
Abstract
The success in preventing hepatitis B virus and human papillomavirus infections by means of vaccination paves the way for the development of other vaccines to prevent sexually transmitted infections (STIs) such as gonorrhoea, syphilis, chlamydia, herpes simplex virus, human immunodeficiency virus and Zika virus. The current status of vaccine development for these infections will be explored in this review.
The general principles for success include the need for prevention of latency, persistence and repeat infections. A reduction in transmission of STIs would reduce the global burden of disease. Therapeutic activity of vaccines against STIs would be advantageous over preventative activity alone, and prevention of congenital and neonatal infections would be an added benefit. There would be an added value in the prevention of long-term consequences of STIs. It may be possible to re-purpose ‘old’ vaccines for new indications. One of the major challenges is the determination of the target populations for STI vaccination.
Introduction
According to the World Health Organisation (WHO), there were estimated to be more than 1 million sexually transmitted infections (STIs) acquired every day worldwide in 2016, and each year there are an estimated 357 million new infections with one of four STIs: chlamydia, gonorrhoea, syphilis and trichomoniasis. 1 Furthermore, antimicrobial drug resistance, especially for gonorrhoea, is a major threat to the successful control of STIs.
There are possibilities for reductions in STIs:
Vaccination against Neisseria meningitidis serogroup B may offer a degree of protection against Neisseria gonorrhoeae.
Candidate vaccines against syphilis, chlamydia, herpes simplex virus (HSV) and human immunodeficiency virus (HIV) are under development.
Zika virus candidates are under development in the context of outbreak preparedness, the prevention of mosquito and sexual transmission, and the prevention of congenital infections.
Mechanisms of natural immunity and immune correlates of protection
Repeated gonorrhoea infections are common and can occur with the same strain or serotype, and the inability of natural infection to induce long-lasting immunity hinders the development of vaccines against gonorrhoea. 2 Regarding syphilis, little is known about the correlates of immunity in humans and it is well recognised that individuals who acquire syphilis can be re-infected following treatment, and that this cycle can be repeated many times. 3 At most, there may be a degree of partial protection following chlamydia infection. 4 But, in general for STIs, natural infection does not generally protect against subsequent infections, and recurring infections are a feature.
Regarding the usefulness of immune correlates of protection, attempts to identify such correlates for HIV infection point to a broader repertoire of immune activation than simply antibody responses.5,6 There is no ideal animal model for studying sexually transmitted diseases, although the cotton rat, for example, has proved useful in the study of genital herpes simplex virus infection, 7 and the nonhuman primate model is useful for studying HIV infection and acquired immunodeficiency syndrome (AIDS). 8
Gottlieb and Johnston provide a very helpful guide with respect to clinical trials and the development of vaccines against sexually transmitted diseases (see Table 1). 9
Roadmap for facilitating clinical evaluation and vaccine introduction. 9

HIV, human immunodeficiency virus; HSV, herpes simplex virus; STI, sexually transmitted infections.
Issues related to the development of vaccines against STIs
The preventable burden of bacterial and viral STIs is difficult to estimate. The causes of this uncertainty range from the reluctance of some individuals to seek diagnosis and treatment, asymptomatic infections rendering the individual unaware that they are infected, latency and persistence of infection, diagnostic tests not being performed and the over-use of antibiotics. These very reasons also help explain why clinical trial design for vaccines against STIs is problematic, and why target populations for vaccine implementation, once STI vaccines are licensed, are ill-defined.
As will be seen below, there is some progress in the development of vaccines against STIs that may have both preventative and therapeutic activity. The design of a clinical trial to test both preventative and therapeutic qualities of an STI vaccine would be based on the premise that the status of the subjects is known at the beginning of the trial, to distinguish infected from non-infected individuals. Such a dichotomy may not be easy to establish. It may be preferable to perform one trial in infected individuals and another in non-infected individuals. Some of these dilemmas will be explored below.
Gonococcus
Burden of disease
The WHO estimated the global prevalence and incidence of gonorrhoea in 2016. 10 The 2016 global prevalence estimate for gonorrhoea in women was 0.9% (95% uncertainty interval 0.7–1.1) whereas in men it was 0.7% (95% uncertainty interval 0.5–1.1). There were 86.9 million total estimated incident cases of gonorrhoea globally (95% uncertainty interval 103.4–231.2 million).
Pre-clinical vaccine development
Lipooligosaccharide being the most abundant molecule expressed on the gonococcal surface and contributing significantly to pathogenesis, is an obvious target for vaccine development. 11 The promising candidate known as TMCP2 has been shown to elicit bactericidal IgG, and reduced colonisation levels of gonococci in experimentally infected mice whilst also accelerating clearance by each of two different gonococcal strains. Other approaches in pre-clinical development include outer membrane vesicles (see below) and purified protein subunit vaccines 12
MeNZB™
Bioinformatic analysis has been performed to assess the similarity of a prototype Neisseria meningitidis serogroup B vaccine known as MeNZB™ OMV (outer membrane vesicle) and antigens from a four-component N. meningitidis serogroup B vaccine known as Bexsero®, to gonococcal proteins. 13 Rabbits were immunised with the OMV component or three recombinant antigens of Bexsero®, and western blot and enzyme-linked immunosorbent assay (ELISA) were used to assess the generation of antibodies recognising Neisseria gonorrhoeae. Serum from humans immunised with Bexsero® was investigated to assess the nature of the anti-gonococcal response. There was found to be a high level of sequence identity between MeNZB™ OMV and Bexsero® OMV antigens and gonococcal proteins. Bexsero® induced antibodies in humans that recognise gonococcal proteins.
During and after the use of MeNZB™ in New Zealand during a meningococcal outbreak between 2004 and 2006, there was observed to be a simultaneous decline in reported cases of gonorrhoea. 14 Figure 1 shows the impact of MeNZB™ on gonorrheal infections in three regions of New Zealand arising from the use of MeNZB™ during 2004–2006. 15 No other STIs described in national surveillance reports declined during this period.

Gonorrhoea rates per 100,000 population in selected New Zealand regions, 1998–2014.
The anti-gonococcal antibodies induced by MeNZB-like OMV proteins could explain the previously seen decrease in gonococcal cases following MeNZB vaccination. 13
Modelling
To explore the potential impact of vaccination against N. meningitidis on N. gonorrhoeae in the United States (US), a decision-analysis modelling exercise was performed. 16 The authors modelled the theoretical impact of a US four-component N. meningitidis serogroup B (4CMenB) vaccination programme on gonorrhoea outcomes. A decision-analysis model was populated using published healthcare utilisation and cost data. A two-dose adolescent vaccination campaign was assumed, with protective immunity starting at age 15 years and an assumed base-case efficacy against gonorrhoea of 20%. One of the key outcome measures was a reduction in gonorrhoea and HIV infections.
The model predicts that without vaccination, a theoretical US adolescent cohort would experience 844,000 gonorrhoea infections (95% credible interval 439,200–1,399,000) over a lifetime. 16 Without vaccination, gonorrhoea infections would increase the number of HIV cases by 557. The model also predicts that adolescent vaccination with 4CMenB would prevent 83,167 (95% credible interval 44,600–134,6000) gonorrhoea infections and decrease the number of HIV infections by 55 (95% credible interval 2–129) per vaccinated birth cohort in the USA. The authors conclude that, even with a low effectiveness against gonorrhoea, for example 20%, a US vaccination programme against serogroup B meningococcal disease using 4CMenB would substantially reduce the number of gonorrhoea infections.
Challenges and next steps
An understanding of how Neisseria meningitidis group B OMV vaccines work against Neisseria gonorrhoeae could enhance the development pathways of vaccines against gonorrhoea. 17
The challenges of vaccine development for gonorrhoea are highlighted in Table 1 and include the use of human challenge models. The next step for this field is to await the results of studies using 4CMenB against gonorrhea and other OMV-based vaccines.17–19
Syphilis
Burden of disease
The WHO estimated the global prevalence and incidence of syphilis in 2016. 10 The 2016 global prevalence estimate for syphilis in women was 0.5% (95% uncertainty interval 0.4–0.6), whereas in men it was 0.5% (95% uncertainty interval 0.4–0.6). There were 6.3 million total estimated incident cases of syphilis globally (95% uncertainty interval 5.5–7.1 million).
Pre-clinical vaccine development
A prototype syphilis vaccine was developed by James Miller as early as 1973. 20 The difficulties ahead are foretold in his conclusion: ‘Conclusive evidence that Treponema pallidum immobilization (TPI) antibody is not associated with the immune response was provided by the finding that 8 of the 11 immune rabbits challenged 1 year after vaccination had no TPI antibody before challenge and failed to develop immobilizing antibody during the 3-month period of observation after challenge’. Nevertheless, the experiment was successful in that rabbits immunised with a non-infectious ʏ-irradiated T. pallidum were completely protected against disease for at least 1 year in the face of T. pallidum infectious challenge.
Possible targets include selected subsets of the T. pallidum repeat (Tpr) protein family (targeting susceptibility and persistence), and the treponemal adhesin protein pallilysin Tp0751 (targeting dissemination).21,22 A novel approach has been the use of non-infectious Borrelia burgdorferi as an effective carrier to deliver and elicit a specific host response to T. pallidum antigens such as those expressed by tp0897 (tprK) and tp0435 genes. 23 Plasmid DNA encoding T. pallidum flagellin FlaB3 has been used as a candidate vaccine for the evaluation of immunogenicity and protection against dissemination. 24 Subsequent intradermal challenge in rabbits showed a significant reduction in the bacterial burden in blood, liver, spleen and testicles in the rabbits vaccinated with plasmid DNA-encoded flagellin (FlaB3).
Table 2 shows the key issues and implications that need to be considered during the pre-clinical development phase of candidate syphilis vaccines.
Key issues needing to be assessed during the process of syphilis pre-clinical vaccine development.

HIV, human immunodeficiency virus.
Challenges and next steps
Because syphilis transmission occurs by contact with the infectious primary chancre or through secondary lesions, prevention or attenuation of these lesions is a necessary requirement for a syphilis vaccine, according to a recent review of the subject by Caroline Cameron. 25 This is because of the need for such a vaccine to either eliminate, or at least reduce, person-to-person transmission. It is also necessary for the vaccine to prevent dissemination of the organism within the infected host, repeat infections, persistence and latency.21,22
Once a suitable candidate or candidates are identified, it will be time to move to the clinical phase of testing in humans. However, with the cloud of the Tuskegee Study, in which the subjects were not informed as to the true purpose of the study and in which subjects with syphilis were not treated, there will be ethical questions related to safety and treatment to be answered before clinical trials begin. 26
Chlamydia
Burden of disease
The WHO has estimated the global prevalence and incidence of chlamydia in 2016. 10 The 2016 global prevalence estimate for chlamydia in women was 3.8% (95% uncertainty interval 3.3–4.5) whereas in men it was 2.7% (95% uncertainty interval 1.9–3.7). There were 127.2 million total estimated incident cases of chlamydia globally (95% uncertainty interval 95.1–165.9 million).
Pre-clinical and clinical vaccine development
Data related to protective immune responses at the cervical mucosa, that could potentially limit chlamydia infection and reinfection, have been used to inform vaccine approaches and biomarkers. 27 It was found that cytokines involved with humoral type 1 interferon and Th17 responses are associated with susceptibility to Chlamydia trachomatis whilst cytokines involved in Th1 polarisation, recruitment and activation are associated with protection against ascension and reinfection.
Trials in mice and koalas indicate that the major outer membrane protein (MOMP) is a highly recognised antigenic target and may be preferable to whole cell targets, which have their limitations. 28 Whilst sterilising immunity is the ultimate goal, vaccine-induced partial immunity preventing upper genital tract infection and inflammation may be cost-effective when compared with current screening and treatment strategies. 29 Current vaccine candidate development is shown in Table 3. 30
Current Ct vaccine candidate development. 30

CDC, Centre for Disease Control; Ct, Chlamydia trachomatis; MOMP, major outer membrane protein; NIH, National Institutes of Health; NIAID, National Institute of Allergy and Infectious Diseases; pmps, polymorphic membrane proteins; UV, ultra violet.
Challenges and next steps
The conclusions and recommendations of a National Institute of Allergy and Infectious Diseases workshop entitled ‘Chlamydia vaccines: the way forward’ highlight some of the challenges in chlamydia vaccine development. Zhong et al. state: 39
● Although preliminary modelling suggests that even a partially protective C. trachomatis (Ct) vaccine may be cost-effective, more data are needed regarding progression of Ct infection to upper genital tract sequelae and burden of Ct-associated disease, especially in lower- and middle-income countries, to define better the potential worldwide impact of a Ct vaccine.
● Clinical testing of a Ct vaccine is feasible; however, choice of clinical trial endpoints warrants further investigation and discussion. Blood biomarkers and other novel approaches for identifying upper genital tract infection and inflammation in women would be useful for defining endpoints for vaccine efficacy studies as well as disease burden.
● Although the immunological basis for protection from Ct infection and disease has been well studied, key issues such as the role of antibody still need to be clarified. A relative consensus was reached that putative Ct vaccines should generate Ct-specific CD4 T cells targeting genital epithelial cells, combined with a strong antibody response.
● Further analysis is needed on the utility of several mouse models available to test candidate vaccines. Harmonization these models such that candidate vaccines can be compared across laboratories with respect to important clinical endpoints of product indications would be valuable.
● Although intramuscular immunization has worked effectively for preventing cervical human papillomavirus infection, it is unclear whether a Ct vaccine can be similarly administered to achieve protection, given the need for robust local T call immunity. An effective Chlamydia vaccine may need to induce strong transmucosal immunity with resident memory T cells in the genital tract
Self-adjuvanting biodegradable nanoparticles may be an option for Ct vaccine delivery. 40
HSV
Burden of disease
The WHO has estimated the global prevalence and incidence of herpes simplex virus type 2 infection. 41 The estimated number of individuals aged 15–49 years who were living with herpes simplex virus type 2 infection worldwide in 2003 was 536 million, or roughly 16% of the world’s population in this age group.
Pre-clinical vaccine development
Pre-clinical development of HSV vaccines utilises well-established animal models to test and screen promising candidate vaccines. 42 The mouse model unfortunately does not recapitulate human infection, because genital reactivation does not occur and mortality is high in initial infection. The guinea pig model mimics infection in humans although promising vaccines in guinea pigs have not translated into efficacious vaccines in humans. Candidates in pre-clinical development include: a trivalent glycoprotein (gD/gC/gE), a live-attenuated vaccine, mutated HSV-1 and HSV-2, an inactivated HSV-2 in MPL/alum, an HSV-1 glycoprotein B lentiviral vector and an intranasal recombinant HSV-1 gB vaccine.
An early HSV type 2 vaccine, whilst shown to induce high levels of neutralising antibodies, nevertheless did not exhibit protection against HSV type 2 infection. 43 A possible explanation for this lies in the ability of HSV to become latent and to reactivate. 44 Further experiments with plasmid DNA encoding full-length glycoprotein D from HSV type 2 (gD2), secreted gD2 or cytosolic gD2, when evaluated in mice and guinea pigs, whilst showing some evidence of reduction of acute disease and subsequent recurrent disease, neither resulted in improved virus clearance from the inoculation site nor significantly reduced recurrent disease when used as a therapeutic vaccine. 45 HSV vaccine under development are shown in Table 4. 46
HSV candidate vaccines in development. 46

HSV, herpes simplex virus.
More recently, intramuscular vaccination with a live-attenuated HSV vaccine (VC2) was shown to stimulate vaginal IL-17A dependent antimicrobial peptide immune responses in a guinea pig model of genital HSV type 2 infection. 47 The live-attenuated virus had been engineered with disabling mutations in the protein that otherwise allows the virus to enter axons. The responses were described as robust and protective of animals from acquiring any appreciable disease after exposure to a highly virulent HSV type 2 strain.
Clinical vaccine development
The candidate GEN-003 therapeutic bivalent subunit vaccine for HSV type 2 has been shown to be clinically effective at doses of 60 µg/50 µg and 60 µg/75 µg in reducing viral shedding for up to 1 year in adults with symptomatic genital HSV type 2 infection.48,49 Lesion rate reductions were also observed at between 31% and 69%, although lesion rates also decreased in the placebo arm at 62%.
Controversies and next steps in herpes simplex virus vaccine development
HSV vaccine development has not been without controversy. 50 It was reported in 2018 that a US professor had injected individuals with his experimental live HSV type 2 vaccine, which had not been cleared from the regulatory viewpoint and which he administered without the necessary safety precautions.
One promising approach uses a vaccine to prime (with a subunit HSV vaccine) and a chemo-attractant (intravaginal/topical imiquimod) to pull immune cells into the genital tract, the so-called prime and pull strategy, which shows that the strategy is able to decrease recurrent HSV more effectively than vaccine alone. 51
HIV
Burden of disease
The WHO states that, since the beginning of the HIV/AIDs epidemic, 75 million people have been infected with HIV and approximately 32 million have died as a result of HIV. 52 Furthermore, globally there were estimated to be 37.9 million people (95% confidence interval 32.7–44.0 million) living with HIV at the end of 2018 and an estimated 0.8% of adults aged 15–49 years are thought to be living with HIV.
Progress of vaccine development to date: pre-clinical and clinical
Some examples of HIV vaccine candidates under pre-clinical and early clinical development are shown in Table 5.
Examples of HIV vaccine candidates under pre-clinical and early clinical development.
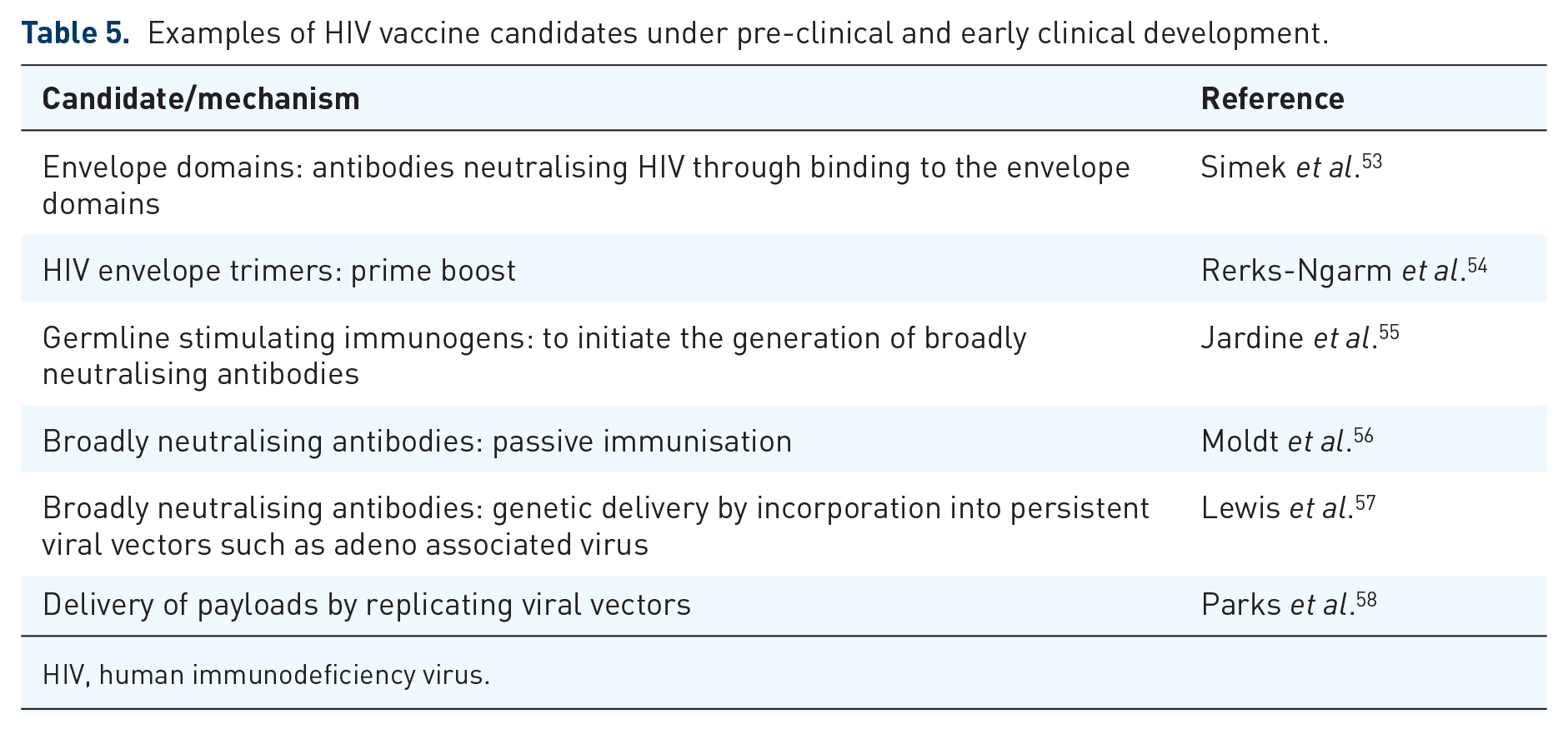
HIV, human immunodeficiency virus.
A vaccine that had therapeutic as well as preventative properties could be a worthwhile approach. The following are some examples of therapeutic vaccine trials currently underway:
● Profectus BioSciences: an exploratory randomised, 2-arm (1:1), double-blind, placebo-controlled trial evaluating the safety and efficacy of an HIV-1 multi-antigen plasmid DNA (HIV-MAG pDNA) vaccine prime in combination with an interleukin-12 plasmid DNA (IL-12 pDNA) adjuvant delivered by in vivo electroporation followed by a recombinant vesicular stomatitis virus vector containing the HIV-1 gag gene (rVSV HIV gag) booster vaccine in subjects on combination anti-retroviral therapy (cART) who started therapy during acute or early HIV infection. 59
● National Institute of Allergy and Infectious Diseases (NIAID): evaluation of the use of ALVAC vCP1452 vaccine in combination with IL-2 to increase HIV-specific immune responses in HIV-infected patients. ALVAC vCP1452 vaccine is a recombinant canarypox HIV vaccine that is administered as a monthly intramuscular injection. The IL-2 is self-administered as a daily subcutaneous injection at a low, non-toxic dose (2 million units). 60
● Sharon Ridler (University of Pittsburgh): evaluation of an investigational dendritic cell HIV vaccine made from a person’s own white blood cells. 61
● NIAID: an open label study to evaluate safety, tolerability, and immune response of a six-plasmid multiclade HIV-1 DNA vaccine, VRC-HIVDNA016-00-VP. The hypothesis is that this regimen will be safe for human administration and elicit immune responses to HIV-1 clade B Gag, Pol and Nef proteins, as well as clades A, B and C Env proteins. The primary objective is to evaluate the safety and tolerability in humans of the investigational vaccine and secondary objectives are to evaluate the immunogenicity of the vaccine as measured by intracellular cytokine staining (ICS) in the 4 weeks after the second or third dose of vaccine and the social impact of participating in an HIV-1 vaccine trial. 62
NIAID: comparison of the safety, tolerability and immunogenicity of CH505TF gp120 produced from stably transfected cells to CH505TF gp120 produced from transiently transfected cells in healthy, HIV-1-uninfected adult participants. 63
GlaxoSmithKline (GSK): study designed to determine whether administration of the GSK Biologicals HIV vaccine 732462 can lead to a reduction in viral load, and impact on the course of human immunodeficiency virus type 1 (HIV-1) infection. In HIV-1 infected persons who have not yet started antiretroviral therapy (ART), such a vaccine would potentially lead to a delay in the initiation of treatment. 64
NIAID, University of California (Los Angeles), Inovio Pharmaceuticals: safety, immunogenicity and anti-reservoir activity of an electroporation-administered HIV DNA vaccine encoding GAG, POL and ENV proteins with IL-12 plasmid in HIV-infected adults on anti-retroviral therapy. 65
● NIAID: a rollover study of those who participated in study A5058s: now a phase II trial to evaluate the ability of vaccine-induced helper and CTL responses to control viremia in the absence of anti-retroviral therapy. 66
● French National Institute for Health and Medical Research-French National Agency for Research on AIDS and Viral Hepatitis (Inserm-ANRS): EVHA T01 is an international, phase I/II, multicentre, multi-stage, double-blind study that will evaluate at least three experimental arms compared with placebo control in HIV-1 infected participants to see if one or more has a clinically relevant impact on the control of viral replication. The three interventions are: GTU-multiHIV B-clade vaccine plus MVA HIV-B HIV vaccine; GTU-multiHIV B-clade vaccine plus MVA HIV-B HIV vaccine plus vedolizumab; vedolizumab. 67
There are open questions regarding therapeutic HIV vaccines: would the same vaccine serve for prevention of both sexual and maternal transmission, would the same vaccine serve for both developing and developed countries, would a therapeutic vaccine be limited to those with anti-retroviral failure, would a therapeutic vaccine decrease transmission?
Ongoing phase IIb/III trials
Using the vaccinia vector with insertion of the HIV envelope protein gp160, the first phase I human vaccine trial was performed in France in 1986. 68 This did not demonstrate efficacy against HIV. A degree of efficacy was not demonstrated until 2009 in the phase III RV144 trial. 54 This consisted of a priming with a canarypox vector (containing gag, pol and nef genes) followed by a boost with gp120, and demonstrated an efficacy of 31%. Since then, this approach continues to be explored. Meanwhile, the only other approach under consideration uses a mosaic vaccine candidate. 69 This involves a public–private partnership with Janssen, the NIAID of the NIH, the HIV Vaccine Trials Network, and the US Army Medical Research and Development Command. One important aim of this mosaic approach is to address the global genetic diversity of HIV.
Challenges of vaccine development
The advent, deployment, uptake and impact of anti-retroviral medications is changing the HIV landscape, especially by dramatically reducing sexual transmission.70,71 Maternal transmission to the unborn baby is also potentially completely controllable with these medications, and this in turn has future positive implications for sexual transmission by the time these infants reach adulthood. 72
In this context, is there a need for an HIV vaccine? If one were available, to whom would it be administered? What efficacy would be acceptable? Would its use detract from the successful use of anti-retroviral medications?
Next steps
The next steps involve progressing both vaccine approaches: the prime-boost approach and the mosaic approach, completing further clinical trials, deciding what would be an ‘acceptable’ efficacy, and planning how to distribute a successful vaccine to those who need it the most.
Zika virus
Burden of disease
At the beginning of 2020, Zika virus is quiescent; the current burden is the large cohort of infants who were infected maternally in 2015–2017. 73
Progress of vaccine development to date
Whilst being transmitted by mosquitos, Zika virus is also established as a sexually transmitted infection, 74 and Zika virus RNA has been demonstrated to be commonly present in the semen of males with symptomatic Zika virus infection, with persistence in some for more than 6 months. 75 Zika virus vaccines under development are summarised in Table 6 (WHO 2019). 76
Zika virus vaccines under development (WHO). 76

MV, measles virus; PIV, purified inactivated virus; PIZV, purified inactivated Zika vaccine; prME, pre-membrane and envelope ; WHO, World Health Organisation; ZIKV, Zika virus.
Challenges and next steps in vaccine development
Whilst there is a healthy Zika virus vaccine pipeline, questions over the precise role of such a vaccine remain. Would the main purpose be to prevent vector-borne Zika virus infection, or sexually transmitted Zika virus infection, or both? Would it be used in routine vaccination or reserved for use in outbreaks? And more fundamentally, can a correlate of protection be developed and what is the best development pathway?
The development of vaccines able to prevent both vertical transmission and congenital Zika virus syndrome is challenging, and clinical trials for testing vaccine efficacy in relation to foetus protection are going to take time. 77
Delivery of protection against STIs
How will it be possible to deliver protection to those at risk of STIs, to target populations most in need? The first clue lies in HIV, with the facilitation of testing in hard-to-reach groups. 78 Programmes like this could readily be adapted to vaccination rather than testing. The next clue lies in the need for education and raising of awareness in ‘implementers’ of progammes. 79 Programmes for education and raising awareness have a universal relevance to vaccination against all forms of sexually transmitted infections. The third clue lies in being capable of rapidly measuring the impact and success of a vaccination programme against STIs. 80
The predicted levels of coverage required for protection by putative vaccines against the STIs gonorrhoea, syphilis, chlamydia, herpes simplex virus, human immunodeficiency virus and Zika virus vary widely according to epidemiology, burden of disease, extent and frequency of transmission, silent infection, ability to cause repeated infections and of course the quality of the vaccine response, and no one model can be applied. In an outbreak situation such as occurred with Zika virus, it is likely that high coverage levels would be required. For maternal transmission, then the coverage could potentially be more targeted. And for sometimes silent and often common infections, universal coverage would be ideal.
Could delivery of vaccines against STIs be performed in a cost-effective way? Based on current delivery models for human papillomavirus vaccine and current screening for STIs, and taking account of regional incidence data, the conclusions of a large costing study are that increased investment and innovative financing are required, especially in low- and middle-income countries, and that there is a need for synergising with other health programmes. 81 And the conclusion of a cost-effectiveness study into a Ct vaccination programme in the US is that it would result in increased costs to the healthcare system but with the benefit of significantly averting morbidity and mortality. 82
Conclusion
Whilst there are considerable costs associated with (i) further research and development into vaccines against STIs and (ii) their future delivery and deployment, nevertheless, in the context of antimicrobial resistance and the potential for resistance against anti-virals, and the potential benefits, further investment in vaccines against STIs is warranted.
Roadmap: general principles
1) Need for prevention of latency, persistence and repeat infections;
2) Reduction in transmission of STIs would reduce the global burden;
3) Therapeutic activity advantageous over preventative activity alone;
4) Prevention of congenital and neonatal infections also an added benefit;
5) Added value of the prevention of long-term consequences of STIs;
6) It may be possible to re-purpose ‘old’ vaccines for new indications;
7) Challenge of determining the target populations for STI vaccination
Footnotes
Conflict of interest statement
EDG McIntosh is an employee of Merck Sharp & Dohme (MSD), which manufactures vaccines. The views expressed herein are his own and do not necessarily reflect the views of Imperial College or MSD.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.