine-preventable disease surveillance; and program-level monitoring and evaluation. In addition, policy support, global collaboration, and emergency preparedness are essential for its success.1,3,4 According to the Immunization Agenda 2030, the vision for the decade of vaccines is to enhance health and ensure that no one is left behind, so that everyone, in any situation or at any stage of life, receives the full benefits of immunization. 5 Since the inception of the national immunization program in Ethiopia in 1980, significant achievements have been made in reducing morbidity and mortality associated with vaccine-preventable diseases. 6 Ethiopia’s immunization system has been improved to adopt a life course and integration approach. The country accepted the Global Action for Vaccines and Immunization (Gavi’s) new global movement aimed at reducing the number of zero-dose children by 25% by 2025 and 50% by 2030, and developed an accelerated catch-up plan as part of this initiative. 2 The Gavi defines zero-dose children as those who have not received the first dose of the pentavalent vaccine (Penta-1). Despite this, the system faces multifaceted problems ranging from policy frameworks to community perceptions at the recipient level.7–12
In spite of significant progress in global immunization efforts, about 12.4 million children worldwide still miss basic, routine vaccines annually. In 2022, 12.4 million of the 72.5 million children targeted by Gavi in lower-income countries did not receive a single vaccine dose, leaving them vulnerable to life-threatening diseases. 13 This significant gap in coverage and equity has resulted in frequent vaccine-preventable outbreaks and numerous preventable deaths worldwide.14,15
Studies show that most vaccine-preventable deaths occur in low- and middle-income countries, which account for more than 69% of global zero-dose vaccination and 67% of deaths associated with vaccine-preventable diseases. 16 Another study shows that in 2021, there were 18.2 million children who received no vaccine doses. Therefore, vaccinating these zero-dose children is crucial to achieving the ambitious immunization coverage goals set for 2030. 17
In Ethiopia, despite significant improvements in immunization coverage over the years, the immunization program has recently been negatively affected by the COVID-19 pandemic, political instability, recent conflicts, political reforms, climate change, and other emergencies, all of which have directly or indirectly impacted the delivery of basic health care services, including immunization. 18 According to the World Health Organization/United Nations Children’s Fund 2022 Estimates of National Immunization Coverage, only 65% of the eligible target population received the first dose of Penta-1, and 70% received the first dose of measles-containing vaccine 1 (MCV1). As a result of these challenges, Ethiopia has about 1,146,000 zero-dose children, making it the second largest host of zero-dose children after Nigeria. 19 To address these significant gaps, some studies have identified several key factors, including limited economic resources, disenfranchisement of women, single motherhood, young maternal age, travel time to health facilities, maternal knowledge, type of residency, postnatal household visits, and insufficient use of antenatal and postnatal care services. However, none of these studies have focused on populations in underserved and unique settings, such as agrarian and pastoralist communities. Therefore, to develop customized interventions, this study aimed to identify the prevalence and associated factors of zero-dose vaccination and to explore possible barriers among children under the age of 2 years.
Patients and methods
Study design and settings
From August to September 2024, an explanatory sequential mixed-method design was used to analyze the prevalence of zero-dose children and associated factors, as well as immunization obstacles in the Southwest Ethiopia region. A community-based cross-sectional study was utilized for the quantitative component, while a qualitative descriptive technique with in-depth interviews was applied to evaluate the barriers to vaccination among caregivers of zero-dose children. The region is among the twelve with the lowest economic growth. It serves as a residence for 16 tribes, showcasing remarkable cultural diversity and Afro-traditionalism. This Region includes towns such as Teppi, Bonga, Tercha, and Mizan Aman, with most people being agro-pastoralists. It faces scarce resources, particularly in health care and education. The study involved all mothers/caregivers and children under 2 years old in selected enumeration areas.
Eligibility criteria: Inclusion criteria and exclusion criteria
For the qualitative component, mothers or caregivers and their children aged <2 years in the selected enumeration areas were included in the study. However, mothers or caregivers and their children aged <45 days were excluded since they could not take Penta-1 before this age. In addition, mothers or caregivers who had severely ill children were excluded from this study.
Sample size and sampling procedure
For the quantitative study, secondary data of 796 participants were collected from the Ministry of Health (MOH) in Ethiopia, specifically from Southwest Ethiopia, involving 21 rural and six urban areas across four zones: Bench Sheko, Dawro, Kaffa, and West Omo. To enhance the quantitative findings, qualitative data were obtained from Kaffa and Bench Sheko zones, with focus on Mizan Aman town, Tello, and Meint Shaha Woreda to reflect urban, agrarian, and pastoralist settings, respectively. Interviews were conducted among purposively selected mothers, distributed in Mizan Aman, Tello, and Menit Shasha, while the Dawro zone was excluded from this aspect due to the low proportion of zero-dose vaccinated children (Supplementary File 1). Data were saturated after interviewing 15 mothers, distributed as six from Mizan Aman, seven from Tello, and two from Menit Shasha.
Data collection tool and procedure
For the quantitative component, pre-collected and stored data were obtained from the MOH of Ethiopia. Even though we did not develop a tool for quantitative data collection, nor pilot test and collect data by ourselves, the ministry collected the data using a validated tool. 20
For qualitative data, an already developed and used in-depth interview guide 20 was adopted. Three female health extension workers were recruited to effectively collect the required information, and a key informant interview guide was used to conduct a one-to-one interview at home. Data collectors better understand the local language, culture, and overall context, and the in-depth interview guide was pilot tested. Fifteen, single-phase, face-to-face, in-depth interviews (30–45 min each) were conducted among mothers of zero-dose children in urban, agrarian, and pastoralist settings, and none of them refused to participate. The interview was conducted in the local language and audio-recorded with consent. The interviews explored knowledge and perceptions of immunization, experiences with antenatal and vaccination services, barriers to vaccination, and beliefs related to childhood vaccination. Field notes captured contextual observations and non-verbal cues.
Data quality control
The quality of quantitative data was trusted since the source of the data is the Federal MOH. Moreover the quality of the data was assessed for errors, outliers, and missing values.
For the qualitative part of the study, we took several steps to ensure the data were reliable and trustworthy. Data collectors were trained before starting, and the investigator regularly checked in to provide guidance and support. We strengthened the rigor of our process by carefully probing during interviews, cross-checking field notes with audio recordings, and discussing findings with peers. All interviews were transcribed word-for-word, and we used ATLAS.ti 8 software (qualitative data analysis software for windows and macOS) for systematic coding, keeping a clear record of all coding decisions along the way.
Study variables
The dependent variable was the prevalence of zero-dose children (yes = not vaccinated for Penta-1 and no = vaccinated for Penta-1). Penta-1 vaccination was considered a proxy for zero-dose children for different reasons. First, it is the first routine vaccine given in the health facilities with an appointment, unlike some birth dose vaccines (Bacille Calmette Guerin, polio birth dose). Second, it is standardized and globally reported.
Independent variables: were sociodemographic characteristics such as age, gender, income, family size, education of parents, health system factors, such as vaccine supply, service delivery methods, and availability and accessibility of vaccination services; and household factors such as fear of side effects, misconceptions, or rumors.
Definitions terms
Accessibility of vaccination services: -refers to the extent to which individuals and communities can easily obtain and utilize immunization services. According to the Ethiopian immunization guide, this variable can be measured by the Penta-1 rate. 21
Availability of vaccination services: means having sufficient vaccines and the necessary infrastructure (cold chain equipment, trained manpower) to provide immunization services. 21
Zero-dose vaccinated children are those children who have not been vaccinated for Penta-1. For operational purposes, Gavi defines zero-dose children as those who lack the Penta-1. 17
Ethical clearance
An ethical clearance letter was obtained from GAMBY Medical and Business College, and this letter was provided to the MOH and the Southwest Ethiopia regional health bureau. During qualitative data collection, all interviewees were informed regarding the scope, purpose, and anticipated outcome of the study. Then, written informed consent was obtained from legally authorized representatives of the minor subjects. In addition, written informed consent was obtained directly from mothers/caregivers who participated in interviews. Throughout the interview, confidentiality and anonymity were maintained, and this research adhered to ethical principles stipulated in the Helsinki Declaration of research in human subjects.
Data analysis
The quantitative data taken from the MOH of Ethiopia were exported to SPSS (Statistical Package for Social sciences) version 27.1 for cleaning and analysis. Descriptive statistics for categorical variables were presented in the form of frequencies and percentages, and means and standard deviations were used to describe continuous variables. The dependent variable (Penta-1 vaccination status) was dichotomized into “not vaccinated for Penta-1” or “vaccinated for Penta-1.” Then, a bivariate logistic regression analysis was performed for each independent variable with the dependent variable to select an eligible variable for the multivariable logistic regression analysis. Finally, an adjusted odds ratio (AOR) with 95% confidence interval (CI) was used to identify associated factors for zero-dose vaccination, and p < 0.05 was used to declare statistical significance.
Our qualitative analysis was guided by the social ecological model (SEM), 22 which helped us look at factors influencing zero-dose vaccination on multiple levels. At the individual level, we considered mothers’ knowledge, beliefs, and myths. At the community level, we explored the impact of misinformation. Institutional factors included vaccine availability and waiting times, while structural factors encompassed distance to health facilities, transportation challenges, and limited health system resources. We used reflexive thematic analysis because it allows us to stay close to participants’ own stories while also uncovering deeper, underlying reasons behind the barriers to vaccination.
After each in-depth interview session, the principal investigator transcribed each audio record verbatim in the language of the interview concurrently after each interview with repeated listening. Then, the transcribed interview was translated into English by an individual who is an expert in both English and local languages. Based on the empirical data, inductive coding was performed. After that, the principal investigator reviewed the transcripts line by line several times. Thereafter, texts were broken down into meaningful units, which were key phrases in the text. Subsequently, meaningful units were condensed and labeled with codes. ATLAS.ti8 software was employed to aid the coding process. The codes, according to similarities and differences, were allocated into seven sub-themes. Similar subthemes were grouped into Themes. Finally, the themes were determined as the expression of the latent meaning of the text.
Result
Sociodemographic characteristics
The result is written based on the quantitative data from 796 participants and the qualitative data from fifteen in-depth interview participants (IIPs). The sociodemographic features of IIPs are presented with table (Supplementary File 2). From the IIPs, important concepts were identified and organized into 13 codes based on the interview. Conceptually similar codes are further organized into seven subthemes and three themes. Theme I: knowledge and information about vaccines. Theme II: Health facility accessibility. Theme III: Service dissatisfaction, and it is written by triangulation with quantitative findings (Table 1).
Shows barrier that may influence childhood vaccination uptake in the Southwest Ethiopia region.

The quantitative data revealed that the majority of caregivers were Orthodox Christians (68.8%), followed by Protestants (19.8%). Most were married (96.2%), and a large proportion was unable to read and write (80.2%). Regarding the occupational status of mothers, housewives represented the primary occupation (76.9%), and the majority (80.2%) of mothers were unable to read and write. Reports from the qualitative study also support the maternal information gap, as most participants reported a lack of information as a barrier to vaccination.
Reproductive history and immunization service-related characteristics
In this study, a significant proportion of children were either the first, second, or third child in the family (85.8%). Most mothers had ⩽3 pregnancies (92.6%) and about 78.6% of mothers had antenatal care (ANC) visits; only 0.6% completed four visits. The number of deliveries at health facilities and at home were almost the same, which accounted 52.0% and 48.0%, respectively, and nearly one-third (33.3%) of mothers did not have postnatal visits at all. Distance to health facilities was also reported as it is a barrier for many mothers, with 49.5% reporting it as “too far.” This finding aligns with maternal expressions of different barriers to child vaccination during in-depth interview sessions. For instance, some participants stated, “I cannot tell you about the distance of the health center from my home; it is about 4–5 h walking distance; do you believe, an early postnatal woman with her newborn can cross such a walking distance with ease?”(P1) and “Leave it convenient ways of transport for a newborn (ደም ልጅ); even, a lorry is not accessible in our Kebele, especially in the summer season” (P13). On the other hand, waiting times were “too long” for 59.5% of respondents, while 25% experienced adverse effects on their child (Table 2).
Reproductive history and immunization service among mothers/caregivers of children under the age of 2 years, Southwest Ethiopia region (Bench Sheko, Dawro, Kaffa, West Omo), 2024/2025.
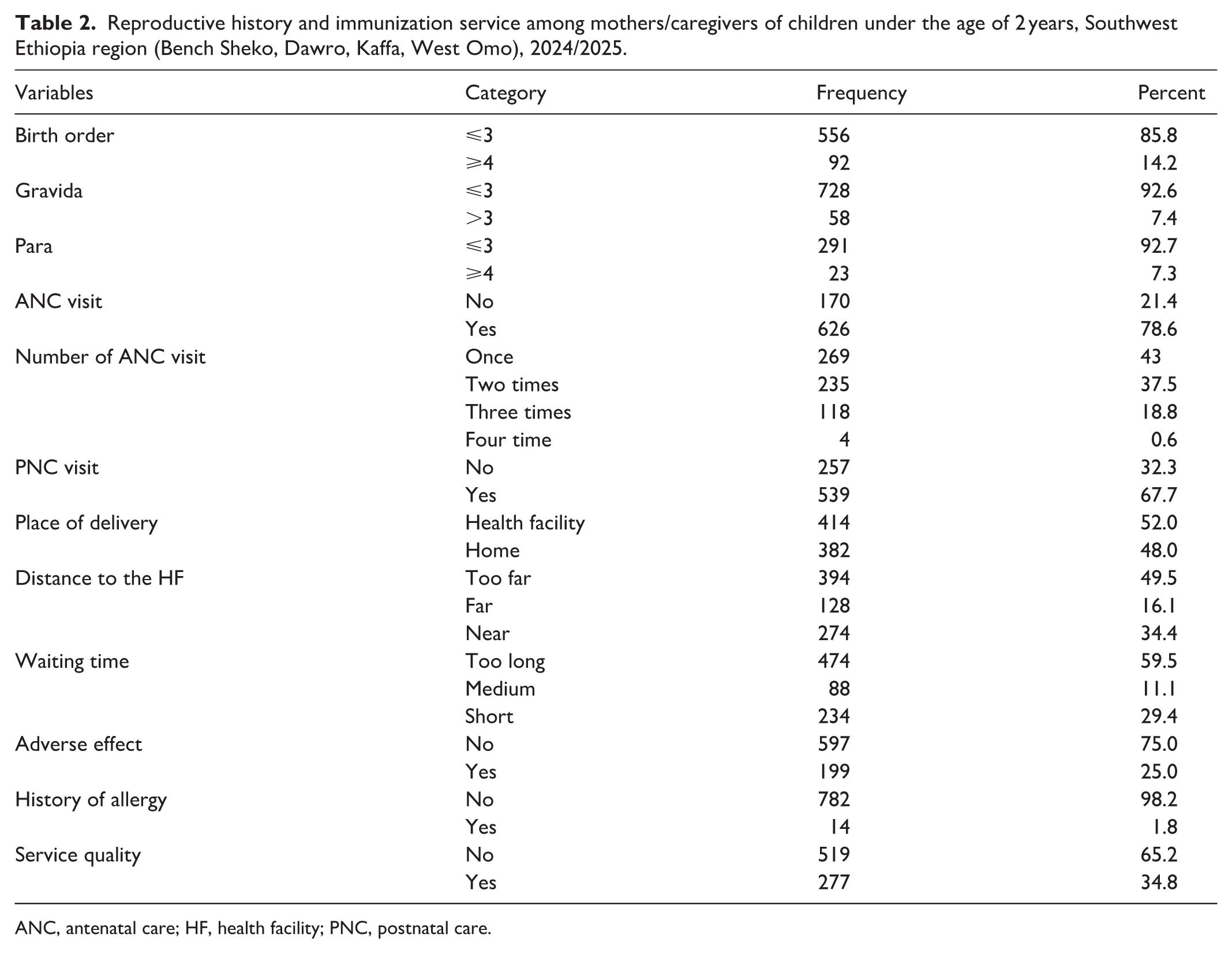
ANC, antenatal care; HF, health facility; PNC, postnatal care.
Information sources about the vaccine and service satisfaction
In this study, the majority, 638 (80.2%) of respondents had information about vaccines. Among those who have information regarding the vaccines, friends were the primary source, accounting for 634, followed by text message. However, Women Development Army, information, education, and communication, and community leaders were the three least common information sources, and recorded to be 16, 25, and 58 respondents, respectively. In this study, only 35.1% of respondents were very satisfied with vaccination services, while 29.0% were not satisfied at all. Dissatisfaction stemmed from vaccine unavailability (14.2%), delayed service unit opening (35.4%), long waiting time (28.6%), and unclean facilities (34.0%). This quantitative report is aligned with maternal expressions during in-depth interviews on service dissatisfaction. All IIPs reported the problem of unavailability of vaccine as well as health extension workers in place, and long waiting time for other infants to open some vaccine vials in their vaccination schedule. For instance, some IIPs expressed that “health extension workers were not available in place even though I went to health post early on my appointment date” (P6); and “after walking a 2 h distance, I have arrived at health post early in the morning to return back home fast for farming; but, the health extension worker was waiting other children to open vaccine vial. This was disgusting” (P11).
Moreover, from the quantitative data lack of adequate information (44.2%) and disrespectful staff (60.3%) were also notable issues. This lack of appropriate information regarding vaccination is deeply investigated through maternal expressions during in-depth interviews. During the interview, maternal expressions regarding the vaccine were related to misinformation and myths. For instance, one IPP stated that “I heard about vaccination in community gatherings from health extension workers, but, I didn’t know anything about the advantage and disadvantages of taking the child for vaccination” (P1), while another stated that “I prefer to be at home with my little baby for at least a couple of months; I am afraid of gathering places of people; my little baby will get sick when people see him” (P8).
Vaccination status and antigens received
According to this study finding, high coverage was noted for oral polio vaccine 0 (OPV0; 85.8%) and OPV1 (85.1%), while lower coverage rates were seen for MCV2 (75.6%) and MCV1 (72.9%). In addition, completion rates for specific vaccines varied, with Rota2 (77.3%) and pneumococcal vaccine 3 (76.0%) showing significant uptake differences (Table 3). The results indicate that about 17.0% (95% CI: 14.4%–19.8%) of children did not receive the Penta-1, while only 64.3% (512) of children received the Penta-2 vaccine (Figure 1). This trend suggests a drop-off in vaccine uptake as the schedule progresses, highlighting potential barriers to completing the vaccination series after the first dose.
Vaccination status and antigens received by children under the age of 2 years at the Southwest Ethiopia region (Bench Sheko, Dawro, Kaffa, and West Omo), 2024/2025.

BCG: Bacille Calmette Guerin; IPV: injectable polio vaccine; MCV: measles-containing vaccine; OPV: oral polio vaccine; PCV: pneumococcal vaccine.

The prevalence of Penta-1 versus Penta-2 vaccination among children aged of under 2 years in the Southwest Ethiopia region, 2024/2025.
Factors associated with zero-dose vaccination among children under the age of 2 years
About 15 independent variables fitted the binary logistic regression model, and all of them are adjusted to identify determinant factors of zero-dose vaccination among children. Finally, only three variables, such as lack of ANC visit, lack of information regarding immunization services, and maternal gravidity of ⩽3 were significantly associated with zero-dose vaccination (p < 0.05). Mothers who did not attend ANC were four times more likely to have zero-dose vaccinated children compared to those who attended it (AOR = 4.01, 95% CI: 2.01–7.98, p = 0.01). This strong association is justified since ANC is a gateway platform linking mothers to preventive health services, including immunization education. However, this important service is halted by the far distance of the health facility and the lack of convenient means of transport to the health facility, as the majority of IIPs explained.
Similarly, mothers who didn’t hear about the vaccination/those who didn’t have information about vaccination) were 2.49 times more likely to have zero-dose vaccinated children compared to their counterparts (AOR = 2.49, 95% CI: 1.29–4.81, p = 0.01). This association is supported by the presence of myths and misinformation identified in interviews (e.g. reliance on divine protection and fear of neonatal exposure to evil eye). From the majority of IIPs expressions, myths and misinformation were important barriers to childhood vaccination.
This study also noted that mothers who experienced ⩽3 pregnancies were 4.2 times more likely to have zero-dose vaccinated children compared to those mothers with experience of more than three pregnancies (AOR = 4.2, 95% CI: 1.43–12.37, p = 0.01; Table 4).
Determinant factors of zero-dose vaccine among children under the age of 2 years at the Southwest Ethiopia region, 2024/2025.

ANC: antenatal care; AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio; HF: health facility; PNC: postnatal care.
Discussion
The primary aim of this study was to estimate the prevalence of zero-dose vaccination and to identify determinants and barriers among children under the age of 2 years in Southwest Ethiopia. This study found that 17.0% (14.4%–19.8%) of children did not receive the Penta-1. Although the prevalence we found is lower than some national and regional estimates, it is still concerning, especially given the global commitment to reduce the number of zero-dose children by 25% by 2025 and by 50% by 2030. 17 Even modest levels remain significant when measured against these ambitious targets. Our findings also reflect broader global vaccination patterns reported by Global Burden of Disease (GBD) 2023, which show that while progress in routine childhood immunization has been made overall, it has been delayed in several low-income and conflict-affected settings. 23 This quantitative finding is consistent with a large-scale descriptive study in 33 sub-Saharan countries, 24 and the Ethiopian Demographic Health, 2019 survey report, with an overall prevalence of 19%. 25
When compared internationally, the 17% prevalence found in this study falls somewhere in the middle. It is higher than the combined estimates from multi-country studies that include higher-income countries, where immunization coverage tends to be stronger, 26 yet lower than estimates from conflict-affected contexts. 27 The discrepancy may be explained by the fact that conflict affects the availability and accessibility of child health services, including vaccination. This may increase the number of zero-dose children in these settings.
Similarly, the prevalence of zero-dose vaccination in this study was lower than that in another study conducted in underserved and special setting populations in Ethiopia, with a high prevalence of zero-dose vaccinated children (33.7%). 25 The possible justification for this huge difference in prevalence might be study time; with time variation, maternal knowledge and health-seeking behavior may be changed, resulting in lower zero-dose vaccination in this study.
The GBD 2019 and 2023 reports show that conflict-affected states have higher zero-dose burdens. Although Ethiopia faces resource challenges, the lower prevalence in this study suggests its immunization system remains partially functional, though access inequities persist.23,28 The persistence of zero-dose children highlights the ongoing burden of preventable infectious diseases in inequitable and weak health systems. Structural barriers—such as distance, poor infrastructure, and limited institutional capacity reduce ANC attendance and maternal knowledge, ultimately lowering immunization coverage. 28
Using the SEM as a guiding framework, the qualitative findings demonstrate that zero-dose vaccination is not solely an individual maternal decision, but the outcome of interacting influences operating at multiple ecological levels that reflect the combined effects of individual knowledge gaps, interpersonal influences, institutional service limitations, and broader structural barriers characteristic of underserved agrarian and pastoralist settings. At the individual level, inadequate maternal knowledge was strongly associated with zero-dose status. Mothers lacking sufficient vaccination information were 2.5 times more likely to have zero-dose children. While individual-level maternal awareness and knowledge of vaccine schedules directly influenced immunization decisions from the quantitative finding, qualitative expressions reveal that myths and misconceptions identified in interviews (e.g. reliance on divine protection, fear of neonatal exposure) reflect community-level normative influences regarding vaccination decisions (P1–3, P8).
This finding is in line with an umbrella review of systematic reviews conducted in Ethiopia 29 and the Democratic Republic of Congo. 27 This finding is also consistent with the growing body of literature linking information gaps and hesitancy to under-immunization, highlighting how misinformation, myths, and vaccine hesitancy, often amplified through informal community networks and digital platforms, contribute to zero-dose status globally. 30
Similarly, ANC attendance emerged as a critical determinant. Mothers who did not attend ANC were four times more likely to have zero-dose children compared to their counterparts. Narratives from the qualitative study revealed that geographical inaccessibility, transportation challenges, and poor road infrastructure limited ANC utilization.
Ecologically, ANC functions as an institutional gateway that connects mothers to preventive services, including immunization counseling, appointment scheduling, and trust-building with health providers. Most participants reported that difficulties of the road and unavailability of means of transport made ANC follow-up difficult; as a result, they did not get enough information about the vaccine and ended up with zero-dose vaccinated children (P7, P14). The possible reason for the association might be that mothers who did not attend their ANC follow-up regularly might not have higher health information/knowledge about the vaccine. As a result, their health-seeking behavior, including immunization service for their children, might be lower and end up with zero-dose vaccinated children. The study supports GBD 2019’s view that strengthening primary health systems is critical. Missing ANC visits limit access to immunization information and weakens connection to health services, increasing the risk of children becoming zero-dose. 28
Finally, the association between higher gravidity and improved vaccination uptake can be interpreted ecologically as cumulative exposure to health institutions. Mothers who experienced three or fewer pregnancies were more likely to have zero-dose children compared to those with four or more pregnancy experiences. Mothers with multiple pregnancies may have increased contact with health facilities across reproductive cycles, strengthening institutional familiarity and confidence for vaccination.
Although this issue was not explored in depth in the global studies we reviewed, our findings support the broader GBD perspective: when people stay connected to the health system over time, they are more likely to use preventive services.23,28
Interestingly, factors such as waiting time and overall satisfaction did not show a significant statistical effect in our multivariable analysis. However, our qualitative results told a different story. Many participants described poor service quality and logistical difficulties as real barriers that discouraged them from returning consistently. This highlights an important point also raised in GBD 2023: national coverage numbers can hide local service delivery problems. In other words, services may technically exist, but practical and contextual challenges can still prevent people from accessing them effectively. 23
Overall, our results are consistent with global evidence showing that zero-dose children are disproportionately found in structurally disadvantaged communities. Achieving the 2030 targets will require more than simply increasing coverage rates. As Nashwan and Abuhammad suggest, addressing misinformation is important. However, our findings make it clear that tackling misinformation alone is not enough. Transportation barriers, limited institutional access, and the need to better integrate immunization counseling into ANC services must also be addressed to create meaningful and sustainable progress. 30
Strengths of the study
This study finding has a number of strengths as stated below. This study utilized a substantial dataset from Ethiopia’s MOH Expanded Program of Immunization survey, covering 27 enumeration areas across four zones, ensuring representativeness and generalizability to the Southwest Ethiopia region. Utilizing this existing high-quality, nationally collected data enhances data accuracy and reliability while reducing data collection time and costs. In addition, the study combined quantitative and qualitative methods, allowing for triangulation and a comprehensive understanding of zero-dose prevalence, associated factors, and possible barriers. Finally, reflexive thematic analysis of qualitative data adds depth to the quantitative findings.
Limitations of the study
First, the cross-sectional nature of the quantitative study limits the ability to establish causal relationships between identified factors and the prevalence of zero-dose children. Second, the sample size for the quantitative study was not calculated; rather taken directly from the collected census data from the MOH. Third, some responses, particularly those related to immunization history and satisfaction with services, may be subject to recall bias, which may affect the data accuracy. Fourth, respondents may have underreported or overreported certain factors, such as vaccine uptake or healthcare accessibility, due to social expectations/social desirability bias. Fifth, this study primarily focuses on household-level factors; issues related to vaccine stockouts, logistics, and cold chain management at health facilities were not thoroughly explored. Finally, transcription and translation of qualitative data from local languages to English may have led to the loss of some nuances in meaning during data interpretation.
Conclusion
This study revealed that the magnitude of zero-dose children is 17%, and demonstrated that zero-dose vaccination in Southwest Ethiopia is best understood through a multilevel ecological lens. While quantitative analysis identified ANC attendance, maternal knowledge/information, and gravidity as significant predictors, qualitative findings revealed how individual knowledge gaps, interpersonal influences, institutional service limitations, and broader structural barriers in underserved agrarian and pastoralist settings intersect to shape immunization behavior.
Based on anchored findings within SEM, effective interventions must be multi-level:
At the individual level, maternal education and immunization literacy should be strengthened.
At the interpersonal and community level, religious leaders, elders, and community influencers should be engaged to address myths and mis-conception deep rooted in religion and culture.
At the institutional level, ANC integration with immunization service should be improved; waiting time should be reduced; and health worker and vaccine availability should be ensured.
The ecological lens also clarifies why zero-dose reduction strategies must incorporate geographic outreach, mobile clinics, and decentralized vaccination posts in pastoralist settings.
Supplemental Material
sj-docx-1-smo-10.1177_20503121261435048 – Supplemental material for Prevalence and its associated factors of zero-dose vaccination and barriers among children under the age of 2 years in Southwest Ethiopia: A mixed-method study
Supplemental material, sj-docx-1-smo-10.1177_20503121261435048 for Prevalence and its associated factors of zero-dose vaccination and barriers among children under the age of 2 years in Southwest Ethiopia: A mixed-method study by Fasika Tamirat and Mekonen Adimasu Kebede in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121261435048 – Supplemental material for Prevalence and its associated factors of zero-dose vaccination and barriers among children under the age of 2 years in Southwest Ethiopia: A mixed-method study
Supplemental material, sj-docx-2-smo-10.1177_20503121261435048 for Prevalence and its associated factors of zero-dose vaccination and barriers among children under the age of 2 years in Southwest Ethiopia: A mixed-method study by Fasika Tamirat and Mekonen Adimasu Kebede in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121261435048 – Supplemental material for Prevalence and its associated factors of zero-dose vaccination and barriers among children under the age of 2 years in Southwest Ethiopia: A mixed-method study
Supplemental material, sj-docx-3-smo-10.1177_20503121261435048 for Prevalence and its associated factors of zero-dose vaccination and barriers among children under the age of 2 years in Southwest Ethiopia: A mixed-method study by Fasika Tamirat and Mekonen Adimasu Kebede in SAGE Open Medicine
Supplemental Material
sj-docx-4-smo-10.1177_20503121261435048 – Supplemental material for Prevalence and its associated factors of zero-dose vaccination and barriers among children under the age of 2 years in Southwest Ethiopia: A mixed-method study
Supplemental material, sj-docx-4-smo-10.1177_20503121261435048 for Prevalence and its associated factors of zero-dose vaccination and barriers among children under the age of 2 years in Southwest Ethiopia: A mixed-method study by Fasika Tamirat and Mekonen Adimasu Kebede in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our thanks to GAMBY Medical and Business College for writing the ethical clearance letter for this study. We would like to extend our thanks to the Federal Ministry of Health, Ethiopia, for sharing quantitative data for other purposes. We would like to express our gratitude to the Regional, Zonal, Woreda, and Keble Level Administrators for facilitating the qualitative data collection process. Finally, we would like to give special thanks for data collectors and study participants.
Ethical considerations
An ethical clearance letter was obtained from GAMBY Medical and Business College, and this letter was provided to the Ministry of Health and the Southwest Ethiopia regional health bureau. During qualitative data collection, all interviewees were informed regarding the scope, purpose, and anticipated outcome of the study. Then, written informed consent was obtained from legally authorized representatives of the minor subjects. In addition, written informed consent was obtained directly from mothers/caregivers who participated in interviews. Throughout the interview, confidentiality and anonymity were maintained, and this research adhered to ethical principles stipulated in the Helsinki Declaration of research in human subjects (protocol no. REC-24-GMBC).
Author contributions
Fasika Tamirat conceptualized and designed the study; collected, analyzed, and interpreted the data. Mekonen Adimasu Kebede involved in designing and analyzing data; writing of the article and advising the entire research article. He also involved in the interpretation of the data and majorly contributed to article preparation. Both authors have read and approved the final article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data sets used and analyzed during the study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.