
Abstract
Background:
Since the introduction of the SARS-CoV-2 vaccine, the incidence of complications associated with pediatric infection has markedly declined. However, there is a notable decline in vaccination coverage among younger age groups. The objective of this study was to identify the factors associated with hesitancy to receive the SARS-CoV-2 vaccine in parents of children aged 3–15 years in a Latin American context.
Methods:
A cross-sectional, analytical study was conducted between February and May 2023. Parents of children between the ages of 3 and 15, residing in the metropolitan region of Chile, were surveyed via an online or in-person questionnaire. Univariate analysis and a multivariate logistic regression model were performed.
Results:
Five hundred thirty-nine surveys were completed; 61.6% of parents were aged between 21 and 40 years, 42.3% had completed higher education, 79.4% had paid employment, and 98.1% were fully vaccinated. Age distribution of children was 36.9% for 3–5 years, 42.4% for 6–11 years, and 20.8% for 12–15 years. 87.4% was vaccinated. In the univariate analysis, vaccine hesitancy was observed in 9%, associated mainly with children 3–5 years, fewer doses in parents’ vaccination schedule, lacking risk perception and concerns about safety, and not knowing where to access pediatric vaccine formulations against COVID-19. In the multivariate analysis, the younger age, lacking risk perception, and concerns about the vaccine’s effectiveness were associated with vaccine hesitancy.
Conclusion:
Addressing hesitancy toward COVID-19 vaccines is of utmost importance. Educational interventions should be implemented to inform parents about the importance and effectiveness of COVID-19 vaccination in children, with special emphasis on parents of younger children, to increase vaccination coverage.
Plain language summary
Background
- Vaccine hesitancy is considered a threat for the public health.
- SARS-CoV-2 vaccines have significantly impacted in the decrease of COVID-19 complications.
- Vaccination coverage among younger age groups has declined.
- This study aimed to identify factors contributing to vaccine hesitancy among parents of children aged 3 to 15 years in a Latin American context.
Methods:
- We conducted a cross-sectional study from February to May 2023.
- We surveyed parents of children aged 3 to 15 residing in the metropolitan region of Chile, using online and in-person questionnaires.
Results:
- Nine% of parents showed vaccine hesitancy, mainly associated with younger children, fewer doses in the parents’ vaccination schedule, lack of risk perception, and concerns about vaccine safety and efficacy.
Conclusions:
- Addressing vaccine hesitancy is crucial. Educational interventions should be implemented to inform parents about the importance, safety and effectiveness of COVID-19 vaccination in children, with a special focus on parents of younger children, to support the vaccination strategy.
Introduction
The COVID-19 pandemic has led to a global increase in morbidity and mortality throughout the world. 1 Initially, the infection primarily affected the adult population, with children under 5 years of age representing approximately 2% of the cases and 0.1% of deaths reported to the World Health Organization (WHO). 2 However, in the years 2021 and 2022, an increase in the impact on the pediatric population was observed. 3 Specifically, 2.5% of cases corresponded to children aged <5 years, while 10.5% were among those aged 5–14 years. 2 This highlights a higher mortality and morbidity rate in the group aged <5 years.2,4 Therefore, COVID-19 vaccination has become a global need. In the Americas, Chile ranked third in terms of the highest complete vaccination scheme per 100 people, 5 with a primary vaccination scheme coverage of 94.5% among those aged 3–17 years; however, this rate declined to 65.6% in children aged 3–5 years. 6 This decrease in vaccination coverage has prompted concerns about the public health implications and the need to investigate the phenomenon of vaccine hesitancy, which is defined as a delay in accepting or refusing vaccination despite the availability of vaccination services. 7
In 2019, the WHO considered vaccine hesitancy a threat to global health. 8 It is influenced by three factors: confidence, complacency, and convenience, which can be presented individually or in combination. 7 Confidence is determined by the efficacy and safety of the vaccine as well as trust in healthcare professionals and the vaccination system. 7 Complacency depends on the perception of the risks and benefits of vaccination in preventing diseases and may be affected by individual responsibilities when seeking vaccination. Finally, convenience is based on the physical and geographical availability of the vaccine as well as its accessibility to the general population. 7
Globally, numerous studies have been conducted to assess parents’ perceptions of the SARS-CoV-2 vaccination. Concerns about the safety and the occurrence of adverse events following immunizations (AEFI), and distrust in the development and approval processes are factors that can potentially influence hesitancy.9–14 In Chile, there is a lack of information about parents’ hesitancy and the factors influencing pediatric SARS-CoV-2 vaccination. Identifying the underlying factors that contribute to hesitancy is crucial for designing effective interventions that promote vaccine acceptance and ensure optimal vaccination coverage in this age group. This study aimed to determine the main factors associated with COVID-19 vaccine hesitancy among parents of children and adolescents aged 3–15 years in the Chilean metropolitan region.
Materials and methods
In Chile, the vaccination campaign against COVID-19 commenced on December 25, 2020, initially targeting adults with preexisting medical conditions and those at high risk of exposure. Subsequently, the program was expanded to include younger age groups, including adolescents in June 2021, and children aged 6–11 and 3–5 years in September 2021 and December 2021, respectively.4,15,16 The COVID-19 mass vaccination campaign delivered more than 24 million doses in almost 6 months, reaching 63% of the total population, and was recognized as one of the most successful COVID-19 vaccination campaigns worldwide.15,17 A variety of vaccine platforms were employed, including messenger RNA (mRNA), inactivated, and viral vector vaccines for adults; mRNA and inactivated vaccines for adolescents; and solely inactivated formulations for young children. All doses were offered free of charge and electronically registered in the National Immunization Program records. Despite vaccination being non-mandatory, the average uptake was higher for adults (92.7%) and children aged 6–17 (90%) than for those aged 3–5 years (63%).15–17
An analytical cross-sectional study was conducted by surveying parents of children and adolescents aged between 3 and 15 years in the metropolitan region of Chile. The study participants were recruited between February 1 and May 20, 2023, using a hybrid methodology. For participants who responded to the online survey, a snowballing technique was employed, whereby the invitation to participate was disseminated through social networks such as Facebook, WhatsApp, and Instagram. Furthermore, the survey was administered to parents and guardians in the medical-surgical hospital wards and outpatient consultations at the Dr. Exequiel González Cortés Children’s Hospital (HEGC) in the face-to-face modality.
The inclusion criteria were established for parents of children and adolescents between 3 and 15 years of age, residing in the Chilean metropolitan region, and who gave informed consent to participate. In situations where the parents were responsible for several children or adolescents, they were asked to respond to only one of them parents who did not provide consent or incomplete surveys were excluded. This study was approved by the South Metropolitan Health Service Ethical Committee (approval no. 014/2023) on February 7, 2023.
To determine the sample size, a minimum of 10 subjects was recruited per questionnaire item. Given that the questionnaire consisted of 35 questions, a sample size of 350 subjects was estimated; considering a 50% rejection rate, a sample size of 525 participants was calculated. The questionnaire (Supplemental Material) was designed using Google Forms and included questions on sociodemographic characteristics, the immunization status of the parents and the child or adolescent, the possibility of annual COVID-19 vaccination, perception of importance, safety, effectiveness, and concern about AEFI as well as aspects related to vaccination (location, access, waiting time, vaccination clinic hours, and vaccine availability), knowledge about vaccines, information sources, a confidence scale, and positive attitudes toward vaccines, based on a survey of factors influencing vaccination delay in Chile. 18 Participants who responded online were recruited using the “snowball” technique through social networks Facebook, WhatsApp, and Instagram. In addition, the survey was administered to parents in the medical-surgical hospitalization wards and clinics of HEGC.
The dependent variable “COVID-19 vaccination hesitancy” was defined according to the responses of parents who reported not having vaccinated their child or adolescent under their care. The independent variables included the sociodemographic characteristics of both parents and children or adolescents. In addition, aspects such as perception of the COVID-19 vaccine, opinions about the vaccination system, and attitudes toward vaccines of the National Immunization Program (NIP) were evaluated.
Statistical analysis was performed using the RStudio Software (RStudio, Inc., Boston, MA, USA); a univariate analysis with the chi-square test (χ²) was conducted for each independent variable. Subsequently, we sought to ascertain the association between significant independent variables, for which an intervention could be implemented to increase adherence to the SARS-CoV-2 vaccine, with “COVID-19 vaccination hesitancy” by constructing a multivariate logistic regression model. The cutoff point for statistical significance was set at p < 0.05, with a 95% confidence interval (CI).
Results
A total of 540 parents were surveyed, of whom one did not provide consent to continue completing the survey. Of the remaining 539 surveys, 354 were completed online and 186 were completed in-person.
Parents characteristics
In all, 62% (n = 332) were aged between 21 and 40 years; 84.5% (n = 457) were women, with 82.2% (n = 443) being mothers. Ninety percent of the respondents reported being Chilean nationals, the majority (59.9%, n = 322) were married or in a civil union, and approximately 42.3% (n = 228) had completed higher education. In addition, the majority (79.4%, n = 428) had paid employment. Regarding personal COVID-19 vaccination status, 529 respondents (98.1%) were already fully vaccinated, of whom 59.9% had received four doses at the time of responding to the survey (Table 1).
Sociodemographic characteristics of parents, children, and adolescents aged 3–15 years, in the metropolitan region, Chile, 2023.

Characteristics of children and adolescents
A total of 96.3% (n = 519) of the children and adolescents were Chilean. In terms of age distribution, the cohort was comprised of 36.9% (n = 199) individuals between the ages of 3 and 5 years, 42.4% (n = 228) between the ages of 6 and 11 years, and 20.8% (n = 112) between the ages of 12 and 15 years. It was observed that 58.1% (n = 313) belonged to the private health system and 41.9% (n = 226) to the Public Health Services. In addition, 73.8% (n = 398) came from bi-parental families, 87.4% (n = 471) reported having at least one dose of vaccine for their child or adolescent, and of these, 40.6% (n = 191) had received three doses of the COVID-19 vaccine.
By contrast, 12.6% (n = 68) of the children were not vaccinated, 50% (n = 34) of the parents in this group, indicated that they did not wish to vaccinate them, 22.1% (n = 15) had not yet decided whether to vaccinate them, and 27.9% (n = 19) expressed their intention to vaccinate them but had not yet visited the vaccination center (Figure 1). None of the parents were unvaccinated against COVID-19, 1.9% (n = 10) had vaccinated the child or adolescent under their care, and 80% (n = 8) expressed a lack of interest in vaccination.
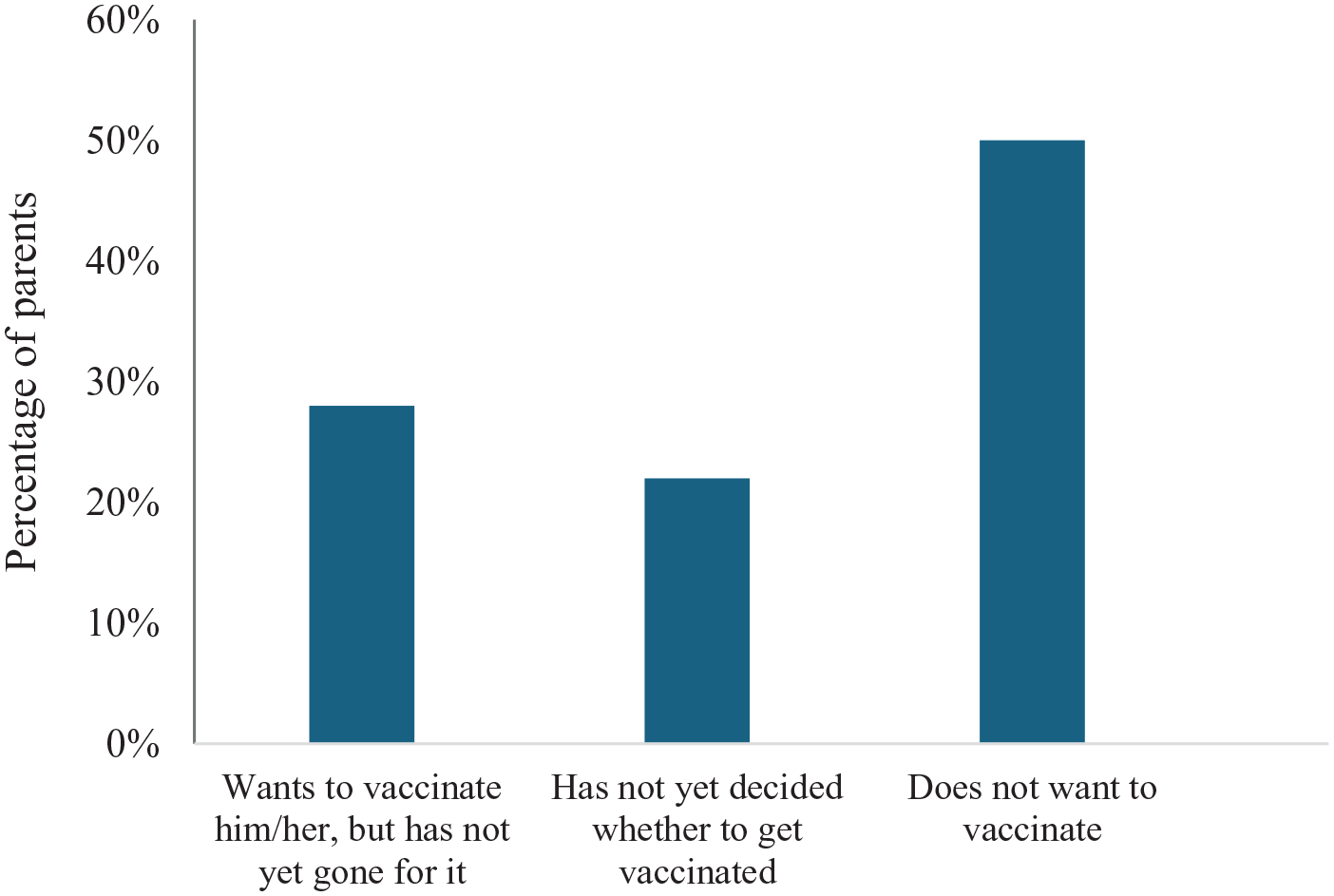
Reasons for not vaccinating children and adolescents aged 3–15 years against COVID-19, metropolitan region, Chile, 2023 (N = 68).
Univariate statistical analysis
Vaccine hesitancy was observed in 12.6% (n = 68) of the study sample. When analyzing the variables individually, it was found that certain parents had a higher probability of not being vaccinated. Among these factors, it was noted that parents aged between 21 and 40 years or older than 61 years (p < 0.05), as well as those whose marital status was divorced/separated/widowed (p < 0.05), lacked higher education or had only higher education without a postgraduate degree (p < 0.05), and were unemployed (p < 0.001) showed a significant increase in the probability of not vaccinating children or adolescents. In addition, it was observed that as the parents received fewer doses of the vaccine, and the probability of hesitancy increased (p < 0.001). Hesitancy was also associated with parents being in charge of children or adolescents in the public health sector (p < 0.001), and having children aged 3–5 years (p < 0.001). No statistically significant association was found between kinship between the parents and the child or adolescent, the gender of the parents, the nationality of both the parents and the child or adolescent, or the family structure in relation to vaccination.
Complacency has been identified as a factor associated with vaccine hesitancy. Parents who reported being little or not at all concerned about the possibility of contracting or re-contracting COVID-19 in children or adolescents had a higher probability of not vaccinating them (p < 0.05). 17.3% (n = 93) of parents indicated that they would not vaccinate their child or adolescent against COVID-19 annually and 59.1% (n = 55) stated that the main reason for not vaccinating was the perception that they were already sufficiently protected. In addition, 34.4% (n = 32) stated that they did not consider COVID-19 to be a fatal disease for their children. These factors were significantly associated with hesitancy (p < 0.001). Regarding the perception of the importance of the vaccine for health, it was observed that parents who considered it of little or no importance had a higher probability of not vaccinating. When analyzing the determinants of confidence, it was found that considering the vaccine to be little or not at all safe (p < 0.001) and being moderately or very concerned about possible severe reactions to the vaccine (p < 0.001) were associated with higher hesitancy. By contrast, parents who perceived the vaccine as effective were more likely to vaccinate children or adolescents under their care (p < 0.001). Regarding convenience, it was observed that not knowing where to access pediatric vaccine formulations against COVID-19 increased hesitancy (p < 0.05), while access to the vaccine, location, vaccination clinic hours, and waiting times did not show statistical significance.
Parents who used the Internet and social networks as a source of information for making vaccination decisions showed greater hesitancy than those who consulted health professionals or friends/family (p < 0.05). Regarding the confidence scale and positive attitudes toward vaccination in general, it was found that those parents who disagreed or had no clear opinion on the evaluation of NIP vaccines showed greater hesitancy toward COVID-19 vaccination (p < 0.05; Table 2).
Factors associated with vaccination against COVID-19 in parents of children and adolescents aged 3–15 years, in the metropolitan region, Chile, 2023 (N = 539).

Multivariate logistic regression model
In the logistic regression model, it was observed that the age of the child was the factor with the greatest influence on the probability of parental hesitancy; the older the age of the child, the less hesitancy to vaccinate (6–11 years, OR = 0.12, 95% CI = 0.05–0.26; 12–15 years, OR = 0.04, 95% CI = 0.01–0.17). Second, complacency was significant, as parents who perceived vaccination as important were associated with less vaccine hesitancy (OR = 0.10, 95% CI = 0.03–0.37). On the other hand, when a child or adolescent belonged to the public health system, there was a greater association with hesitancy (OR = 0.23, 95% CI = 0.12–0.47). Finally, trust also emerged as a factor associated with hesitancy, given the perceived effectiveness of the vaccine (OR = 0.29, 95% CI = 0.11–0.71; Table 3).
Factors associated with reluctance to vaccinate against COVID-19 in parents of children and adolescents aged 3–15 years, metropolitan region, Chile, 2023 (N = 539).

CI, confidence intervals; OR, odds ratio.
Discussion
The spread of COVID-19 increased global morbidity and mortality, extending to the pediatric population. This underscores the need for vaccination, which significantly reduces mortality worldwide and highlights the importance of adequate vaccination adherence. 19 In Chile, a successful centrally planned vaccination campaign at a national level against COVID-19 was implemented in December 2020. The campaign was based on prioritized risk conditions or age groups, with the vaccination program progressively decreasing in age.4,15 Although vaccination was not mandatory, the campaign administered more than 24 million doses in almost 6 months, representing 63% of the total population fully vaccinated by the end of the program, overall uptake of 92.7% had been achieved among individuals aged 18 years and above, 99% and 91% in the 12–17 and 6–11 age groups, respectively, and 63% was achieved in the 3–5 age group,15–17 raising concern and emphasizing the need to investigate vaccine hesitancy in the pediatric population.
Vaccine hesitancy exhibits considerable variation across different populations, with a global prevalence rate of 20.8% reported in Europe.20,21 In Asia, the range is more extensive, with rates oscillating between 20% and 60%.22–24 A comparable rate of hesitancy is evident in the United States, as demonstrated in the Ruggiero et al. study, which revealed a hesitancy rate of 21.9%. 25 In Latin America, the hesitancy rate is lower, with a study in Brazil reporting a 2.8%, 26 and another in Peru showing a vaccination intention of 83.5%. 14 However, higher hesitancy rates have also been reported, such as a study in Mexico that reported 14%. 27
In Chile, a higher percentage of vaccination coverage in children has been observed than in other countries in Latin America, Asia, Africa, and the Middle East. 28 Despite this, our study found a hesitancy rate of 12.6%. By identifying the factors associated with vaccine hesitancy, we found that younger parents with a lower level of education, and those who were unemployed, had higher hesitancy; associations were also evaluated in other series.9,13,21,28 By contrast, parents of younger children showed greater hesitancy compared to other age groups, which could explain the decrease in vaccination coverage, as indicated by data from the Ministry of Health, in line with other published studies.28,29 This trend may be related to the perception of greater vulnerability to serious adverse events at a younger age. 30
Vaccine confidence plays a crucial role; those who consider the vaccine unsafe or ineffective and are concerned about adverse effects are more likely to hesitate, as suggested by multiple studies.9,12,15,20–24,30–32 Nevertheless, it is important to note that after the start of the COVID-19 vaccination, surveillance of the safety of vaccines administered in Chile has been reinforced. 16 According to official reports on children AEFI at the national level, adverse events were extremely rare (0.01%), underscoring vaccine safety. 33 The effectiveness observed in various randomized clinical trials in reducing both the incidence and severity of multisystem inflammatory syndrome in children associated with COVID-19,4,34,35 has highlighted the importance of integrating the vaccine into the annual vaccination schedule. 36 We also observed that complacency was a fundamental influencing factor, as parents who were less concerned about the severity of the infection in children considered the vaccine unimportant or were sufficiently protected, as highlighted in other studies.12,30 However, this attitude can lead to a long-term decrease in vaccination coverage. In addition, we found that convenience was not an influencing factor in our study, suggesting that the physical and geographical availability of vaccines was not an issue in this setting.
It is important to acknowledge that hesitancy can pose a challenge to achieving optimal vaccination coverage in the pediatric population, particularly in younger children. This is evidenced by the fact that vaccination coverage between the ages of 6 months and 2 years is a mere 0.9% during the first 6 months of the implementation, as reported by the Immunization Department, at the Ministry of Health of Chile. 37 To address this issue, a comprehensive strategy that includes evidence-based and quality education directed at the general population. The implementation and execution of this initiative could be carried out by multidisciplinary teams, which would gather efforts from governmental institutions, healthcare professionals, and scientific societies, which play a crucial role in disseminating accurate information and building trust in vaccination.20,21,29 The aim of this strategy must be to achieving optimal coverage, including booster doses. As suggested in the report of the Chilean National Immunization Technical Advisory Group, efforts should be prioritized in age groups with lower vaccination coverage’. 38 In our study, we also identified that parents not vaccinated against COVID-19 showed a greater reluctance to vaccinate their children, a finding congruent with that described by Issanov et al. 39 who reported that adults with children were more likely to have reluctant attitudes toward vaccination. We therefore consider it essential to implement strategies specifically targeting adults with children, with an emphasis on parents of young children. These strategies should focus on promoting the importance of maintaining an up-to-date vaccination schedule.
The dissemination of this information, through scientific journals and the work of health professionals, has proven to be an effective strategy to reduce reluctance to vaccinate in the general population. 40 This effect is also reflected in the results of our study, which found that parents who consulted reliable sources, such as medical societies or health professionals, had significantly lower levels of reluctance toward vaccination. For this reason, a comprehensive educational approach could contribute to optimizing vaccination coverage, even beyond the age group analyzed in this study. This is particularly relevant when considering the need to vaccinate infants from 6 months of age.
The limitations of our study included its design, which allows for the establishment of associations but not causality between the factors; and the online dissemination of the survey, which could result in the under-reporting of data. Moreover, as COVID-19 vaccination behavior was assessed based on responses from 1 to 2 years ago, societal context and perceptions regarding vaccination might have evolved since then, especially those related to vaccination fatigue that has been reported from other countries. This temporal gap could influence participants’ responses and introduce potential bias. Finally, during the data collection of our study, we were not able to determine whether the parents or guardians of the children had participated in clinical trials or not. As previously stated, the administration of the SARS-CoV-2 vaccine is not obligatory in Chile, including for medical personnel and government employees. Consequently, these facts were not considered a potential source of bias in our study. While the representativeness of the sample could be improved, replicating this research on a larger scale would provide further insights.
In summary, our study revealed that COVID-19 vaccine hesitancy in the pediatric population of the Metropolitan Region of Chile could be influenced by a number of factors, including the parents’ age, educational level, employment status, number of vaccine doses received by the parents, the child’s age, their health insurance, and the parent’s perception of the vaccine’s importance, safety, and effectiveness.
Conclusion
It is of utmost importance to approach the hesitancy to vaccinate against COVID-19, considering the need to increase vaccination coverage in the pediatric population. Considering that the main factors associated with reluctance in our population were complacency and trust, it is necessary to educate parents and guardians about the importance of vaccine administration and its effectiveness, with special attention to parents of younger children.
Supplemental Material
sj-doc-1-tav-10.1177_25151355251322312 – Supplemental material for Parental hesitancy for pediatric COVID-19 vaccines in Chile
Supplemental material, sj-doc-1-tav-10.1177_25151355251322312 for Parental hesitancy for pediatric COVID-19 vaccines in Chile by Daisy Cedillo, María Jesús Godoy, Paula Leal and Rodolfo Villena in Therapeutic Advances in Vaccines and Immunotherapy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.