
Abstract
Background:
The risk of neonatal tetanus infection will be reduced when the pregnant woman takes two doses of the maternal tetanus toxoid vaccine. In Ethiopia, however, low immunization coverage levels, mostly due to missed opportunities, are a concern. The study’s main objective of the study was to assess tetanus toxoid immunization utilization coverage and associated factors among postnatal mothers in Debre Markos town, Ethiopia.
Materials and Methods:
A community-based cross-sectional study was conducted among 505 mothers who had given birth in the last 12 months. A two-stage stratified sampling technique was applied, and the The participants were selected using a systematic random sampling technique. Data were entered into EpiData manager version 4.6.0 and analyzed using Statistical Package for Social Science (SPSS) version 25 software. Bivariable and multivariable logistic regression analysis was performed. Adjusted odds ratios (AORs) at 95% CIs were used to identify factors associated with tetanus toxoid immunization utilization.
Results:
The total tetanus vaccine intake (TT+2) doses were 71.2% (95% CI: 67.4–76.2). Mothers who attended primary school (AOR: 0.07, 95% CI: (0.01–0.6)), mothers whose husbands had secondary education (AOR: 0.26, 95% CI: (0.08–0.84)), mothers who attended 2–3 times antenatal care (ANC) visit (AOR: 0.05, 95% CI: (0.01–0.3)), good quality service (AOR: 2.8, 95% CI: (1.05–7.5)), appropriate behavior of health workers (AOR: 6.2, 95% CI: (2.2–18.7)), and who visited health extension workers (AOR: 7.6, 95% CI: (2.3–25.3)) were significantly associated with TT vaccine utilization.
Conclusion:
Only three out of four pregnant women received the current TT vaccine during their previous pregnancy. The most influencing factors in TT vaccine utilization were the mother and her husband’s low educational level, 2–3 times ANC visits during pregnancy, the standard of healthcare service, the healthcare provider’s behavior, and the mother’s visits with health extension staff.
Plain language summary
Maternal and neonatal mortality is high both in developed and developing countries due to preventable infection. Tetanus is an acute bacterial infection caused by a highly potent neurotoxin that affects the mother and newborn during pregnancy, childbirth, and postnatal. World Health Organization recommended that women of childbearing age benefit from tetanus toxoid immunization. So, assessing tetanus toxoid immunization coverage and their associated factors will help the policy makers for the next planning. The study was employed in the community among 505 childbearing women and found that 71.2% of them were vaccinated with tetanus toxoid dose two (TT++). Even though the women and neonates in the community benefited from the vaccine, only 7.7% of them had cards. Almost 58.8% of the women reported that there was a gap in counseling about the tetanus toxoid vaccine purpose. In this study mother’s and husband’s educational status, number of Antenatal care visits, perceived quality of service, the behavior of health workers, traveling time to health facilities, and health extension are factors that affected tetanus toxoid vaccine coverage. Finally, the researchers in the area can use this finding as input and conduct further study including qualitative design to explore women’s experiences related to the tetanus toxoid vaccine.
Keywords
Introduction
Tetanus is an acute bacterial infection caused by a highly potent neurotoxin produced by the spore-forming gram-positive bacterium clostridium tetani. Tetanus is a highly fatal, noncommunicable, and toxin-mediated disease. 1 Globally, maternal and neonatal tetanus is a public health problem due to low maternal tetanus toxoid immunization. Mothers and newborns are at a high risk of acquiring tetanus during birth, where maternal tetanus infections are associated with unhygienic delivery procedures, abortion, and miscarriage.2,3 According to the World Health Organization (WHO) key facts, tetanus can be prevented through immunization with tetanus-toxoid-containing vaccines. However, people who recover from tetanus do not have natural immunity and can be infected again. Based on this fact, WHO recommended that women of childbearing age should begin a five-dose regimen of vaccination. The primary dose should be slender at any time in her reproductive age. The TT+2 dose is given 4 weeks apart and also the third dose is given at least 4 weeks apart and also the third dose is given at least 6 months after the second dose. 4 Maternal and Neonatal Tetanus Elimination (MNTE) strategies focused on reproductive-age women, and also supplementary immunization campaign activities’ implementation to vaccinate women aged 15–49 years with limited access to health services and effective surveillance in high-risk areas has been very successful. 5 In Africa and Southeast Asia most mothers and newborns die from tetanus because of poverty, weak medical infrastructure, or humanitarian crisis; mostly the poor women have no access to medical services and have little information about safe delivery methods and postnatal services. 6 The majority of the sub-Saharan African countries had faced difficulty in achieving the scope WHO Global TT immunization target set to achieve complete elimination of MNT at least 90% and 80% national and district vaccination utilization. 7 Most maternal problems occur due to lack of vaccination or incomplete immunization on exposure leading to an increase in morbidity and mortality. An estimated 15,000–30,000 women die from tetanus infection during or after delivery.8–10 The causality of tetanus among neonates is about 80%–100%, and it is still a significant public health concern in areas with poor immunization utilization and limited access to clean deliveries. 11 According to a 2018 WHO report, around 25,000 newborns died due to neonatal tetanus (NT) and it mostly occurs in remote communities and areas underserved by healthcare system frameworks. Africa has the most elevated MNT deaths, which averages 110,000 in a year and accounts for 90% of global NT cases. 12 For a long period Ethiopia has had the highest neonatal mortality and morbidity related to tetanus due to low tetanus toxoid immunization and the high number of home deliveries. Maternal and NT are preventable with proper implementation of TT vaccine immunization strategy which needs special attention. 13 Ethiopia is one of the sub-Saharan countries and still has low TT vaccine utilization coverage as per the 2016 Ethiopian Demographic Health Survey report that indicated only 49% of newborns were protected at birth. 14 The magnitude magnified in Amhara Region is that only 36% of reproductive-age women have got TT2 and above immunization. 15 Therefore, this study aimed to assess TT vaccine coverage and associated factors among reproductive-age women in Debre Markos town, Ethiopia.
Materials and methods
The study was conducted in Debre Markos town. A community-based cross-sectional study design was used from February 8 to March 8, 2021. Debre Markos has one referral hospital, three health centers, seven health posts, and five nongovernmental clinics, which provide different reproductive health services in the town.
All reproductive-age women (15–49 years) in Debre Markos town were the source population and women who gave birth in the last 12 months in the selected kebeles and were available during the data collection were the study population.
Women of reproductive age who had at least one child in the last 12 months were included, and women who had a mental problem, were unable to hear, and were not available at home during the survey were excluded. The sample size was calculated using a single population proportion formula and Epi InfoTM7 version 7.1 Stat Calc with the following assumptions: 95% confidence interval, 5% margin of error; and 72.5% of the mothers who received at least two TT doses were taken from the study result in Southern Region. 16 The sample size for the second objective was calculated using the Epi InfoTM7 version 7.1 Stat calc function. This Epi InfoTM7 version 7.1 is a Center for Disease Control and Prevention based in the USA. The formula that yields the highest number was taken to calculate the final sample size. Considering the design effect of 1.5% and 10% nonresponse rate, the final sample size was 505. Two-stage stratified sampling technique was applied in the study. From 11 kebeles, 4 were selected with a simple random sampling method. Then to select 505 participants from selected kebeles, all the kebeles listed down their respective mothers who delivered in the last year and allocated proportionally from 738. Finally, participants were selected using systematic random sampling.
Data collection technique
Data were collected with interviewer-administered and pretested structured questionnaires. The questionnaire was adapted from the study conducted in the Northern part of Ethiopia with some modifications. 3 The questionnaire included sociodemographic, obstetric, and health service-related determinants and questions on TT immunization. Four trained data collectors (health extension workers) through a face-to-face interview collected data. Training and orientation for data collectors and supervisors about the purpose of the study and the procedure of data collection were given for 2 days.
Data quality assurance
The adapted questionnaire was originally prepared in English, then it was translated into the local language and retranslated into English by language experts to ensure consistency. Every day during the data collection period, completed questionnaires were reviewed for accuracy. Five percent of the sample in the nonselected area participated in the pretest.
Data analysis methods
Collected data were entered into EpiData manager version 4.6.0 and were exported to SPSS version 25 software for further analysis. By using descriptive statistics, data were summarized as frequencies and percentages and were visualized using tables and charts. In the bivariable analysis, variables with p < 0.25 were included in the multivariable analysis. In the multivariable logistic regression, adjusted odds ratios (AORs) at 95% CIs were used to predict factors associated with TT utilization, and variables with p < 0.05 were considered statistically significant.
Results
Sociodemographic characteristics
A total of 505 women who delivered in the last 12 months before the survey were interviewed face-to-face giving a 100% response rate. Most (92.7%) of the participants were married and the majority (86.5%) of them were orthodox religious followers (Table 1).
Sociodemographic characteristics of study participants in Debre Markos town, Ethiopia, 2021 (N = 505).

Housewife, private employee, student.
ETB, Ethiopian Birr.
Obstetric and health service-related characteristics
More than half of the participants (56.4%) had given birth to 2–3 children during their lifetime. The majority (97.8%) of the participants had at least one ANC visit in the last pregnancy and about 92.3% of participants had visited health extension workers during their pregnancy (Table 2).
Tetanus toxoid vaccine coverage related to obstetric and health service factors among postpartum women in Debre Markos town, Ethiopia, 2021 (N = 505).

ANC, antenatal care; HW, health worker.
Tetanus toxoid vaccine utilization
Based on the mother’s vaccination card and oral history, 322 (71.2%) mothers received legitimate tetanus vaccinations during their previous pregnancies. More than half (59.2%) of the vaccination status was confirmed through oral history, and only 7.7% of participants had vaccination cards (Table 3).
TT vaccination utilization characteristics of mothers who gave birth in the last 12 months in Debre Markos town, Ethiopia, 2021 (N = 505).

Reasons for not getting the valid TT + ² vaccine
For about 58.8% of participants, the most common reason for not getting or starting the vaccine was nobody advised them about the importance of the TT vaccine (as shown in Figure 1).

Reasons explained by mothers for not starting TT vaccine in Debre Markos town, North-West Ethiopia, 2021.
Distribution of each TT vaccine
Of the participants, 71.2% of women were immunized with more than two TT doses in the last pregnancy (Figure 2).

Tetanus toxoid vaccine utilization status in Debre Markos town, North-West Ethiopia, 2021.
Factors associated with tetanus toxoid vaccine utilization
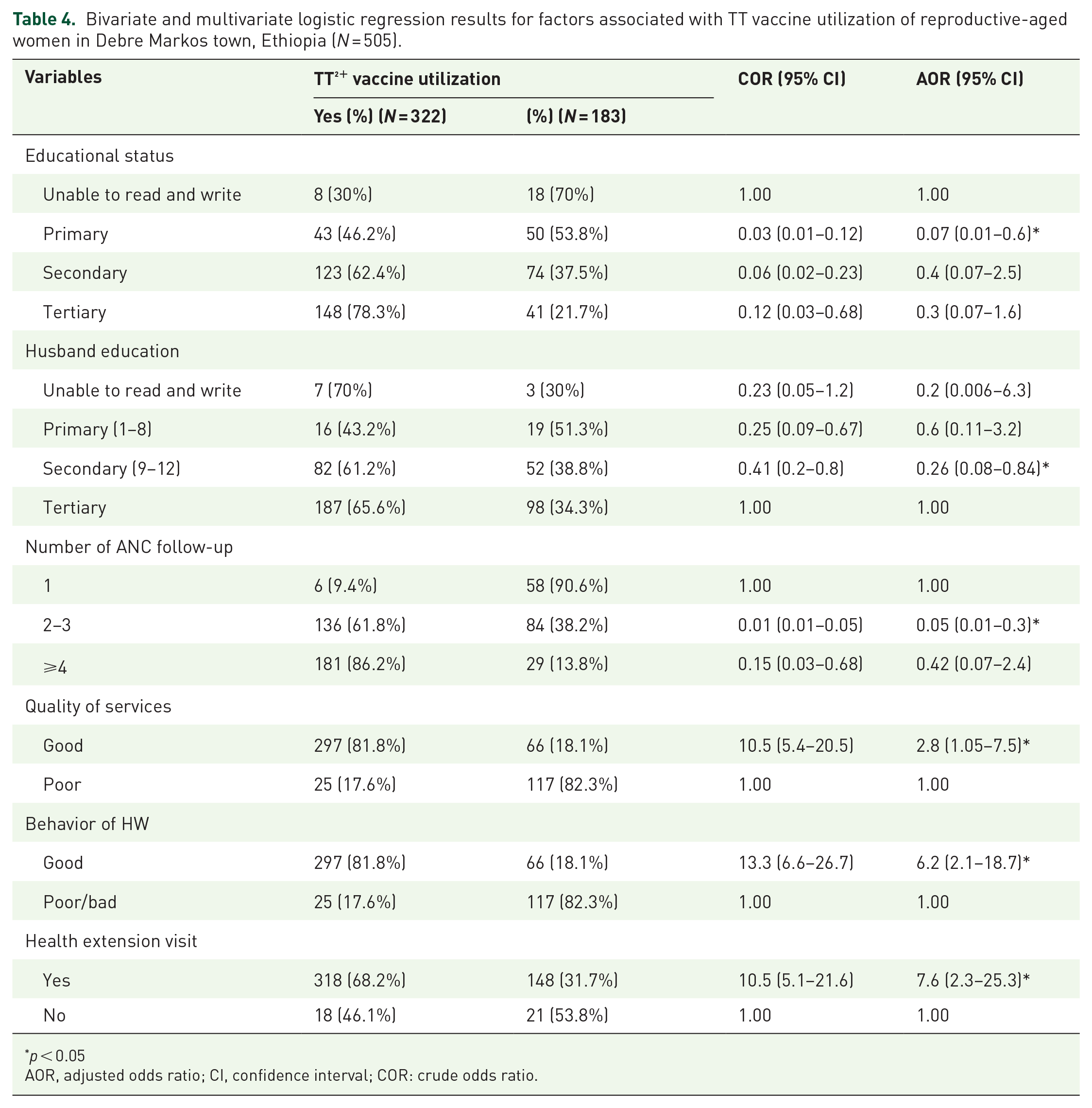
After controlling possible confounders in the multivariable logistic regression model, the mother’s and husband’s educational status, number of ANC visits, perceived quality of service, the behavior of health workers, traveling time to health facilities, and health extension visits were significantly associated with TT vaccine utilization. Accordingly, mothers who attended primary school were 7% less likely to be immunized TT vaccine than those who were uneducated (AOR: 0.07, 95% CI: (0.01–0.6)), p = 0.001]. Mothers whose husbands had secondary education were 26% less likely to receive two doses of TT vaccine than mothers whose husbands had higher education (AOR: 0.26, 95% CI: (0.08–0.84), p = 0.02). Mothers who had 2–3 times ANC follow-up in the last pregnancy were 5% less likely to have the odds of protective doses of TT vaccine than the congruent (AOR: 0.05, 95% CI: (0.01–0.3), p = 0.001). Mothers who receive a good quality of service were 2.8 times more likely to receive TT vaccine than the congruent (AOR: 2.8, 95% CI: (1.05–7.5), p = 0.04). Furthermore, participants who got the service from health workers with good behavior were 6.2 times more likely to receive the vaccine than their corresponding (AOR: 6.2, 95% CI: (2.2–19.2), p = 0.001). Finally, mothers who had visited with health extension workers were 7.6 times more likely to have TT vaccine utilization (AOR: 3.1, 95% CI: (2.3–25.3), p = 0.03; Table 4).
Bivariate and multivariate logistic regression results for factors associated with TT vaccine utilization of reproductive-aged women in Debre Markos town, Ethiopia (N = 505).
p < 0.05
AOR, adjusted odds ratio; CI, confidence interval; COR: crude odds ratio.
Discussion
This study revealed that the proportion of valid tetanus toxoid (TT + ) vaccination use was 71.2%. The result is consistent with that of western Cameroon and southern Ethiopia (72.5%, 71.9 and 72.78, respectively)16–18 but lower than the WHO target and Ethiopian Ministry of Health (90.0%), Pakistan (86.1%), Sierra Leone (81.6%), and Ivory Coast (81.97%).19–22 This result is higher than that of Ethiopian Demographic Health Survey of 2016 and other local reports in the Ethiopian regions and in Nigeria.14,10,19,23–25 Referring to measurement methods may be the possible cause of discrepancy in vaccine utilization coverage.3,10 Multivariate analysis model findings claimed that maternal educational level, husband’s educational level, number of ANC visits, quality of the provided health services, behavior of the health workers, and the health extension visit were significantly associated with sufficient utilization of TT vaccine. Consequently, mothers who attended primary school were 7% less likely to receive two doses of TT vaccine per injection than those who attended higher education (AC: 0.07, 95% CI (0.01–0.30)). This outcome is comparable to that of the study from different regions of Ethiopia and Nigeria.10,16,23–24,26 The result contrasts with a study conducted in Sierra Leone that states, that women with primary and higher education levels had lower odds of receiving TT immunization when compared to those with no formal education. 21 Easy communication between them can help healthcare providers to have a good approach and respect for educated mothers.10,20 Mothers whose husbands had secondary education were 26% less likely to receive two doses of TT vaccine than mothers whose husbands had higher education (AOR: 0.26, 95% CI: (0.08–0.84)). This finding is supported by a study conducted in Ethiopia.16,26 Therefore, effective decision-making with his spouse will assist in receiving the TT vaccine during pregnancy.
Mothers who attended 2–3 antenatal care visits were 5% less likely to receive two doses of TT vaccine injection compared to mothers who attended one antenatal care visit (AOR: 0.05, 95% CI (0.01–0.25)). This finding was supported by different studies conducted in Ethiopia, Sierra Leone, and Ivory Coast.3,10,19,21,22 In this study, valid TT vaccine utilization is 2.8 times more likely with mothers who perceived good quality services than the counter. The result is supported by a study conducted in Ethiopia. 3 A study conducted in developing countries concluded that the quality of care provided is vital to user confidence in the health system and a study conducted in Ghana showed that satisfaction with the service and treatment they receive affect TT vaccine utilization.27,28 The behavior of health workers was also a significant factor in receiving the recommended doses of the TT vaccine. This research demonstrated that health workers who behaved well had a six-fold higher chance of receiving the vaccine in at least two doses. This finding is supported by a study that stated, that effective communication with providers, demonstrating empathy and understanding is more likely to improve patient knowledge, health literacy, and shared decision-making, encouraging return visits. 27 Mothers do not complete the recommended vaccine, because they are dissatisfied with the services they have received for such reasons as rudeness on the part of the service provider.27,28 In another study, half of the unvaccinated women reported that health providers did not motivate them to receive the TT vaccine. 29 This study revealed that mothers who visited with extension workers during their pregnancy were seven times more likely to receive at least two doses of the TT vaccine that was congruent with the study conducted in Ethiopia. 16 According to theory, mother and newborn infections originate from not receiving the tetanus toxoid vaccination. Practically, tetanus toxoid immunization utilization will reduce maternal and neonatal infection, which is fatal for the mother and neonate, and in the public health aspect, it provides information about factors that contribute to utilizing the valid TT vaccine that can be worked on to minimize deaths from tetanus infection.
Conclusion
About 71.2% of study participants received the current TT vaccine during their previous pregnancy. This study tried to find factors that affect vaccine utilization and the most influencing factors in TT vaccine use were mothers’ low educational levels, husbands’ low educational level, 2–3 ANC visits during pregnancy, poor standard of healthcare service, improper actions of health professionals, and mothers’ visit with health extension staff. The government has to include the strategic direction at all levels and present it to all stakeholders and implementers.
Limitations of the study
Because of the drawback of the cross-sectional study design, the authors recommended that future researchers address this by using a different study design including a qualitative one.
Footnotes
Acknowledgements
The authors would like to acknowledge Addis Ababa University, College of Health Sciences, School of Nursing and Midwifery for small grant financial support during data collection, study participants, and Debre Markos town health bureau for the provision of support letter.